Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
223 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What is gait? ***
|
translatory progression of the body produced by coordinated, rotatory movements of body joints
|
|
|
|
The body moves in a straight line via _______. ***
|
angular joint motions
|
|
|
|
What capability is required for (general plane) motion of the human body? ***
|
- persons muscle must be able to accept and support weight of HAT (75% BW) on one lower extremity and at same time swing other LE forward in order to progress
|
|
|
|
What is a gait cycle? ***
|
- activities occurring from the point of initial heel contact of one LE to the point at which initial heel contact of the same extremity occurs again
- heel strike to heel strike of same LE |
|
|
|
During one gait cycle, each extremity passes through what two phases? ***
|
- stance phase
- swing phase |
|
|
|
Describe the stance phase. ***
|
- extremity is in contact with ground
- 60% of gait cycle is stance phase - heel strike: instant the heel contacts surface - foot flat: immediately after heel strike; foot is flat on surface - midstance: body weight passes over supporting LE - heel off: point at which heel leaves the ground - toe off: only the toe is in contact with the ground (Heel off + toe off may be collectively called push off) |
|
|
|
How much of the gait cycle consists of stance phase? ***
|
60%
|
|
|
|
Heel off + toe off may collectively be called _____ ____. ***
|
push off
|
|
|
|
What are the 5 parts of the stance phase (traditional)? ***
|
- heel strike
- foot flat - midstance - heel off - toe off |
|
|
|
Describe the swing phase (traditional). ***
|
- 40% of gait cycle
- acceleration: begins once the toe leaves ground and continues until midswing - midswing: leg passes directly beneath body - deceleration: occurs after midswing when knee is extending for heel strike |
|
|
|
How much of the gait cycle consists of swing phase? ***
|
40%
|
|
|
|
What are the 3 parts of the swing phase (traditional)? ***
|
- acceleration
- midswing - deceleration |
|
|
|
Describe double support ***
|
-gait cycle consists primarily of single support activity except for two periods of double support
- occurs when both limbs are in contact with the ground at the same time - early stance phase and late stance phase |
|
|
|
How much double support occurs during running? ***
|
- none
- there are periods of time when neither extremity is in contact with the ground |
|
|
|
What is stance time? ***
|
- amount of time during stance phase of one extremity during gait cycle
- will decrease if pain or weakness in stance leg |
|
|
|
What is stride length? ***
|
- distance between two successive heel strikes of same LE
- left step length + right step length = stride length |
|
|
|
How may stride length vary? ***
|
- varies with leg length, height, age, sex
- decreases with elderly, increases with increased speed |
|
|
|
What is step length? ***
|
- distance from heel strike of one LE to heel strike of opposite extremity
- a measure of gait symmetry - if R and L step lengths are unequal gait is asymmetrical - step length R + step length L should = stride length (average adult is 28 inches + 28 inches = 56 inches) |
|
|
|
What is cadence? ***
|
- number of steps per minute (count each heel strike)
- as step length decreases, cadence increases at any given velocity - usually 80-120 spm normal walking |
|
|
|
What is normal cadence? ***
|
- usually 80-120 spm normal walking
- average men = 110 spm, women = 116 spm |
|
|
|
What is cadence for running? ***
|
180 spm
|
|
|
|
What happens as you approach a cadence of 180 spm? As you pass 180 spm? ***
|
- double stance time decreases
- at over 180 spm running occurs because to achieve that cadence double stance disappears and float periods appear |
|
|
|
What is step width? ***
|
- width of base of support
- distance between midpoint of heel of one foot and same point on the other foot - increased when there is an increased demand for side-to-side stability - normal range (1-5 inches; average 3 inches) |
|
|
|
What is a normal range for step width? ***
|
- normal range (1-5 inches)
|
|
|
|
How much ROM is needed in LE for normal gait? ***
|
- approximate total ROM for normal gait is determined by looking at joint angle at each LE joint though gait cycle
- if individual has limited ROM at any of the joints, gait pattern will exhibit deviations from normal |
|
|
|
How much ROM is needed for normal gait at the hip? ***
|
- 30 degrees flexion
- 10-20 degrees extension |
|
|
|
How much ROM is needed for normal gait at the knee? ***
|
- 60 degrees flexion
- full extension |
|
|
|
How much ROM is needed for normal gait at the ankle? ***
|
- 10 degrees dorsiflexion
- 20 degrees plantar flexion |
|
|
|
What are determinants of gait? ***
|
- adjustments made by the body to help keep movements of body’s COG to a minimum
- minimize vertical displacement and horizontal displacement - transverse pelvic rotation - pelvic tilt - knee flexion during midstance - foot and ankle motion - knee motion - lateral pelvic rotation |
|
|
|
What is normal vertical displacement? ***
|
- about 2 inches
- highest at midstance - lowest at heel strike |
|
|
|
Where in the gait cycle is horizontal displacement greatest? ***
|
midstance
|
|
|
|
How is gait made more/less efficient? ***
|
- if changes in body’s COG are large and abrupt, more energy expended
- as changes are minimized gait becomes more efficient and less energy is required |
|
|
|
By what body mechanics is vertical displacement minimized? ***
|
- lateral pelvic tilt
- knee flexion at midstance - proper knee/ankle/foot interactions - pelvic rotation |
|
|
|
How does proper lateral pelvic tilt minimize vertical displacement? ***
|
- slight pelvic drop on nonstance side keeps COG lower than if pelvis did not drop
- action of gluteus medius prevents excessive drop |
|
|
|
How does proper knee flexion at midstance minimize vertical displacement? ***
|
- COG is highest at midstance
- with knee in slight flexion, COG is kept from rising |
|
|
|
How do proper knee/ankle/foot interactions minimize vertical displacement? ***
|
movements at knee occur in conjunction with movements at ankle/foot to prevent abrupt changes in vertical displacement of body's COG by lengthening or shortening extremity
|
|
|
|
How does proper pelvic rotation minimize vertical displacement? ***
