Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back
|
Describe carcinoma of the penis
|
1) Uncircumscribed men, poor hygeine, smoking, HPV
2) Begins as CIS (Bowen's disease in adults). Restricted to epithelium, BM intact 3) Squamous cell carcinoma is crusted grey ulcerated papules of the glans which can affect the inguinal lymph nodes and metastasize |
|
|
What are the 3 penile congenital anomalies
|
1) Hypospadias (ventral, aborted development of corpus spongiosum, often associated with cryptorchidism)
2) Epispadias (dorsal, bladder formation abnormality) 3) Phimosis but more commonly due to poor hygeine of uncircumcised penis. Risk of developing Bowen's disease, erectile dysfunction and vascular insufficiency. |
|
|
What are 4 important epidermal lesions of the penis
|
1) Condyloma avvuminata (genital warts) - benign or cancerous depending on strain of HPV
2) Squampous cell carcinoma in-situ (paeds) 3) Bowen's disease due to poor hygeine and smegma toxins 4) Malignant SCC |
|
|
What are the histological features of penile SCC
|
Keratin pearl surrounded by malignant epithelial cells and lymphocytes
|
|
|
What are the complications of cryptorchidism
|
Trauma and temperature causing
1) sterility 2) lack of androgen production 3) testicular atrophy 4) testicular cancer, bilateral risk |
|
|
What are the aetiologies of testicular atrophy
|
1) atherosclerosis
2) inflammatory orchitis (usually infection) 3) hypopituitarism (eg androgen, anabolic steroid supplementation) |
|
|
A patient presents with enlarged testes. What are the DDx and what additional info is needed
|
Chronic: Hydrocoele is not painful and transilluminates. Other "coeles" don't transilluminate. Haematocoele may be acute and associated with trauma.
Testicular tumour is non-acute and not painful Acute (painful) testicular torsion of epididymo orchitis. Need Hx of past episodes of torsion, cremasteric reflex and U/S For orchitis need sexual Hx ( STI by chlamydia or gonnorrhoea) and discharge (puss, clear, blood) plus pain and possible systemic symptoms. |
|
|
A patient with a palpable mass in his teste is likely to have a tumour. What types of primary are there?
|
Germ cell (carcinoma in situ, seminoma, teratoma, yolk sac, choriocarcinoma)
Sex cord stromal (leydig, sertoli, mixed) |
|
|
Describe the aetiology of the most common seminomatous germ cell tumours
|
GS neoplasia arises from intratubular germ cells.
Seminoma most common cancer of tests. 30-40YO. Bulky homogenous mass, no necrosis or haemorrhage. Rapidly grows and metastasises to lungs but sensitive to chemo and radiation. bHCG and LDH are markers |
|
|
Describe non-seminomatous germ cell tumours
|
1) Embryonal carcinoma: 20-40YO with necrosis and haemorrhage. No serum marker (Dx by exclusion and histology)
2) Yolk Sac: Most common tumour up to 3YO. Dx by AFP. Curable in infants 3) Choriocarcinoma: highly malignant, small primary, rapid haematoginous spread. HCG is serum marker. 4) Teratoma: large, heterogenous made up of normal, embryonic or foetal tissue. Benign in infants but malignant in children. No markers. |
|
|
A 24 YO sexually active male suffers from epididymo ochhitis. What is the likely organism. What id he was 65
|
<35YO - chlamydia, gonnorhoea
>45YO - extension of UTI caused by E.coli, Pseudomonas |
|
|
How is prostate cancer graded
|
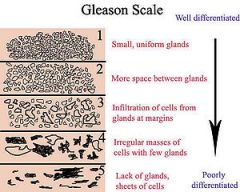
Gleeson score from 2 areas of the biopsy with neoplasia. Score based on glands and cellularity
|
|
|
What are the possible ways endometrial tissue disseminates to other parts of the body
|
1) Regurgitation - retrograde menstruation through the fallopian tubes deposits endometrial tissue into the abdomen
2) Coelomic metaplasia - peritoneal metaplasia of undifferentiated embryonic cells into endometrium 4) Via lymphatics and blood vessels |
|
|
What are common sites of endometriosis
|
Ovaries, uterus, fallopian tubes, colon and appendix.
