![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
149 Cards in this Set
- Front
- Back
|
The refractive status of the eye relates to: |
the manner in which light rays entering the eye are brought to a focus |
|
|
light rays |
light traveling through space in a straight lines |
|
|
optical infinity |
when light rays assume a virtually parallel course at a distance of about 20 ft (6 m) and is continuous to infinity |
|
|
When light rays encounter an object, what happens? |
they are either absorbed, reflected, or refracted |
|
|
The path a light ray takes as it passes through a transparent medium depends on two factors: |
angle of incidence and index of refraction (n) |
|
|
angle of incidence |
formed by the light ray and the surface of the medium |
|
|
index of refraction |
is a number that indicates the speed of light through a medium compared with the speed of light through a vacuum |
|
|
What is the formula for calculating the index of refraction? |
dividing speed of light in a vacuum, by the speed of light in the medium |
|
|
speed of light in a vacuum |
186,000 mps |
|
|
speed of light through water |
about 140,000 mps |
|
|
midline |
is that point at which light is traveling along the normal |
|
|
convex |
-"plus lens" |
|
|
concave |
-"minus lens" |
|
|
diopter |
How the power of a lens is measured, and is the reciprocal of the focal length of a lens (in meters) |
|
|
focal length |
is measured from the lens to the point at which the light rays meet on the midline |
|
|
The medium must be ________ to allow light through. |
transparent |
|
|
Refraction of light depends on what? |
1) the angle of incidence of the light rays |
|
|
cornea |
a clear, transparent, steeply curved structure that contributes about 70% of the optical power of the eye |
|
|
Light rays traveling from air into the cornea are refracted as a result of: |
anterior corneal curvature combined with the change in speed as the light rays pass from air into the cornea |
|
|
The total power of the cornea averages about: |
+42.00D |
|
|
How is the corneal curvature measured? |
by either a keratometer or an ophthalmometer |
|
|
Te average corneal curvature measures about: |
44.00D on the keratometer |
|
|
The cornea and aqueous humor _________ light rays entering the eye. |
converge |
|
|
crystalline lens |
a biconvex, normally transparent, resilient structure that lies just behind the iris |
|
|
How is the cyrstalline lens held in place? |
suspensory ligaments attached at one end to the ciliary muscle, and at the other end to the lens |
|
|
What are the 3 major layers of the lens? |
1) the highly elastic outer capsule |
|
|
What allows the lens to change shape? |
changes in tension on the suspensory ligaments |
|
|
accommodation |
the act of the crystalline lens changing its shape to focus |
|
|
The ability of the eye to accommodate depends on: |
age, refractive error, and overall physical health |
|
|
amplitude of accommodation |
the ability of the lens in the eye to focus |
|
|
measuring amplitude of accommodation : "push up" method |
a near point target (1-2 lines better than BCVA) is presented and brought toward the eyes until it blurs; distance between the target and the eyes is measured in cm and converted to diopters (divide the measurement into 100) |
|
|
Accommodation is generally greatest: |
in children, and decreases with age; Hofstetter's formula is able to calculate the average expected amplitude of accommodatoin |
|
|
Hofstetter's formula |
18.5 - (0.3 * age) |
|
|
accommodative reserve |
the difference between supply and demand |
|
|
accommodative insufficiency |
-insufficient amplitude of accommodation |
|
|
near point triad |
near point vision results in accommodation, convergence of the eyes, and miosis of the pupil |
|
|
retina to brain process |
the retina receives light rays, translates them into electrophysiologic impulses, and transmits the impulses to the brain where they are interpreted as a visual image |
|
|
photoreceptors |
-"light receivers" |
|
|
rods |
-the prevalent photoreceptor |
|
|
cones |
-about 7 million in the retina |
|
|
fovea centralis |
the area of the retina that provides the most acute vision; marked by a small depression in the center of the macula lutea |
|
|
axial length |
the length of the eyevall from the cornea to the posterior pole; average axial length = 23-25mm (about the size of a quarter) |
|
|
a-scan ultrasonography |
may be used to measure axial length; usually performed to calculate the power of an IOL before cataract surgery |
|
|
emmetropia |
a state of proper correlation between the refractive system of the eye and the axial length of the eyeball; rays of light entering the eye parallel to the optic axis being brought to a focus exactly on the retina |
|
|
ametropia |
*can be either refractive or axial* |
|
|
refractive ametropia |
axial length is normal and the refractive power (either/both the cornea and the lens) is either too strong or too weak to focus light rays on the retina |
|
|
axial ametropia |
refractive power of the eye is normal and the axial length is either too long or too short to place the retina at the point of focus |
|
|
myopia |
the refractive condition in which, when accommodation is relaxed, parallel light rays entering the eye focus in front of the retina (nearsighted) |
