Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
36 Cards in this Set
- Front
- Back

|
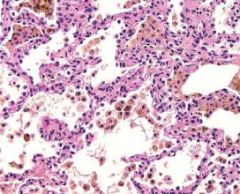
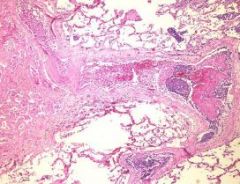
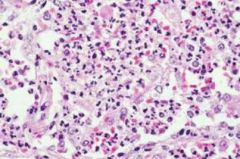
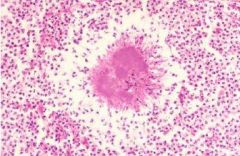
Normal Alveolar Parenchyma
- shows a pulmonary macrophage in a central alveolus |
|
|
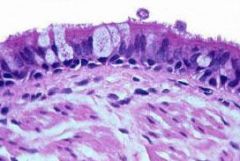
Normal Bronchus
- bronchial wall includes respiratory mucosa, smooth muscle, submucosa with seromucinous glands, and cartilage. The epithelium is pseudostratified and columnar and cosists of ciliated cells, goblet cells, and reserve cells. Neuroendocrine cells cannot be distinguished. |
|
|
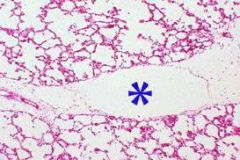
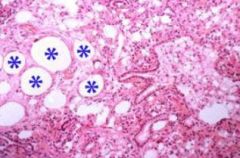
Normal Intralobular Septum with Lymphatic
- lymphatic (*) couses through an intralobular septum |
|
|
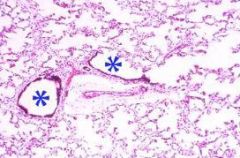
Normal Alveolar Parenchyma
- Terminal and respiratory bronchioles shown with alveolar ducts, sacs, and a small artery. |
|
|
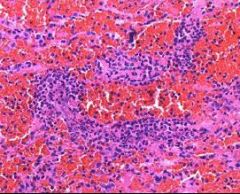
Chronic Passive Congestion
- Hemosiderin laden macrophages ("heart failure cells") and edematous fluid occupies the alveoli |
|

|
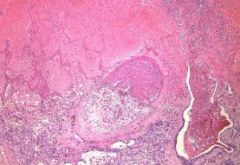
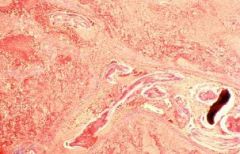
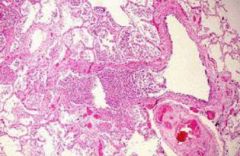
Recent Pulmonary Infarct
- lies in the typical subpleural location and has the characteristic "wedge" shape. The hemorrhagic appearance tells you that it is a recent not old infarct. |
|
|
Organizing PE
- A small artery is filled by an organizing fibrin embolus |
|
|
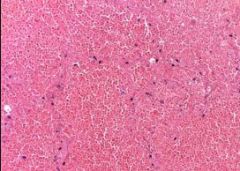
Pulmonary Infarct
- The lung tissue shows coagulative necrosis and hemorrhage |
|
|
Tumor Emboli
- A plug of metastatic carcinoma and fibrin fills a small pulmonary artery. The parenchyma on the left is infarcted. |
|
|
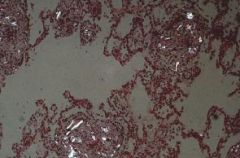
IV Talcosis
- Abundant talc, which is polarizable, is present adjacent to blood vessels in this lung of an IV drug user |
|
|
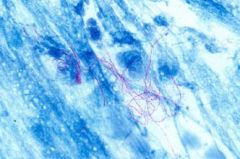
Dirofilaria Immitis
- The body of a dog heartworm is curled in the lumen of a small pulmonary artery. Seen with Masson trichrome stain. |
|
|
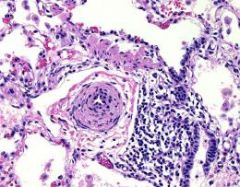
Pulmonary HTN
- This small artery demonstrates medial hypertrophy |
|
|
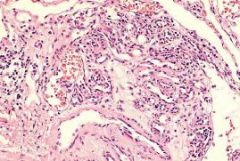
Pulmonary HTN
- This plexiform lesion is an aggregate of small capillaries and indicates the existense of SEVERE pulmonary HTN |
|
|
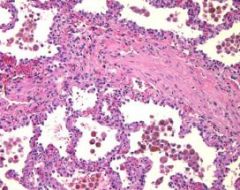
Pulmonary Veno-Occlusive Disease
- A small vein is occluded by fibrous tissue and the surrounding lung shows changes of chronic passive congestion (hemisiderin layden macrophages) |
|
|
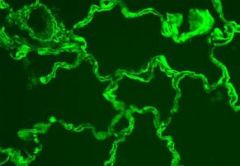
Goodpasture's Syndrome
- IF staining for IgG reveals the linear diagnostic staining along the alveolar basement membrane |
|
|
Wegener's Granulomatosis - small vessel vasculitis
- The capillaries are densely infiltrated by PMNs and there is a background of pulmonary hemorrhage |
|
|
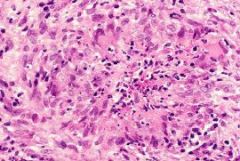
Wegener's Granulomatosis - granuloma
- This small granuloma has a central microabscess |
|