|
|
|
What is the condition of endometrium deep in the myometrium. What are the symptoms and signs
|
Adenomyoma
1) Severe menstrual pain 2) Enlargement of uterus up to 4x mass |
|
|
What are the sites of an ectopic pregnancy
|
Fallopian tube
Ovary Abdomen |
|
|
What are the symptoms or signs of an ectopic pregnancy and what risk factors are usually associated?
|
Pain in right iliac fossa or massive haemorrhage. Risk factors are:
Salpingitis, PID, age, adhesions, endometritis, smoking, past Hx of ectopic |
|
|
What follow up should be done following an STI diagnosis
|
Screen for other STI's, particularly HIV (10x risk)
Contact tracing |
|
|
What are the risk factors for STI
|
Low socioeconomic status (homelessness, poverty)
Poor access to services (rural remote, indigenous) Body image (teenagers developing, negative image) IV drug use Mental illness, developmental disorders MSM |
|
|
What are the consequences of STI's
|
Mortality and morbidity
Infertility Vertical transmission HIV risk |
|
|
What are common symptoms of Clamydia in men
|
Discharge: watery, milky after several weeks
LGV: Proctatitis (DRE tenderness) with lymph node enlargement (common in MSM) |
|
|
What are the signs and symptoms of gonnorhoea in men
|
1) Copious prurulent urethral discharge
2) Intense dysurea within 2-8 days |
|
|
What are the sites of gonnorhoea infection
|
Urethra
Rectum Pharynx Conjunctiva Cervix Dissemination and sepsis |
|
|
Describe the epidemiology and aetiology of syphylis
|
1) Mostly MSM but spans all ages to 75+
2) Painless chancre is highly infective 3) High in indigenous 4) Oral, vaginal, anal and dermal transmission common |
|
|
How is syphilis diagnosed
|
1) PCR of chancre swab in 1st deg disease
2) Serology in 2 deg disease |
|
|
What strains of HPV are targeted by Gardisil and how are men protected
|
1) HPV 6, 11 (benign) and 16, 18 (oncogenic)
2) Herd immunity |
|
|
What are the infective disorders of the Fallopian tubes? complications?
|
1) Pyosalpynx caused by gonnorhoea, chlamydia, staph, strep, coliforms due to salpingitis, IUD, abortion, products of conception
2) Hydrosalpynx: fusion of fimbriated end following PID 3) Salpingitis 4) Complications: oophoritis, endometritis, ovarian abcess, hydrosalpynx, pyosalpynx |
|
|
What are the benign ovarian cysts
|
Functional:
Cystic follicle (< 2mm) Follicular cyst (> 2mm anovulatory). Luteal cysts (persistent corpus luteum) Non Functional: endometrioid cystic teratoma |
|
|
What are the 4 diagnostic criteria of PCOS
|
1) Polycystic ovaries (strings of pearls)
2) Hyperandrogenism: hirsutism, male-pattern balding, acne 3) obesity and insulin resistance 4) menstrual abnormality |
|
|
Describe the pathogenesis of PCOS
|
1) Increased frequency and amplitude of LH due to hyperinsulinaemia (insulin resistance) resulting in
2) Theca cell hyperplasia resulting androgen overproduction 3) Granulosa cell defect causing excess oestrogen secretion and endometrial hyperplasia or, alternately, exogenous oestrogen production from excess androgens due to obesity |
|
|
What are the 3 classes of ovarian tumours