|
- creates an apparent lengthening of LE, preventing an excessive drop in COG
- (see text pg. 347) |
|
|
|
How is horizontal displacement reduced? ***
|
physiologic valgus at knee
- reduces width of BOS from what it would be if femoral and tibial shafts formed a vertical line from greater tuberosity - BOS is relatively narrow - therefore little horizontal displacement is necessary to shift COG from one LE to the other |
|
|
|
What are the 5 parts of the stance phase (Rancho Los Amigos- RLA)? ***
|
- initial contact
- loading response - midstance - terminal stance - preswing |
|
|
|
What are the 3 parts of the swing phase (Rancho Los Amigos- RLA)? ***
|
- initial swing
- midswing - terminal swing |
|
|
|
Describe muscle activation and function during gait. ***
|
- muscles generate force and control for trunk and limb movement during gait
- control acceleration and deceleration for smooth movement - most muscle activation is eccentric to control contact with walking surface - muscles work synergistically, but some muscle groups are the most active during specific sub-phases of gait |
|
|
|
What muscles are active during the toe off/preswing phase of gait? ***
|
- adductors (pectineus, gracilis, adductor longus/brevis/magnus)
|
|
|
|
What muscles are active during the acceleration/initial swing phase of gait? ***
|
- pretibial/dorsiflexors (tibialis anterior, extensor hallucis longus, extensor digitorum longus)
|
|
|
|
What muscles are active during the midswing phase of gait? ***
|
- hamstrings (biceps femoris, semitendinosus, semimembranosus)
- pretibial/dorsiflexors (tibialis anterior, extensor hallucis longus, extensor digitorum longus) |
|
|
|
What muscles are active during the deceleration/terminal swing phase of gait? ***
|
- gluteus maximus
- gluteus medius - quadriceps femoris - hamstrings (biceps femoris, semitendinosus, semimembranosus) - pretibial/dorsiflexors (tibialis anterior, extensor hallucis longus, extensor digitorum longus) |
|
|
|
What muscles are active during the heel strike/initial contact phase of gait? ***
|
- gluteus maximus
- gluteus medius - adductors (pectineus, gracilis, adductor longus/brevis/magnus) - hamstrings (biceps femoris, semitendinosus, semimembranosus) - pretibial/dorsiflexors (tibialis anterior, extensor hallucis longus, extensor digitorum longus) |
|
|
|
What muscles are active during the foot flat/loading response phase of gait? ***
|
- gluteus maximus
- gluteus medius - hamstrings (biceps femoris, semitendinosus, semimembranosus) - plantar flexors (gastrocnemius, soleus, tibialis posterior, flexor digitorum longus, flexor hallucis longus, peroneus longus, peroneus brevis) |
|
|
|
What muscles are active during the midstance phase of gait? ***
|
- gluteus maximus
- gluteus medius - plantar flexors (gastrocnemius, soleus, tibialis posterior, flexor digitorum longus, flexor hallucis longus, peroneus longus, peroneus brevis) |
|
|
|
What muscles are active during the heel off/terminal stance phase of gait? ***
|
- plantar flexors (gastrocnemius, soleus, tibialis posterior, flexor digitorum longus, flexor hallucis longus, peroneus longus, peroneus brevis)
|
|
|
|
Describe heel strike (initial contact--RLA) in the stance phase (COG, ankle, knee, hip actions). ***
|
- gait cycle beginning, when heel first contacts ground
- COG of body is at its lowest point - ankle is held in neutral dorsiflexion - ankle transitions toward foot-flat stance and dorsiflexor muscles are eccentrically activated to lower ankle into plantar flexion - knee is slightly flexed, positioned to absorb shock of initial weight bearing - quadriceps are eccentrically active to allow a slight “give” to flexed knee and help prevent knee from buckling - hip extensors are isometrically active to prevent trunk from jackknifing forward |
|
|
|
Describe foot flat (loading response--RLA) in the stance phase (muscular, ankle, knee, hip actions). ***
|
- point in which entire plantar surface of foot contacts ground
- loading-response phase of gait - muscles and joints of lower limb assist with shock absorption, as lower extremity continues to accept increasing amounts of body weight - ankle has just rapidly moved into 5-10 degrees of plantar flexion - knee continues to flex to about 15 degrees, acting as a shock absorbing “spring” - quadriceps continue to function eccentrically, and hip extensors guide hip toward increasing extension |
|
|
|
Describe midstance (midstance--RLA) in the stance phase (muscular, ankle, knee, hip actions). ***
|
- occurs as leg approaches vertical position
- leg is in single-limb support, as other limb is freely swinging forward - dorsiflexor muscles are inactive; plantar flexor muscles are eccentrically active, controlling rate at which lower leg advances over foot - knee reaches near-fully extended position - hip abductors play important role in stabilizing pelvis in frontal plane, preventing opposite side of pelvis from dropping excessively |
|
|
|
Describe heel off (terminal stance--RLA) in the stance phase (muscular, ankle, knee, hip actions). ***
|
- occurs just after mid stance as lower leg and ankle begin “pushing off,” continuing to propel body forward
- begins as heel breaks contact with ground - plantar flexor muscles and Achilles tendon stretch in preparation for propulsion - at heel off, plantar flexor muscles have switched their activation from eccentric to concentric - extended knee prepares to flex, usually driven by short burst of activity from hamstring muscles - hip continues to extend, ending in about 10 degrees of extension - eccentric activation of hip flexors, particularly iliopsoas, helps control amount of hip extension that occurs |
|
|
|
Describe toe off (preswing--RLA) in the stance phase (muscular, ankle, knee, hip actions). ***
|
- final event of stance phase of gait
- toe off ends when toes break contact with ground - toes are in marked hyperextension at metatarsophalangeal joints, supported by activation of intrinsic foot muscles - ankle continues plantar flexing through concentric activation of plantar flexor muscles - at toe off, knee is flexed 30 degrees, but hamstrings are only minimally active - most knee flexion arises as a result of inertia produced, as hip is pulled into flexion - in final stage of toe off, hip is in nearly-neutral position, with thigh nearly perpendicular to ground |
|
|
