![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
68 Cards in this Set
- Front
- Back
|
Mirror neurons |
Neurons fire similarly when a task is perceived and when the task is produced. Used to anticipate what someone else will do, learn a new task (sound & sight). Ex: expert watchers and elite players will both have hand cortex activation when watching free throws. Neurons in ventral premotor cortex (F5) during prod of complex actions |
|
|
What is particular about the left hemi in action? |
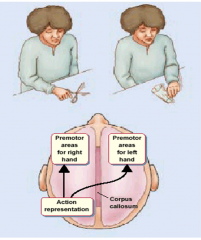
"Lefthemisphere contains movement formulas that bilaterallyprogram the selection, timing, and spatial relationships of skilledmovements." |
|
|
Secondary/association neural region for motor |
translation of goals into motor codes; formation of sequential reps. abstract spatial reps of action goals |
|
|
Apraxia |
Loss of ability to generate coordinated, purposeful actions NOT due to a loss of muscle control. This is a problem making coordinated gestures, especially apparent when miming actions (i.e. whistling, saluting, ..) This is usually a left-hemi injury. Assess these with motor(show me how to open door with key) +perception test(show me which pic shows that) (posterior apraxia does best on this) |
|
|
ideomotor apraxia vs ideational apraxia |
Ideomotor apraxia: Difficultyin carrying out commands, producing coherent actions, esp. with complex sequential actions. Ideational apraxia: Loss of knowledge about actions and how they are used to manipulate objects. More severe problem. Linked to parietal area (would not recognize correct action)` |
|
|
Cerebellum |
Coordinating movements in time, learning to adapt movement (to things like wearing prism glasses). Fine turning of motor signals for feedback, timing muscular commands. |
|
|
How does the brain coordinate movement to agonist and antagonist muscles? What happens with this and cerebellar damage? |
People with cerebellar movements overshoot agonist intensity and therefore overshoot arm location. They pull back and overshoot return area. It continues this way with a smaller error each time until the right spot is reached. Motor learning abolished in cerebellar lesion, never learns to adapt movement |
|
|
Ataxia |
Ataxia: impairment of coordination despite intact knowledge of appropriate action |
|
|
What kind of memory makes up nondeclarative memory? |
procedural, perceptural representation system, classical conditioning (conditioned responses between two stimuli), nonassociative learning (habituation, sensitization |
|
|
Amnesia |
loss of memory that affects all of the senses. Anterograde: partial or total loss of mem for events after neuro disturbance - prob w/ learning new things. Retrograde amnesia: loss of mem for events prior to neuro disturbance - prob w/ mem |
|
|
Clive wearing & anterograde amnesia |
clive had bilateral hippocampal lesions and inferior prefrontal damage. He has anterograde amnesia: associated with medial temporal lobe region (hippocampus. anygdala, and surrounding cortex) |
|
|
Hippocampus in memory encoding |
Hippocampusis critical for forming declarative memories. Correct recollections trigger activity in medial temporal lobe and frontal cortex compared to forgotten words. Parahippocampus - remember > forget at onset of event. RightTPJunction - remember > forget when facts available. |
|
|
Consolidation theory |
hippocampus (acquisition of declarative memory) is part of a network for developing associations between representations in different cortical areas in which the hippocampus is eventually not needed to activate different information about a memory- a process model. Hippocampus is thought to strengthen connections between other neurons |
|
|
LTP |
giving a burst of electric stimulation to a neuron in the hippocampus, it takes less and less stimulation for that neuron to fire. The three rules of neuronal LTP: cooperativity (more than one input must be active at the same time), associativity (weak with strong co-occur), and specificity (only that synapse is potentiated) |
|
|
What is the key component to memory and skill? |
Stability! This stable long term memory is obtained through consolidation (memories are strengthened and stabilized, increasing resistance to interference and decay) |
|
|
What happens in the absence of sleep? |
Impaired working mem, decreased arousal, increased RT to stimuli. |
|
|