|
1) Epithelial
2) Germ cell 3) Sex cord stromal |
|
|
What are the classifications of ovarian epithelial tumours
|
Serous (cuboidal cells with cilia) and mucinous (columnar) which can be:
1) Benign (1 layer) 2) Borderline (> 1 layer with structural complexity. Can implant in the abdoment) 3) Invasive: invades the stroma |
|
|
What are the 3 epithelial tumours of the ovary
|
1) Serous adenoma
2) Mucinous adenoma 3) Invasive adenocarcinoma |
|
|
What surface epithelial carcinoma of the ovary in young patients is associated with endometriosis
|
Endometrioid carcinoma of the ovary
|
|
|
What are the 4 germ cell tumours of the ovary
|
1) Teratoma
2) Choriocarcinoma 3) Dysgerminoma 4) Yolk sac tumour |
|
|
What are 4 clinical signs of a possible germ cell tumour
|
1) Dysmenorrhoea or precocious puberty due to increased hcg (choriocarcinoma)
2) Abdominal distension due to mass and/or ascites 3) Pain due to possible torsion 4) Symptoms of pregnancy (nausea, breast enlargement) |
|
|
What are the 3 types of teraoma
|
1) Mature (contains mature tissue - benign)
2) Immature (1% go on to become SCC) 3) Stuma ovarii - thyroid tissue causing hyperthyroidism. Can develop thyroid cancer. |
|
|
What cancer is like a seminoma
|
Dysgerminoma
|
|
|
What type of ovarian cancer is found in children and how is it diagnosed
|
Yolk sac - alpha-FP
|
|
|
How does gestational choriocarcinoma arise
|
Generally from a complete hydatidform mole
|
|
|
Describethe aetiology of the 2 types of hydatidform mole
|
1) Complete: egg loses DNA and is fertilised by one sperm. DNA replicates forming diploid, but paternally derived and non viable conceptus but placenta forms. Can become malignant (gestational choriocarcinoma from trophoblast cells)
2) Partial: 2 sperm fertilise the egg (triploid, quadriploid) |
|
|
What are the sex cord stromal tumours
|
Granulosa-theca cell (high oestrogen; precocious puberty, oligomenorrhoea with menorrhagia, post menopausal bleeding)
Sertoli-leydig cell tumours (androgens), masculinisation, precocious puberty, delayed puberty and virilisation in girls |
|
|
What syndrome, involving the abdomen and thorax is caused by an ovarian fibroma
|
Dissemination of an ovarian fibroma into the peritoneum and pleura results in Meigs syndroms: ascites, right sided pleural effusion and pain
|
|
|
What type of metastatic cancer forms in the ovaries arising from the GI tract and breasts
|
Krukenberg tumour: bilateral tumours of the ovaries from gastric adenocarcinoma and metastatic BC
|
|
|
List 3 categories of vulval pathology
|
1) Infective: HSVI and II, HPV (condyloma), trichomoniasis vaginalis, chlamydia, gonorrhoea, staph and strep
2) Obstructive: Bartholin gland cyst 3) Tumours: dysplastic (binucleated cells) condyloma -> VIN (vulval intraepithelial neoplasia) -> SCC Melanoma and other skin cancers (BCC) Extramamillary Paget's Disease |
|
|
Why are young women at risk of developing cervical cancer
|
After puberty, columnar epithelium shifts transformation zone to exocervix, highly mitotic due to vaginal acidity and prone to infection by HPV.