|
Describe acceleration (initial swing--RLA) in the swing phase (muscular, ankle, knee, hip actions). ***
|
- leg begins to accelerate forward
- plantar flexed ankle begins to dorsiflex, clearing ground as it is advanced forward - knee continues to flex, and hip flexors continue to contract, pulling extended thigh forward |
|
|
|
Describe midswing (midswing--RLA) in the swing phase (muscular, ankle, knee, hip actions). ***
|
- midpoint of swing phase
- contralateral leg is mid stance, supporting body weight - ankle is held in neutral position - knee is flexed about 50-60 degrees, helping advance lower limb - hip approaches 35 degrees of flexion, continuing to be pulled forward through concentric hip flexor activation |
|
|
|
Describe deceleration (terminal swing--RLA) in the swing phase (muscular, ankle, knee, hip actions). ***
|
- limb begins to decelerate in preparation for heel contact
- leg is placed well in front of body, preparing for transition to accept body weight - ankle dorsiflexors are activated isometrically, positioning foot for heel contact - knee has moved from flexed position of mid swing to almost full extension - hamstrings are active eccentrically at this time to slow rapidly extending knee - hip flexor muscles become inactive in terminal swing - hip extensors decelerate forward leg progression leg through eccentric activation |
|
|
|
Describe muscle and joint interactions at the hip in the frontal plane during gait cycle. ***
|
- abductor muscles play important role in frontal plane hip stability
- without activation of hip abductors on stance leg, opposite side of pelvis would drop under force of gravity, known as positive Trendelenburg sign - activation of stance leg’s hip abductors holds pelvis level |
|
|
|
Describe muscle and joint interactions at the knee in the frontal plane during gait cycle. ***
|
- strong medial and lateral collateral ligaments of knee provide natural stability to knee in frontal plane
- loss of this stability may lead to issues such as genu valgus, potentially altering normal gait mechanics - instability of knee may arise from impairments at hip or foot |
|
|
|
Describe muscle and joint interactions at the ankle in the frontal plane during gait cycle. ***
|
- while walking, subtalar and transverse tarsal joints cooperate to transform foot from pliable platform at early stance to more rigid platform at late stance
- position of supination arranges bones of foot to their most stable position, forming rigid lever for push-off |
|
|
|
Describe muscle and joint interactions in horizontal plane during gait cycle. ***
|
- much of lower limb control within horizontal plane during walking occurs at hip and foot
- during walking, pelvis rotates in horizontal plane about a vertical axis of rotation through hip joint of stance leg - because trunk remains relatively stationary during walking, lumbar spine must rotate slightly to de-couple rotating pelvis from thorax |
|
|
|
What are some causes of atypical/abnormal gait? ***
|
- muscular weakness/paralysis
- joint muscle ROM limited - neurological involvement - pain - leg length discrepancy |
|
|
|
Name some types of atypical/abnormal gait. ***
|
- antalgic gait
- ataxic gait - circumducted gait - crouch gait - equinnus gait - gluteus maximus gait - gluteus medius gait - hemiplegic gait - Parkinsonian gait (festinating) - scissors gait - steppage gait - vaulting gait - waddling gait |
|
|
|
Foot slap is a gait deviation most likely due to which of the following impairments? ***
a. contracture or tightness of the hamstrings b. weakness of the quadriceps c. weakness of the dorsiflexor muscles d. weakness of the hip abductor muscle |
c. weakness of the dorsiflexor muscles
|
|
|
|
Which of the following is not true regarding the heel contact component of a gait cycle? ***
a. heel contact occurs at the beginning (0%) period of the gait cycle b. at heel contact, the ankle is typically held in about 20 degrees of plantar flexion c. at heel contact, the knee is slightly flexed to help absorb the impact of initial weight bearing d. at heel contact, the hip extensor muscles are active to prevent the trunk from jackknifing forward |
b. at heel contact, the ankle is typically held in about 20 degrees of plantar flexion
|
|
|
|
Which of the following are considered components of the stance phase of a gait cycle? ***
a. heel off b. mid swing c. foot flat d. a and c e. all of the above |
d. a and c
|
|
|
|
At which of the following periods within a gait cycle is the leg in single-limb support? ***
a. heel contact b. foot flat c. mid stance d. a and b e. all of the above |
c. mid stance
|
|
|
|
Which of the following events follows the mid-stance period of a gait cycle? ***
a. foot flat b. heel off c. toe off d. early swing |
b. heel off
|
|
|
|
Which of the following best describes the events that occur during terminal swing? ***
a. strong concentric contraction of the plantar flexors to reach the foot forward b. hip and knee both in a fully extended position c. eccentric activation of the hamstrings to decelerate the extending knee d. concentric activation of all the hip extensor muscles |
c. eccentric activation of the hamstrings to decelerate the extending knee
|
|
|
|
Which of the following best describes a weak quadriceps gait deviation? ***
a. a fully extended knee throughout stance combined with a forward lean of the trunk to keep the line of gravity anterior to the medial-lateral axis of the knee b. rising up on tip-toes during the stance phase of gait to clear the swing leg from the ground c. hyperextension of the hip during the swing phase of gait d. excessive flexion of the knees and hips during the stance phase of gait |
a. a fully extended knee throughout stance combined with a forward lean of the trunk to keep the line of gravity anterior to the medial-lateral axis of the knee
|
|
|
|
Which of the following is considered an average walking velocity for a healthy adult? ***
a. 3 mph b. 5 mph c. 6 mph d. 1 mph |
a. 3 mph
|
|
|
|
Which of the following gait deviations or compensations is most likely used by a person walking with a brace that keeps the knee in extension? ***
a. uncompensated weak hip abductor gait b. high-stepping gait c. hip circumduction d. a and b e. all of the above |
c. hip circumduction
|
|
|
|
The body's center of gravity is at its highest point during which of the following periods of a gait cycle? ***