|
|
physiologic myopia |
myopia is usually physiologic - refers simply to the shape involving particularly either/both a steep corneal curvature and long axial length |
|
|
pathologic myopia |
causes include diabetes (change in blood sugar level affects index of refraction), and degenerative changes in the eyeball (cataract formation) |
|
|
orthokeratology |
-often called Corneal Refractive Therapy (CRT) |
|
|
hyperopia |
the refractive condition in which, when accommodation is relaxed, parallel light rays entering the eye focus behind the retina; farsighted/ hypermetropia (closely connected to accommodation) |
|
|
latent hyperope |
a hyperopic individual (usually child/adolescent), who accommodates constantly to compensate for refractive error |
|
|
Accommodation and convergence are related in that: |
with every diopter of accommodation, there is a specific amount of convergence (explained in the AC/A ratio) |
|
|
amblyopia |
-"lazy eye" |
|
|
astigmatism |
a refractive condition in which parallel light rays entering the eye do not focus at a single point but instead form two line images at different meridians, generally at right angles to each other |
|
|
interval of Sturm |
the distance between the 2 lines of focus in an astigmatism |
|
|
circle of least confusion |
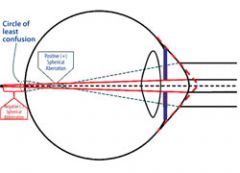
at the midpoint between the two focus lines (in an astigmatism) a circle is formed, the circle of least confusion |
|
|
residual astigmatism |
the difference between ocular astigmatism and corneal astigmatism |
|
|
regular astigmatism |
two the principal meridians are 90 degrees apart |
|
|
with-the-rule astigmatism |
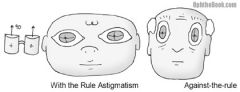
refers to a steeper curvature in the vertical meridian (like a football lying on its side) |
|
|
against-the-rule astigmatism |
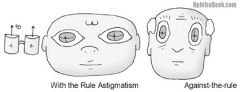
refers to a steeper curvature in the horizontal meridian (like a football standing on end) |
|
|
oblique astigmatism |
occurs when the meridians are between 30-60 degrees and 120-150 degrees |
|
|
irregular astigmatism |
-is not common in non-traumatized eyes |
|
|
Why is it impossible for an astigmatism to be axial? |
because an eyeball cannot be of two different lengths |
|
|
mixed astigmatism |
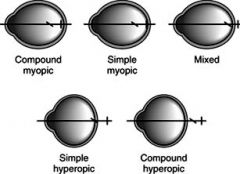
one focal line is in front of the retina, and the other is behind the retina |
|
|
simple astigmatism |
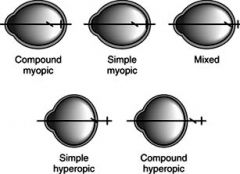
one line is on the retina, the other is either in front of the retina (simple myopic) or behind the retina (simple hyperopic) |
|
|
compound astigmatism |
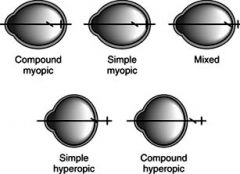
both focus lines are either in front of the retina (compound myopic) or behind the retina (compound hyperopic) |
|
|
cylindrical lens |
a lens with power in only one meridian |
|
|
spherocylinder |
used for compound or mixed asitgmatism; has a different power in each of its principal meridians |
|
|
RGP |
has a rigid spherical back surface that rests on the corneal tear film; the tear film fills in the spaces |
|
|
bitoric contact lenses |
have toric curves on both the front and back surfaces; used in cases of combined significant residual astigmatism and corneal astigmatism |
|
|
radial keratotomy |
performed by making spoke-like incisions into the cornea to flatten the center |
|
|
photorefractive karatectomy (PRK) |
uses a custom-designed laser to reshape the cornea by scraping away the top layer of the cornea (epithelium) and vaporizing a portion of the middle layer (stroma) |
|
|
LASIK |
-Laser Assisted In Situ Kertomileusis |
|
|
presbyopia |
-is a reduction in the ability to accommodate that occurs normally with age |
|
|
aphakia |
the absence of the crystalline lens |
|
|
cataracts |
-an opacity of the cyrstalline lens or its capsule |
|
|
senile cataract |
*most prevalent type of cataract* |
|
|
nuclear cataract |
-may cause an increase in myopia or a decrease in hyperopia |
|
|
subcapsular cataracts |
-often appear at the posterior pole of the lens |
|
|
cortical cataracts |
-are cataracts within the cortex itself |
|
|
treatment for aphakia |
involves one of or a combo of three methods: |
|
|
spectacle lens correctin for aphakia |
-"aphakic spectacle lenses" |
|
|
full-field aphakic spectacle lenses |
has power throughout the lens that decreases from center to edge |
|
|
lenticular aphakic spectacle lenses |

-reduces thickness and weight |
|
|
contact lens correction for aphakia |
afford the patient a comfortable, nonmagnified, wide-field vision |
|
|
IOL implant to correct for aphakia |
-most commonly used method to treat aphakia |
|
|
anisometropia |
a condition of unequal refractive state of the two eyes, usually at least 1 diopter different |
|
|
What are the 3 types of anisometropia? |
simple |
|
|
simple anisometropia |
one eye is emmetropic the other is ametropic |
|
|
compound anisometropia |
refers to both eyes being myopic, hyperopic, or astigmatic, but in differing amounts |
|
|
mixed anisometropia (antimetropia) |
one eye is myopic, the other is hyperopic |
|
|
refractive anisometropia |
attributed to a marked difference in corneal curvature of the two eyes, or monocular aphakia; best corrected with contact lenses |
|
|
axial anisometropia |
