Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
24 Cards in this Set
- Front
- Back
|
case
|

|
|
|
RF/ ETIOLOGY
|

|
|
|
PRESENTATION
|

|
|
|
DS
|

|
|
|
TX/ COMPLICATIONS
|

|
|
|
signs and symptoms of infective endocarditis include
|
signs and symptoms of infective endocarditis include acute findings of fever, anorexia, weight loss, pallor, night sweats, myalgias, and new onset of a heart murmur, usually as a
result of valve disease from infection. Later findings result from embolic phenomena and include splinter hemorrhages, Roth spots (retinal hemorrhages), Janeway lesions, Osler nodes, splenomegaly, clubbing, arthralgias, arthritis, glomerulonephritis, and aseptic meningitis |
|
|
The pathogenesis of infective endocarditis results from
|
The pathogenesis of infective endocarditis results from the initial setting of a jet of blood or turbulence within the heart leading to endothelial
damage and formation of a sterile clot or vegetation. |
|
|
DS
|
|
|
|
DS
|
|
|
|
most common causative organisms.Among patients with bums or IV drug abusers
|
Among patients with bums or IV drug abusers, staphylococci
are the most common causative organisms. Infants with sepsis are also at higher risk for endocarditis with no underlying cardiac disease |
|
|
considered to be highrisk
lesions for development of infective endocarditis |
Valvular heart lesions are most commonly associated
with predisposition for the development of infective endocarditis; however, other forms of congenital heart disease, including tetralogy of Fallot, ventricular septal defect, patent ductus arteriosus, coarctation of the aorta, and pulmonary valve stenosis, have also been implicated. Congenital heart defects such as atrial septal defect, peripheral pulmonary stenosis, and mitral valve prolapse without mitral regurgitation are not considered to be highrisk lesions for development of infective endocarditis, and thus bacterial endocarditis prophylaxis is not indicated in these situations |
|
|
In patients with suspected infective endocarditis, a course of
|
In patients with suspected infective endocarditis, a course of either vancomycin or oxacillin and gentamicin
is started because the most likely organisms include streptococci and staphylococci, depending on the rate of methicillin-resistant S aureus in the patient's geographic area. Once the organism is identified, the antibiotic regimen can be adjusted. |
|
|
complications associated with endocarditis include
|
complications associated with endocarditis include mycotic aneurysms, localized cardiac abscesses, and autoimmune
phenomena such as nephritis and arthritis. |
|
|
Procedures in which there is a risk for significant
bacteremia would require bacterial endocarditis prophylaxis. |
Procedures in which there is a risk for significant
bacteremia would require bacterial endocarditis prophylaxis. These procedures include dental procedures where bleeding is anticipated, tonsillectomy, cardiac surgery, incision of infected sites, urologic surgery, and Foley placement in the presence of a urinary tract infection. Endotracheal intubation is not associated with a high incidence of bacteremia and thus antibiotic prophylaxis is not required. |
|
|
Common organisms causing infective endocarditis in relation to native valve or other cardiac lesions and prosthetic valve:
|
Common organisms causing infective endocarditis in relation to native valve or other cardiac lesions and prosthetic valve: 0) Prosthetic valve: Staphylococcus epidermidis, Staphylococcus aureus, Streptococcus, viridans, Pseudomonas
aeruginosa, Serratia marcescens, and fungi. (li) Native valve or other cardiac lesions: Streptococcus viridans group, Staphylococcus aureus, and group D. streptococcus |
|
|
CASE
KEY WORDS |

|
|
|
Which antibiotic should not be used in a patient with infective endocarditis and is allergic to penicillin?
|

|
|
|
Antibiotics used in infective endocarditis
|

|
|
|
Antibiotics used in infective endocarditis
|

|
|
|
Antibiotic prophylaxis is not recommended (important for Board examination
|

|
|
|
Antibiotic prophylaxis is recommended (important for Board examination
|

|
|
|
Endocarditis prophylaxis is recommended
|
|
|
|
Endocarditis prophylaxis is not recommended:
|

|
|
|
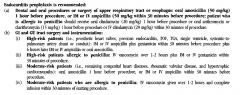
Endocarditis prophylaxis is indicated (high-risk and moderate-risk patients):
|

|