a. heel contact b. early swing c. mid stance d. foot flat |
c. mid stance
|
|
|
|
Which of the following best describes a vaulting gait deviation? ***
a. excessive hyperextension of the knee during the stance phase of gait b. flexion of the hip and knee during the stance phase of gait c. rising up on the toes of the stance leg to create extra clearance for the swing leg d. pelvis drops excessively on the side opposite the stance limb |
c. rising up on the toes of the stance leg to create extra clearance for the swing leg
|
|
|
|
Concentric contraction of the hip flexor muscles is most likely to occur during: ***
a. mid stance b. early swing c. foot flat d. terminal swing |
b. early swing
|
|
|
|
The hamstrings are activated eccentrically during terminal swing in order to slow the advancing leg. ***
a. true b. false |
a. true
|
|
|
|
The periods of double-limb support are considered the least stable portions of a gait cycle. ***
a. true b. false |
b. false
|
|
|
|
The subtalar and transverse tarsal joints cooperate to transform the foot into a pliable platform during early stance. This is an essential component of the shock-absorbing mechanism during the transition to full weight bearing. ***
a. true b. false |
a. true
|
|
|
|
An individual with a hip flexion contracture of the right leg is likely to display genu recurvatum of the same (right) leg. ***
a. true b. false |
b. false
|
|
|
|
The dorsiflexor muscles are isometrically activated during mid swing to prevent the foot from falling into plantar flexion. ***
a. true b. false |
a. true
|
|
|
|
The stance phase of gait comprises the first 60% of a gait cycle. ***
a. true b. false |
a. true
|
|
|
|
If a person displays a compensated response to left hip abductor weakness, he or she will most likely lean the trunk to the left. ***
a. true b. false |
a. true
|
|
|
|
The foot flat portion of a gait cycle typically coincides with a position of double-limb support. ***
a. true b. false |
a. true
|
|
|
|
What is posture? ***
|
relative arrangement of body segments for specific activities
|
|
|
|
Ability to to assume various postures is dependent on an intact....***
|
- nervous system
- musculoskeletal system |
|
|
|
Posture is either _____ or _____. ***
|
- static
- dynamic |
|
|
|
Name some static postures. ***
|
- standing
- lying - sitting |
|
|
|
Name some dynamic postures. ***
|
- running
- walking - throwing - lifting |
|
|
|
What is postural control? ***
|
ability to maintain stability of body or body segments in response to external forces that threaten to disturb equilibrium (maintain your balance)
|
|
|
|
Advantages of bipedal stance ***
|
- frees up hands for tasking
- little energy expense by muscles because bones, joints, ligaments provide most of counteractivity to gravity (especially in static postures; body wants to conserve energy) - frequent changes in positions promotes circulatory return |
|
|
|
Disadvantages of bipedal stance ***
|
- increased work for the heart (pumping against gravity)
- increases weightbearing stresses on vertebral column, pelvis, LEs - decreases overall stability |
|
|
|
What is the BOS? ***
|
- base of support
- area formed under the body by connecting all points in contact with the ground - bipedal BOS is smaller than quadripedal - less stable |
|
|
|
What is COG? ***
|
- center of gravity (a.k.a. center of mass)
- hypothetical points at which all the body mass is concentrated and the point at which the object can be balanced - human COG is slightly anterior to the S-2 segment (different in water) - greatest stability with large BOS and low COG - small BOS and high COG for human body = unstable design |
|
|
|
What is the LOG? ***
|
- line of gravity
- action line of the gravitational forces on the body - vertical line drawn through the body’s COG - optimal erect posture |
|
|
|
What is postural sway? ***
|
- a constant swaying motion of the body during erect standing
- LOG continually shifts within BOS with postural swaying - requires constant fine adjustments of passive and active structures to counter changing gravitational forces and maintain balance (keeping LOG within BOS) |
|
|
|
Describe the LOG in optimal erect posture. ***
|
- when LOG passes directly through joint axis, there is no gravitational force on the segment
- body segments in near vertical alignment, compressive forces distributed optimally over all weightbearing joint surfaces - no excessive tension on muscles or ligaments - ideal posture does not exist in humans: LOG passes slightly away from most joint axes (but only a minimal amount) - you can’t balance without muscular stabilization |
|
|
|
Describe what happens when LOG passes some distance from joint axis. ***
|
- increase in pull of gravity on the segment
- the further the distance from the axis, the greater the gravitational force on segment - requires increased counter forces from passive and active structures at each of the involved joints to maintain erect posture |
|
|
|
Describe the anterior view of the body along a plumb line. ***
|
- plumb line bisects body into two symmetrical halves; bisects:
- head - face - sternum - vertebral bodies - pelvis - equidistance between knees and malleoli |
|
|
|
Describe the posterior view of the body along a plumb line. ***
|
- bisects body into two symmetrical halves
- bisects occiput, through spinous processes, gluteal cleft, - equidistance between knees and malleoli |
|
|
|
Describe the sagittal view of the body along a plumb line. ***
|
plumb line falls:
- though ear lobe - anterior to atlanto-occipital (AO) axis - anterior to cervical 5 joint axis - through acromion process - bisects the trunk - anterior to thoracic 4 joint axes - posterior to lumbar 4 joint axes - passes through greater trochanter - posterior to hip joint - passes anterior to midline of knee - anterior to knee joint - slightly anterior to lateral malleolus - anterior to ankle joint axis |
|
|
|
What are the goals of optimal posture? ***
|
- reduction of energy expenditure
- reduction of stress on supporting structures - each segment of the body is part of a closed kinematic chain - any change in position of one segment will cause changes to occur at other segments - changes from normal alignment cause abnormal stresses on structures which are not designed to take stress over prolonged periods |
|
|
|