What are the key assumptions of the consolidation theory? |
Consolidation is an active process. and consolidation strengthens memory representation |
|
|
Stages of sleep |
Alert wakefulness (beta waves) > just before sleep (alpha waves) > stage 1 (theta waves) > stage 2 (sleep spindles & k complexes) > stages 3/4 (delta waves), slow wave sleep, deepest > REM. Go down stages and back up before first REM. Stage 3 is longest early and gets slower and the opposite for REM |
|
|
Define polysomnography |
records brain waves, heart rate, breathing, blood oxygen levels, as well as eye and leg movements during sleep |
|
|
Tasks to judge effect of sleep on skill: sensorimotor learning, sequential finger tapping, and perceptual learning of synthetic speech. |
sensorimotor learning (navigate virtual environment in FPSG - different maps. Participants that napped learned better), sequential finger tapping(sequence of nums to tap as quickly + correctly as poss. Sleep improves skill), and perceptual learning of synthetic speech(explained in depth on another side). |
|
|
perceptual learning of synthetic speech |
Speech generated by computer which is at first difficult, but users quickly improve. Design: Control control: take test after training. Control AM: AM training, 12 hour wake & then pretest. Waking interval, and then is given post test. Control PM: trainingn in PM, 12 hours sleep, post test. Findings: Wake perentage pts improvement signif lower than other controls. Sleep stablizes learning, performance decreases across waking interval |
|
|
Does sleep affect a memory that decays over a waking interval? |
Now have 24 AM and 24 PM groups for perceptual learning of synthetic speech. Have a wake interval and a sleep interval and then take the test. Since both of these groups performed about the same, we can see that sleep helps |
|
|
Sleep and skill |
Stabilizes performane. Protects learning from decay or loss, and recovers or restores memories that appear to have been lost over the course of the day |
|
|
Paired associates task |
Participants asked to learn pairs of words and then were taking a cued recall test, where feedback was given for each pair. Another of these test were given 12 hours later with wake & sleep groups. People must get 60% correct to move forward. Ppl better at test II when have slept (recalling more word pairs than they did initially on test I after 12 hours) wake group is the same |
|
|
Sleep and declaritive mem |
Sleep increases recall of paired associates. There is no sig change in performance after an equal interval of wakefulness. Improvement in declarative mem is related to SWS and sleep spindles |
|
|
Sleep - Passive or active protection against interference (how) |
Learning associated word pairs. 12 hr delay for wake/sleep. one half of each group does an interference task (learning new associations, instead of table-blanket, learn blanket-tool), the non interference is tested again. Interference test: retreive initial pair. |
|
|
Sleep - Passive or active protection against interference (results) |
Sleep group is recalling more word pairs than wake group (non interference). Interference - do much worse when exposed to interference than when not. The sleep group is not particularly affected by interference (-10%), but wake interfered is very affected. Suggests that sleep is providing a more active protection against interference |
|
|
Reactivation/replay |
Information squired or learned during he day is reprocessed or reactivated during sleep. Reflect transfer of info from hippocampus to cortex. Firing rates of place cells indicate location in environment (there is overlap in areas) |
|
|
Replay& hippocampus |
Replay is associated with high freq bursts in hippocampus, called sharp wave ripple activity (and with sleep spindles). There are related to slow oscillations arising from frontal networks during SWS. Coupling of activity between hippocampus and cortex may reflect transfer or information |
|
|
Replay in humans |
Hippocampal activity was greater during sleep after navigation than after control task. Navigation improvement after sleep was correlated with hippocampal activation during sleep |
|
|
Predications of reactivation theory |
1. increasing slow oscillations should increase reactivation 2. reactivation should increase consolidation across sleep 3. if this process reflects transfer of information from the hippocampus to the cortex than there should be a reduction in hippocampal activation after consolidation |