|
|
|
What are 4 ways in which an XY has a female phenotype
|
1) No MIF (no Mullerian Inhibitory Factor causing Persistent Mullerian Duct Syndrome)
2) Inadequate testosterone or dihydrotestosterone (eg 5-alpha-reductase deficiency - external female genitalia with cryptorchidism) 3) No androgen receptors (Androgen Insensitivity Syndrome - 46XY female, cryptorchidism, testes produce testosterone and MIF so no uterus) 4) No gonads: Swyer's Syndrome - 46XY perpubertal female (no oestrogen) due to gonadal agenesis |
|
|
A female child approaches puberty but shows no 2ndary sexual characteristics and amenorrhoea. What two classifications of 46XY abnormalities may have occurred
|
1) With uterus (ie MIF absent) then Swyer's (gonadal agenesis)
2) Without uterus (ie with MIF and testes) then androgen insensitivity syndrome |
|
|
Describe the pathogenesis of congenital adrenal hyperplasia
|
1) Deficiecy of 21-hydroxylase
2) Decreased synthesis of cortisol and aldosterone with hyponatremia, hyperkalemia, dehydration 3) Decreased cortisol causing Addisonian symptoms 4) Raised ACTH increasing production of precursor proteins resulting in increased progesterone and testosterone production - virilisation and genital ambiguity in females (lpenis-like clitoris) |
|

What is this, what virus
|
Condyloma accumenata, HPV (6, 11 are benign)
|
|
|
An excematous malignancy of the vulval epithelium
|
Extramammary Paget's Disease
|
|
|
Describe the symptoms of progression of PID
|
Begins wih vaginitis (pus in vagina), cervical inflammation (cervicitis), endometritis, salpingitis (and tuboovarian abcess causing fibrosis of Fallopian tube and ovary), oophoritis and peritonitis (guarding, rigidity, RT, adhesions, bowel obstruction)
|
|
|
Where do ectopics mainly occur
|
Ampulla (mid dilation) of the Fallopian tube
|
|
|
Why are HPV 16 and 18 oncogenic
|
Contain oncogenes for E6 (P53 knockout) and E7 (RBG)
|
|
|
What are the stages of development of cervical carcinoma
|
Dysplasia in epithelium:
1) CIN 1 - Basal region 2) CIN 2 - intermediate epihelium 3) CIN 3 - full thickness of epithelium 4) Carcinoma in situ (basement membrane intact) 5) Invasive SCC |
|
|
What are the complications of cervical carcinoma
|
Invasion of the rectum (constipation), haemorrhagic necrosis within the tumour causing post coital bleeding, invasion of the bladder, compression of the ureters with renal failure and/or sepsis
|
|
|
Age of precocious puberty
|
< 8 for secondary sexual characteristics or eaely menarch < 10
|
|
|
Define heterosexual
|
Secondary characteristics of opposite sex
|
|
|
What is measuring system for the stages of sexual development called and how is it different for boys and girls
|
Tanner stages:
Boys - orchidometer Girls - breasts and pubic hair |
|
|
What abnormalities are associated with precocious puberty
|
1) Increased ICP (eg hydrocephaly)
2) Functional sex cord stromal tumours (granulosa cell and thecomas in girls, sertoli and leydig cell tumours in boys |
|
|
What are two types of functional ovarian tumours and their consequences
|
1) Granulosa cell tumour, thecoma: secrete oestrogen and cause precocious puberty in girls and delayed puberty in boys
|
|
|
I quit the pill 8 months ago and I'm still not pregnant. Am I infertile
|
1) 12 months of unprotected sex without becoming pregnant is defined as infertility
2) Consider male infertility also |
|
|
What are fibroids originating from the myometrium. What are the complications and what if it's fast growing?
|
Leiomyoma (uterine fibroids) causing menorrhagia (anaemia), dysmenorrhoea, constipation, bladder and ureter compression (urgency, hydronephrosis, UTI) infertility
If fast growing: possible leiomyosarcoma |
|
|
Risk factors for PID
|
1) Previous PID
2) Younger age when sexually active 3) Low socioeconomic status 4) Multiple partners |
|
|
What are the signs and symptoms if PID
|
Asymptomatic early on
Lower abdominal pain Cervical, vaginal discharge Nausea and vomiting. Irregular bleeding and fever each occur in up to one third of patients. Cervical motion tenderness Guarding, and rebound tenderness Dyspareunia Dysuria |
|
|
Complications of PID
|
1) Tubo-ovarian abcess
2) Hydrosalpynx 3) Pyosalpynx 4) Fitz-Hugh-Curtis Syndrome (parahepatic fibrosis) |
|
|
What are the DDx of PID
|
1) Adnexal torsion
2) Ectopic pregnancy |