How do sustained stresses over long time periods alter body structures? ***
|
- muscles/ligaments which are overstretched will weaken and lose passive tension (recoil)
- muscles in the shortened position will lose sarcomeres (thus size and strength), become weakened - muscles/ligaments in shortened position will become contracted and will limit full ROM - prolonged compressive forces on joints will cause degenerative changes of cartilage and bone (plastic deformation?) |
|
|
|
What two types of factors cause postural problems? ***
|
- postural
- structural |
|
|
|
What postural factors contribute to postural problems? ***
|
- poor postural habits
- muscle weakness/imbalance - occupational postures - pain - respiratory problems |
|
|
|
What structural factors contribute to postural problems? ***
|
- bony abnormalities
- leg length discrepancy - curvature of spine |
|
|
|
What are some common postural deviations? ***
|
- flexed-knee posture
- excessive anterior pelvic tilt - genu valgum - genu varum - foot and toe deformities - scoliosis |
|
|
|
What is flexed-knee posture? ***
|
- contractures cause increased hip flexion and ankle DF
- requires increased muscle activity of extensor muscle groups to counter gravitational movements |
|
|
|
What is excessive anterior pelvic tilt? ***
|
- hip flexion tightness increases anterior pelvic tilt, which causes:
- increased lumbar lordosis - exaggerated thoracic kyphotic curve which causes - exaggerated cervical lordotic curve to counter the malalignments |
|
|
|
What is genu valgum? ***
|
- a.k.a. knock knees
- associated with coxa vara - increased gravitational torque acting around knee ---- medially: abnormal tensile stresses ---- laterally: abnormal compressive stresses ---- ankle/foot: abnormal pronation affecting medial structures |
|
|
|
What is genu varum? ***
|
- a.k.a. bowed legs
- associated with coxa valga - increased gravitational torque acting around knee ---- medially: abnormal compressive stresses ---- laterally: abnormal tensile stresses ---- ankle/foot: abnormal supination affecting lateral structures |
|
|
|
Describe some foot and toe deformities. ***
|
- pes planus results in hypermobility in foot
- pes cavus results in decreased mobility in foot - results in claw toe (hyperextension of MTP, flexion of PIP/DIP) - hallux valgus results in lateral deviation of great toe (bunions) |
|
|
|
What is scoliosis? ***
|
- abnormal lateral curvature and rotation of vertebral column
- can occur in thoracic, lumbar, or thoracolumbar regions - causes: idiopathic - females > males - functional: related to habitual patterns or postures; usually job related (e.g., mail carriers, factory line workers) |
|
|
|
Anterior cervical triangle borders
|
- mandible
- sternocleidomastoids |
|
|
|
Anterior cervical triangle contents
|
- carotid artery
- jugular vein |
|
|
|
Axillary region borders
|
- pectorals
- serratus anterior - latissimus dorsi |
|
|
|
Axillary region contents
|
- brachial plexus
- brachial/axillary artery - brachial/axillary vein |
|
|
|
Cubital fossa borders
|
- brachioradialis
- pronator teres |
|
|
|
Cubital fossa contents
|
- biceps tendon
- brachial artery - median nerve |
|
|
|
Carpal tunnel borders
|
- flexor retinaculum
- carpals |
|
|
|
Carpal tunnel contents
|
- median nerve
- wrist flexor tendons (FDS, FDP, FPL) |
|
|
|
Femoral triangle borders
|
- inguinal ligament
- sartorius - adductor longus |
|
|
|
Femoral triangle contents
|
- femoral nerve
- femoral artery - femoral vein |
|
|
|
Popliteal fossa borders
|
- biceps femoris
- semitendinosus - semimembranosus - gastrocnemius |
|
|
|
Popliteal fossa contents
|
- common peroneal (fibular) nerve
- tibial nerve - popliteal artery - popliteal vein |
|
|
|
List some postural deviations of the back. ***
|
- hollow back
- flat ....... - slumping posture - military posture - round shoulders - high shoulder - high hip - head tilt - scoliosis |
|
|
|
What postural deviations occur at the head? ***
|
anterior view
- tilted or rotated head, mandible asymmetrical posterior view - tilted or rotated head lateral view - forward head |
|
|
|
What postural deviations occur at the cervical spine? ***
|
lateral view
- exaggerated curve - flattened curve |
|
|
|
What postural deviations occur at the shoulders? ***
|
anterior view
- elevated or depressed posterior view - elevated or depressed lateral view - rounded |
|
|
|
What postural deviations occur at the scapulae. ***
|
posterior
- abducted - adducted - winged |
|
|
|
What postural deviations occur at the thoracic spine? ***
|
posterior
- lateral deviation lateral - exaggerated curve |
|
|
|
What postural deviations occur at the lumbar spine? ***
|
posterior
- lateral deviation lateral - exaggerated curve - flattened curve |
|
|
|
What postural deviations occur at the pelvis? ***
|
posterior
- lateral pelvic tilt - pelvis rotated lateral - anterior pelvic tilt - posterior pelvic tilt |
|
|
|
What postural deviations occur at the hip? ***
|
anterior
- medially rotated - laterally rotated |
|
|
|
What postural deviations occur at the knee? ***
|
anterior
- external/internal tibial torsion posterior - genu varum/valgum lateral - genu recurvatum - flexed knee |
|
|
|
What postural deviations occur at the ankle/foot? ***
|
anterior
- claw toe - hammer toe - mallet toe posterior - pes planus - pes cavus lateral - forward posture - flattened longitudinal arch - exaggerated longitudinal arch |
|
|
|
Are the gait deviations actual diagnoses?
|
no
they are descriptors for documentation purposes |
|
|
|
Describe a foot slap gait.
|
foot quickly drops into plantar flexion and slaps the ground after heel strike
|
|
|
|
Reason for foot slap gait.
|
- weak dorsiflexors
- may follow injury to common peroneal nerve, distal neuropathy, or hemiplegia - dorsiflexors cannot slowly (eccentrically) control plantar flexion - loss of eccentric control of dorsiflexors |
|
|
|
Describe a high-stepping gait.
|
pt appears to be stepping over an imaginary obstacle
|
|
|
|
Reason for a high-stepping gait.
|
- marked weakness of dorsiflexors, resulting in foot drop
- to clear the foot from the ground, pt must excessively flex the hip and knee to advance the leg - loss of concentric control of dorsiflexors |
|
|
|
Describe a vaulting gait.
|
pt rises up on toes of stance foot to allow clearance for contralateral advancing limb
|
|
|
|
Reason for vaulting gait?