attributed to difference in axial length between the two eyes along with fairly equal curvature (resulting in a marked difference in total refractive error); best corrected with glasses |
|
|
aniseikonia |
a difference in size of the two retinal images; two major subdivisions are inherent and acquired |
|
|
inherent aniseikonia |
refers to different image sizes caused by the refractive condition of the two eyes |
|
|
acquired aniseikonia |
occurs as a result of the effects of corrective lenses |
|
|
eikonometer |
clinical measurement of aniseikonia (eikonometry is performed with the eyes disassociated, either with polarized filters, or independently adjustable optical systems for each eye) |
|
|
iseikonic lenses |
lenses specifically designed to alleviate aniseikonia |
|
|
amblyopia |
-"lazy eye" |
|
|
strabismic amblyopia |
-is also called amblyopia ex anopsia |
|
|
refractive amblyopia |
-associated with uncorrected refractive errors |
|
|
stimulus deprivation amblyopia |
-results when sensory receptors do not receive input (i.e. retina doesn't receive light), due to some factor, such as a congenital cataract |
|
|
The eye is said to have a refractive error when ______________. |
light rays don't bend properly to form a single-point focus on the retina |
|
|
The index of refraction is abbreviated by the symbol _____________. |
n |
|
|
A light ray traveling from one medium to another medium that has a higher index of refraction will be _____________. |
bent toward the normal |
|
|
Divergence occurs when light rays ________________. |
bend away from the midline |
|
|
There is no refraction of light at __________________. |
the optical center |
|
|
Light rays assume a virtually parallel course, "optical infinity", at approximately _____________. |
20 ft/6m |
|
|
Convex lenses are also referred to as ________________. |
plus lenses |
|
|
A lens in which the center is thinner than its edges is known as _________________. |
concave |
|
|
Light rays entering the eye must first pass through the ________________. |
cornea |
|
|
Which structure contributes approximately 70% of the optical power of the eye? |
the cornea |
|
|
Combining front and back surface powers, the total power of the cornea averages approximately how many diopters? |
42.00D |
|
|
Which part of the eye is biconvex, normally transparent, and fits just behind the iris? |
the crystalline lens |
|
|
Accommodation is defined as ________________. |
the act of the crystalline lens at varying distances |
|
|
The number of diopters of power is equal to the reciprocal of the focal length of a lens in ______________. |
meters |
|
|
A 3.00D lens has a focal length of ________________. |
33 cm |
|
|
The ability of the crystalline lens to focus is known as |
amplitude of accommodation |
|
|
Accommodative reserve is the difference between _________________. |
supply and demand |
|
|
There are approximately 130 million of what in the human retina? |
rods |
|
|
Cones in the human retina provide which of the following? |
c |
|
|
The area of the retina that provides the most acute vision is the _________________. |
fovea centralis |
|
|
What is the length of the eyeball from the cornea to the posterior pole known as? |
axial length |
|
|
Axial length discrepancies will results in producing a __________________. |
refractive error |
|
|
In an emmetropic eye, where are parallel light rays refracted? |
on the retina |
|
|
Myopia is commonly called ______________. |
nearsighted |
|
|
Concave lenses would be used to correct ________________. |
myopia |
|
|
Minus lenses may cause ____________________. |
barrel distortion |
|
|
How are light rays refracted in hyperopia? |
behind the retina |
|
|
Hyperopia is closely connected with what? |
accommodation |
|
|
Treatment for hyperopia is usually with what type of lens? |
convex lenses |
|
|
What is the distance between two line of focus called? |
Interval of Sturm |
|
|
The difference between total ocular astigmatism and corneal astigmatism is called __________________. |
residual astigmatism |
|
|
In mixed astigmatism, the focal lines are __________________. |
one in front of the retina, one behind the retina |
|
|
What type of lens is used for correction of compound astigmatism? |
spherocylindrical |
|
|
A normal reduction in the ability to accommodate is known as ______________. |
presbyopia |
|
|
What is the distinction between hyperopia and presbyopia? |
accommodative amplitude |
|
|
Who is credited with inventing bifocals? |
Benjamin Franklin |
|
|
What is the most prevalent type of cataract? |
senile |
|
|
What is aphakia? |
the absence of the crystalline lens |
|
|
What is the condition of an unequal refractive state of the two eyes known as? |
anisometropia |
|
|
How is refractive anisometropia best corrected? |
contact lenses |
|
|
What instrument is used in the clinical measurement of aniseikonia? |
eikonometer |
|
|
The difference in the size of the two retinal images is known as ___________________. |
aniseikonia |
|
|
What is the small depression in the center of the macula lutea, which is located at the back of the retina? |
fovea centralis |
|
|
What are the major categories of amblyopia? |
-strabismic amblyopia |
|
|
Strabismic amblyopia ("lazy eye") is most likely the result of what? |
abnormal binocularity |