|
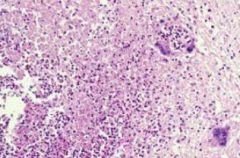
Acute Bronchopneumonia
- The tan-yellow spots centered around the airways are foci of acute bronchopneumonia, represents acute inflammatory exudate in bronchi, bronchioles and adjascent alveoli |
|
|
Acute Bronchopneumonia
- PMNs fill a bronchiole and adjascent alveoli |
|
|
Acute Bronchopneumonia
- PMNs fill a bronchiole and adjascent alveoli |
|
|
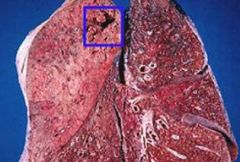
Lobar Pneumonia
- Left upper lobe is pale, firm and consolidated reflecting the acute inflammatory exudate filling all airspaces. The box contains focal abscess formation. |
|

|
Empyema
- Suppurative exudate covers the pleural surfaces. This can organize to form a pleural rind and pleural adhesion that can impair lung expansion |
|
|
Lipoid Pneumonia
- Large empty spaces represent collections of fat (washed out)(. The fat triggers fibrosis. Endogenous lipoid pneumonia is usually caused by bronchial obstruction by a tumor or other process and is histologically similar but lacks the large fat collections |
|
|
Nocardia asteroides
- form chains and are acid fast positive |
|
|
Actinomyces israelii
- This is the characteristic sulfur granule formed by the bacteria |
|
|
|
Lung Abscess
- cavity formed by suppurative necrosis of lung tissue, in this case caused by a bacterial infection that was probably related to aspiration because its located in the RLL |
|

|
Lung Abscess
- cavity formed by suppurative necrosis of lung tissue, in this case caused by a bacterial infection that was probably related to aspiration because its located in the RLL |
|
|
|
|
|
|
Lung Abscess
- PMNs are mixed with necrotic material. The giant cells raise the possibility of aspirated material (although we can't see any aspirated material here) |
|
|
|
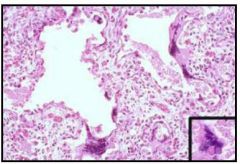
Respiratory Syncytial Virus
- Alveolar septa are widened and show prominent fibroblast proliferation. Multinucleated giant cells characteristic of RSV are present. The inset shows a giant cell with an eosinophilic intracytoplasmic inclusion. |
|
|
|
Respiratory Syncytial Virus
- Alveolar septa are widened and show prominent fibroblast proliferation. Multinucleated giant cells characteristic of RSV are present. The inset shows a giant cell with an eosinophilic intracytoplasmic inclusion. |
|
|
Respiratory Syncytial Virus
- Alveolar septa are widened and show prominent fibroblast proliferation. Multinucleated giant cells characteristic of RSV are present. The inset shows a giant cell with an eosinophilic intracytoplasmic inclusion. |
|
|
|
Influenza A induced necrotizing tracheobronchitis and diffuse alveolar damage
- The lungs are red and firm. The tracheal and bronchial mucosa is marked hyperemic due to necrosis of the bronchial epithelium. |
|
|
|
Influenza A induced necrotizing tracheobronchitis and diffuse alveolar damage
- The lungs are red and firm. The tracheal and bronchial mucosa is marked hyperemic due to necrosis of the bronchial epithelium. |
|

|
Influenza A induced necrotizing tracheobronchitis and diffuse alveolar damage
- The lungs are red and firm. The tracheal and bronchial mucosa is marked hyperemic due to necrosis of the bronchial epithelium. |
|
|
|
Adenovirus induced necrotizing bronchiolitis and pneumonia
- A bronchiole and surrounding alveoli are filled with acute inflammatory exudate and necrosis |