|
- any LE impairment that reduces ability to functionally reduce length of the advancing limb (e.g., inability to flex hip or knee)
- standing on tiptoes gives extra clearance to the long leg so it can clear the ground during swing - often occurs with other maneuvers for similar reasons (e.g., hip hiking and circumduction) |
|
|
|
Describe a weak quadriceps gait.
|
- knee remains fully extended throughout stance; combined with excessive forward lean of trunk
|
|
|
|
Reason for weak quadriceps gait?
|
- weakness or avoidance of activation of quadriceps muscle
- forward lean shifts LOG anterior to medial-lateral axis of knee, mechanically locking it in extension and reducing need for activation of quadriceps - may stress posterior capsule of knee and eventually lead to genu recurvatum |
|
|
|
Describe a genu recurvatum gait.
|
- severe plantar flexion contracture
- excessive hyperextension of knee during stance phase of gait - knee locked, plantar flexion and anterior pelvic tilt compensate |
|
|
|
Reason for genu recuvatum gait?
|
- long-term paralysis of the quadriceps with overstretched posterior capsule; may involve paralysis of knee flexors
- plantar flexion contracture |
|
|
|
Describe "crouched" (walking with hip or knee flexion) gait.
|
- hip and knee are flexed in stance phase (ankle in DF too, to compensate)
- often associated with increased lumbar lordosis and reduced stride length |
|
|
|
Reason for "crouched" (walking with hip or knee flexion) gait?
|
- may be due to severe pathologies such as spasticity or tightness of hip and knee flexor muscles, weakness of hip extensor muscles, pain, or joint limitations due to arthritis
- often seen with cerebral palsy - hip flexion contractures are in the hip adductor and IR muscles |
|
|
|
Describe a weak hip abductor gait.
|
uncompensated - when in single-limb support, pelvis leans toward side opposite the weak hip abductor muscles
compensated - when in single-limb support, trunk and pelvis lean to same side as weak hip abudctors, shortening the moment arm |
|
|
|
Reason for weak hip abductor gait?
|
- weak hip abductor muscles
- can be caused by Guillain-Barre, MD, polio, hip pain, arthritis, obesity, or any condition that reduces activation of hip abductors - uncompensated - hip drops = Trendelenberg sign - compensated - lessens burden on weak muscles |
|
|
|
Describe a weak gluteus maximus gait.
|
- backward lean of trunk during early stance phase
|
|
|
|
Reason for a weak gluteus maximus gait?
|
- weak hip extensors, such as gluteus maximus
- may be caused by polio - leaning the trunk back during stance shifts line of gravity posterior to hip, lessening the demand on the hip extensors (locking hip and hanging on the Ys) |
|
|
|
Describe a hip hiking gait.
|
- excessive elevation of pelvis on side of swing leg
- often occurs with other maneuvers for similar reasons (e.g., vaulting and circumduction) |
|
|
|
Reason for hip hiking gait?
|
- inability to functionally shorten the swing leg; hike provides the extra room for clearance
- may be due to weak hip flexor muscles |
|
|
|
Describe a hip circumduction gait.
|
- swing leg is advanced in semicircular arc to create clearance for the functionally long leg
|
|
|
|
Reason for hip circumduction gait?
|
- inability to functionally shorten swing leg
- may be due to reduced active or passive hip or knee flexion or due to wearing a "straight-leg" brace at knee - often occurs with other maneuvers for similar reasons (e.g., vaulting and hip hiking) |
|
|
|
What comprises the CNS? The PNS? ***
|
- brain and spinal cord
- all other nerve tissue (cranial nerves, spinal nerves, etc.) |
|
|
|
Describe the PNS. ***
|
- consists of all nervous tissue outside the vertebral canal
- formed by nerves leading to and from CNS - nerves contain axonal fibers which conduct afferent/efferent information - cranial nerves 12 (pairs) - spinal nerves 31 (pairs) (mixed) |
|
|
|
Regions of a peripheral nerve ***
|
- spinal cord (in vertebral canal) gives rise to the ventral and dorsal roots at each segmental level
- ventral and dorsal roots formed bilaterally from cord - roots join while in vertebral canal, form a single spinal nerve, pass out of vertebral canal via intervertebral foramen |
|
|
|
Difference between ventral roots and dorsal roots ***
|
- ventral root (outgoing motor axon fibers)
- dorsal root (incoming sensory axon fibers) |
|
|
|
What happens once spinal nerves pass outside the intervertebral canal? ***
|
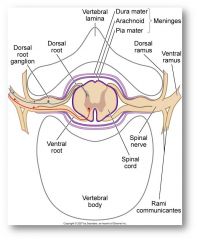
- once outside of intervertebral canal, spinal nerve immediately splits into 2 branches (rami)
- anterior (ventral) ramus – innervates autonomic nervous system, BUE/BLE and anterior/lateral aspects of trunk - posterior (dorsal) ramus innervates posterior trunk |
|
|
|
What is the function of the anterior (ventral) ramus? The posterior (dorsal) ramus? ***
|
- anterior (ventral) ramus – innervates autonomic nervous system, BUE/BLE and anterior/lateral aspects of trunk
- posterior (dorsal) ramus innervates posterior trunk |
|
|
|
Peripheral nerves contain nerve fibers which innervate both... ***
|
- visceral organs and
- somatic (skeletal muscle, joints, bones, skin) structures |
|
|
|
Composition (layers) of a peripheral nerve ***
|
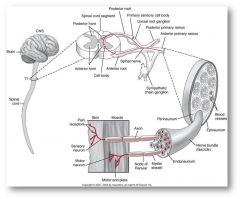
- made up of myelinated and/or unmyelinated axons which transmit either sensory or motor information