|
|
testing predictions of the reactivation theory(1&2) |
Increasing slow oscillations artificially vai 4 frontal electrodes: increases spindle activity, and increases declarative memory consolidation during sleep |
|
|
testing predictions of the reactivation theory - 3 |
ppl studiest 90 word pairs and were given a cued recall test after learning whiele in an fMRI scanner. ppl then either slept or stayed awake for a night. After 2 days (have a night of recovery sleep) and after 6 months, all ppl were given another cued recall test. Improvement after 2 days but not after 6 mo |
|
|
Task to investigate altering of consolidation |
Ppl learned a visuospatial loc task while presented with a rose odor. Rose odor was presented again during sleep in order to reactivate memory for the task. In I: rose during learning and SWS. II: during SWS. III: during learning and REM sleep. IV: during learning and waking interval prior to sleep |
|
|
results of Task to investigate altering of consolidation |
Providing a contextual cue during consolidation can increase consolidation. Odor presented during sleep can increase hippocampal activation and may serve to increase reactivation |
|
|
What are the extrapyramidal tracts and where do they originate? |
The extrapyramidal tracts are the rubiospinal from the bright red nucleus, the tectospinal from the superior colliculus, the vestibulospinal from the vestibular nucleus, and the reticulospinal from the reticular formation
|
|
|
Tell me about the pyramidal tract |
The corticospinal tract is 90% crossed, 10% uncrossed. It is direct control of individual muscles and here the longest neurons in the brain synapse on alpha motor neurons(that synapse on muscle fibers) or interneurons. It travels from the motor cortex > midbrain > medulla >(cross after medulliary pyramids)> spinal cord |
|
|
Anatomy of skeletal muscles |
Alpha motor neurons synapse on muscle fibers. In the ventral root of the spinal cord, the alpha motor neurons are synapsed upon by stretch receptors (on muscle spindles) that enter through the dorsal root. This prevents overstretching of muscles by contracting them some when the stretch becomes potentially dangerous. |
|
|
Primary motor cortex (M1) |
Execution of movement. M1 neurons show directional tuning (records high activity for preferred direction and less for closer but no cigar). Computes simple movement codes in terms of muscles, movement direction |
|
|
Population vector |
Decribes activity across many neurons each tuned to a preferred direction. Movement of animal is function of summed activity over all of the cells. Provides excellent predictor of movement direction with even small groups of neurons. |
|
|
Muscle tuning of an M1 neuron |
Preferred direction is usually confounded with muscle activity. Direction: external reference frame. Muscle: internal reference frame. MEthod to test if representation is direction or msucle: looking at neurons that fire for a direction regardless of the muscles used for that action (have do the same action with different muscles) and same but opposite elationships |
|
|
Hemiplegia vs hemiparesis: |
hemiplegia: loss of voluntary movement in contralateral limb(s). Hemiparesis: weakness, impaired control of contralateral limb(S) |
|
|
Secondary and association areas (motor) |
Premotor cortex: externally-guided movement. Supplamentary motor area: internally-guided movements. SMA&Premotor: body-centered reference frame and unconscious motor planning. Parietal: how to move in space (i.e. reaching) - eye-centered reference frame, conscious intention to move and movement goals. |
|
|
How do we know that action plans are not tied to a particular effector? |
A signature will look very similar if written by the right or left hand, mouth, or foot |
|
|
What do supp motor areas do? How do we know this? |
They represent and construct action plans for sequences of simple movement (independent muscle movements show in M1). We know this because TMS to SMA shows errors only in complex hand moving task, reported errors like "i forgot where i was in seq" whereas errors in simple and complex hand task was seen in TMS stimulation of M1 ("my hand got stuck") |
|
|
Cerebellar organization |