- mixed axons (myelinated/unmyelinated/sensory/motor) are each surrounded by a connective tissue sheath called endoneurium (inner) and then are grouped into bundles called fasiculi - each fasciculus is surrounded by a connective tissue sheath called a perineurium - entire nerve in comprised of many fasiculi and is surrounded by tough connective tissue sheath called epineurium (over) (contains fat cells and small blood vessels) |
|
|
|
Endoneurium ***
|
surrounds individual axon
|
|
|
|
Perineurium ***
|
surrounds individual fascicle
|
|
|
|
Epineurium ***
|
surrounds entire nerve
|
|
|
|
What is a nerve plexus? ***
|
- a network of spinal nerves in one region
- anterior (ventral) rami of the spinal nerves join together, intermingle, split and regroup to form a network - peripheral nerves are formed from each plexus - at every level except thoracic (direct innervation) |
|
|
|
At which spinal level are there no plexuses? ***
|
- thoracic (direct innervation)
|
|
|
|
What are the four major plexuses? ***
|
- cervical
- brachial - lumbosacral - coccygeal |
|
|
|
Cervical plexus (general) ***
|
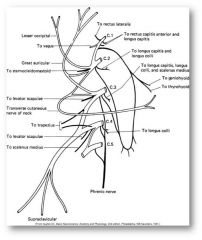
- C1-C4 spinal nerves
- innervates muscles of the neck and diaphragm |
|
|
|
Brachial plexus (general) ***
|
- C5-T1
- innervates muscles of the scapula and UE |
|
|
|
Lumbosacral plexus (general) ***
|
- L1-S3 or T12-S3
- innervates muscles of LE ---- lumbar division (L1-L4) or (T12-L4) ---- sacral division (L4-S3) |
|
|
|
Coccygeal plexus (general) ***
|
- S3 – coccyx
- innervates muscles of the genitalia and perineum |
|
|
|
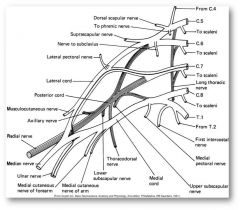
Brachial plexus specific innervations ***
|
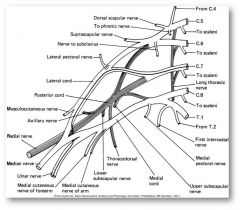
- all scapular nerves: scapular muscles (C5-6)
- thoracodorsal nerve: lattisimus dorsi (C6-8) - pectoral nerve: pectoralis major (C5-T1) - axillary nerve: deltoid, teres minor (C5-6) - musculotaneous nerve: biceps, brachialis, coracobrachialis - radial nerve: triceps, wrist/finger extensors, supinator, brachioradialis (C5-C8) - median nerve: pronators, FCR, FDS, FDP (radial side), thumb opposition, flexion, abduction, lumbricals 1,2 (C6-T1) - ulnar nerve: FCU, FDP (ulnar side), interossei, lumbricals 4, 5 (C8 – T1) |
|
|
|
Lumbosacral plexus specific innervations ***
|
lumbar division (L1-S3)
- obturator nerve: hip adductors - femoral nerve: hip flexors, quadriceps sacral division (L4-S3) - inferior gluteal nerve: gluteus maximus - superior gluteal nerve: gluteus medius/minimus, TFL - sciatic nerve: hamstrings ---- tibial nerve: plantar flexors, posterior tibialis ---- common peroneal (fibular) nerve: no muscles directly -------- superficial peroneal (fibular) nerve: peroneus longus/brevis -------- deep peroneal (fibular) nerve: tibialis anterior, toe extensors |
|
|
|
Lumbar division of lumbosacral plexus ***
|
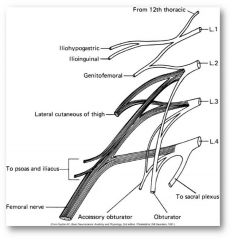
lumbar division (L1-S3)
- obturator nerve: hip adductors - femoral nerve: hip flexors, quadriceps |
|
|
|
Sacral division of lumbosacral plexus ***
|
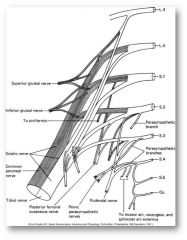
sacral division (L4-S3)
- inferior gluteal nerve: gluteus maximus - superior gluteal nerve: gluteus medius/minimus, TFL - sciatic nerve: hamstrings ---- tibial nerve: plantar flexors, posterior tibialis ---- common peroneal (fibular) nerve: no muscles directly -------- superficial peroneal (fibular) nerve: peroneus longus/brevis -------- deep peroneal (fibular) nerve: tibialis anterior, toe extensors |
|
|
|
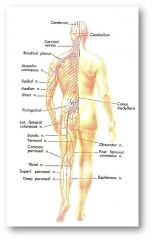
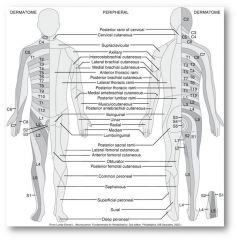
Cutaneous sensory distribution: ***
peripheral nerves |
innervate specific muscles and they also innervate specific cutaneous areas
[these areas are different from dermatomal areas; cutaneous areas (nerve fields) are sensory areas innervated by peripheral nerves] |
|
|
|
Cutaneous sensory distribution: ***
axillary nerve |
lateral arm over lower 2/3 of deltoid
|
|
|
|
Cutaneous sensory distribution: ***
musculocutaneous nerve |
lateral surface of forearm
|
|
|
|
Cutaneous sensory distribution: ***
median nerve |
- radial half of palm
- palmar aspect of thumb - digits 2,3,4 (radial side) - dorsum of finger tips 2,3 |
|
|
|
Cutaneous sensory distribution: ***
ulnar nerve |
- ulnar side of hand
- thumb - digits 2,3,4 (radial side) |
|
|
|
Cutaneous sensory distribution: ***
obturator nerve |
- middle of medial thigh
- medioposterior aspect of thigh and knee |
|
|
|
Cutaneous sensory distribution: ***
sciatic nerve |
no sensory directly
|
|
|
|
Cutaneous sensory distribution: ***
tibial nerve |
(medial/lateral plantar nerve)
- posteriolateral aspect of lower leg - sole of foot |
|
|
|
Cutaneous sensory distribution: ***
common peroneal nerve |
lateral aspect of lower leg just below knee level
|
|
|
|
Cutaneous sensory distribution: ***
superficial peroneal nerve |
- anteriolateral lower leg
- dorsum of ankle and foot |
|
|
|
Cutaneous sensory distribution: ***
deep peroneal nerve |
- triangle over dorsum of distal metatarsals 1 and 2
|
|
|
|
What are some clinical signs of injury to a peripheral nerve? ***
|
- sensory and motor impairments
- sensory impairment: ----if the area of sensory impairment follows a dermatomal pattern, then lesion is proximal (spinal nerve/nerve root injury) Ex: HNP with spinal nerve root impingement ---- if area of sensory impairment follows cutaneous pattern (nerve field) then lesion is distal and is PNI. EX: entrapment, trauma, compression |
|
|
|
Signs and symptoms of peripheral nerve injuries (PNI) ***
|
- loss of sensation
- paresthesias - pain - muscle weakness - muscle paralysis |
|
|
|
Classifications of PNI ***
general |
- stretch (neurapraxia)
- neuroma - rupture - avulsion - compression |
|
|
|
Classifications of PNI ***
stretch |
- shocks nerve, but does not tear
- usually heals within 3 months |
|
|
|
Classifications of PNI ***
neuroma |
scar that develops due to injury
|
|
|
|
Classifications of PNI ***
rupture |
complete disruption of nerve
(requires surgical intervention; graft) |
|
|
|
Classifications of PNI ***
avulsion |
nerve torn from spinal cord
|
|
|
|
Classifications of PNI ***
compression |
pressure causes myelin breakdown
|
|
|
|
Causes of PNI ***
|
nerve entrapment/compression due to:
- inflammation/edema of surrounding soft tissue - bony impingement - tight cast - poor positioning - trauma: lacerations, stretching, fractures - disease process: viral infection, arthritis, vascular insufficiency |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- axillary |
- shoulder abduction
- shoulder flexion - shoulder extension |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- musculocutaneous |
- elbow flexion
- supination |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- median |
- pronation
- thumb opposition - thumb flexion - thumb abduction |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- radial |
- elbow extension
- wrist extension - finger extension - thumb extension |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- ulnar |
- wrist flexion
- finger flexion - intrinsics (lumbricals, interossei) |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- femoral |
- hip flexion
- knee extension |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- obturator |
- hip adduction
|
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- sciatic |
- hip extension
- knee flexion - actions of tibial, peroneal |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- tibial |
- plantar flexion
- inversion - toe flexion |
|
|
|
Clinical signs of injury to individual peripheral nerves (motor):
- common peroneal |
- dorsiflexion
- eversion - toe extension |
|
|
|
Name eight common PNI ***
|
- compression of long thoracic nerve
- entrapment of/trauma to radial nerve - entrapment/compression of ulnar and median nerves - entrapment of sciatic nerve - compression of tibial nerve - compression of common peroneal nerve - Morton's neuroma - diabetic neuropathy |
|
|
|
Compression of long thoracic nerve ***
|
- serratus anterior: stabilizes scapula against chest wall
- deficit: winging of scapula |
|
|
|
Entrapment of/direct trauma to radial nerve ***
|
- triceps, wrist and finger extensors
- deficit: drop wrist (usually distal to triceps) |
|
|
|
Entrapment/compression of ulnar and median nerves ***
|
- wrist/finger flexors, intrinsics: wrist/finger flexion, abduction/adduction, and flexion of MCP/extension of IPs
- if ulnar nerve only: cubital tunnel = ulnar wrist and hand (claw hand) - if median nerve only: CTS - atrophy of thenar eminence (median nerve) - benediction hand (median nerve) |
|
|
|
Entrapment of sciatic nerve ***
|
- a.k.a. piriformis syndrome
- hamstrings, plantar flexors, dorsiflexors, toe flexors and extensors - deficit: weakness in hip extension, knee flexion, PF, toe flex |
|
|
|
Compression of tibial nerve ***
|
- (popliteal fossa, baker’s cyst)
- triceps surae: tibialis posterior, toe flexors, PF, invertors - deficits: absence of above actions, no push off with gait |
|
|
|
Compression of common peroneal nerve ***
|
- peroneals, anterior tibialis, toe extensor, everters, DF
- deficits: inability to DF foot during gait, drop foot, steppage gait |
|
|
|
Morton's neuroma ***
|
enlargement of conjoined lateral and medial plantar nerve may be caused by high heels or pes planus
|
|
|
|
Diabetic neuropathy ***
|
- damage to nerves due to elevated blood glucose
- decreased sensation (stocking glove) – does not follow pathway of ulnar/median/radial nerves - due to lack of nutrition |
|
|
|
Divisions of human circulatory system ***
|
- pulmonary system: blood circulates through lungs (gas exchange)
- systemic system: blood circulated through heart, brain, organs and all other body tissues |
|
|
|
Peripheral vascular system of head, trunk and extremities ***
|
- arterial and venous systems supply blood to the head/trunk, upper and lower extremities
- deep veins enclosed in same connective tissue sheaths with the arteries they accompany - superficial veins immediately under the skin and communicate with deep veins - major peripheral arteries and veins often have same names |
|
|
|
Major vascular structures of upper extremity ***
arterial |
- aorta
- subclavian artery - axillary artery - brachial artery - radial/ulnar artery - digital arteries - capillaries |
|
|
|
Major vascular structures of upper extremity ***
venous |
- capillaries
- digital veins - radial/ulnar veins - brachial/deep basilic/cephalic vein - axillary vein - subclavian vein - superior vena cava |
|
|
|
Major vascular structures of lower extremity ***
arterial |
- aorta
- common iliac artery - internal/external iliac artery - femoral artery - popliteal artery - anterior/posterior tibialis (peroneal) artery - digital arteries - capillaries |
|
|
|
Major vascular structures of lower extremity ***
venous |
- capillaries
- veins - anterior/posterior tibialis, peroneal - saphenous (superficial); popliteal (deep) veins - femoral vein - internal/external iliac veins - common iliac vein - inferior vena cava |
|