Medial cerebellar cells (spinocerebellum) code motor execution to descending systems. Lateral cerebellar neurons (neocerebellum/cortex) code motor planning to motor and premotor cortices, and the vestibulocerebellum balances and coordinates eye movements to vestibular nuclei. |
|
|
Basal ganglia - direct & indirect pathways |
Initiation of state changes(motor or cognitive). direct: Excites cortex. Cortex > striatum > GPi, SN > thalamus > cortex. InDirect: Inhibits cortex. Cortex > striatum > GPe > STN > GPi, SN > thalamus > cortex |
|
|
Computational model of basal ganglia's role in movement initiation |
The inhibitory output of the basalganglia keeps potential responses in check until activation for one of theoptions reaches a threshold, resulting in the initiation of that movement. Bythis model, “selection” occurs even though the basal ganglia need not evaluatethe possible choices, but rather, only monitors their activation level. |
|
|
Parkinson's disease: akineasia |
Akinesia: loss or impairment of the power of voluntary movement. PD patients would learn two finger-tap seqs. When given AA, PD patients had an RT comparable to controls. When asked to shift to a different sequence, the RT of PD patients is MUCH HIGHER than controls |
|
|
Bradyphrenia |
Problems in shifting cognitive state associated with being a PD patient (wanted patients to respond to shapes w/color or shape. No shift: shape, shape. shift: color, shape. PD patients showed a significantly higher RT for the shifted condition |
|
|
Tell me about Parkinson's disease |
Characterized by a loss of dopaminergic projections from the sunstantia nigra to the striatum (therefore no dopamine is activating the pathways where prev was here). Stronger activation is now required to trigger the same action. |
|
|
Affordance competition |
Multiple action plans compete for selection.Two populations of neurons both fire until something makes it evident that one of the two pathways should be selected. The other pathways dies in firing and the first begins to fire rapidly |
|
|
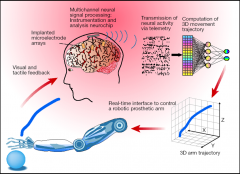
Paraplegia vs quadraplegia |
Paraplegia(lower body) or Quadraplegia (all four limbs depending on level of damge) caused by damage to the spinal cord |
|
|
Brain machine interface - neuroprosthetics brain |
|
|
|
Medial temporal lobe and memory acquisition |
Medial temporal lobe region/hippocampus associatedwithacquisition of declarative memory, a Descriptive account |
|
|
Computational implications of consolidation theory |
Provides process-based account of the kinds of memory that should be spared following MTL lesions: changes that occur within a cortical region, priming (reactivation of perceptual trace), and motor skills (associations of successive motor commands within primary and/or secondary motor areas |
|
|
Brain structures associated with anterograde amnesia: |
Medial temporal lobe region, diencephalon (thalamus and mammilary bodies), and Korsakoff's disease caused by a lack of thiamine (vitamin B1) |
|
|
Korsakoff's disease |
caused by lack of thiamine (vitamin B1) usually caused by alcohol misuse. Usually preceded by Wernicke encephalopathy is a medical emergency that causes life-threatening brain disruption, confusion, staggering and stumbling, lack of coordination, and abnormal involuntary eye movements. Korsakoff syndrome causes problems learning new information, inability to remember recent events and long-term memory gaps. These patients will make up information that they do not know |
|
|
Brain structures associated with retrograde amnesia |
Cerebral cortex: memories are stored throughout the brain. It is not possible to wipe out all memory. Focal lesions can cause specific memory deficits (anomia - loss of word mem, prosopagnosia..) |
|
|
Alzheimer's disease |
Associated with anterograde and retrograde amnesia. Retrograde becomes worse with time. Has a cortical and subcortical pathology due to widespread damage, although the hippocampus degenerates more rapidly |
|
|
What did we learn from HM? |
Due to HM, there was a shift from focusing on localizing specific memories to a focus on the study of the memory process that emphasized that storage of memory could be distinct from formation of memory |
|
|
How do amnesiacs perform on non-declarative memory tasks? |
Amnesics also show normal learning on sequence task (procedural learning) |
|
|
Patient evidence favoring separate systems for declarative and non-declarative memory |
Threshold reading task: study word list. Test phase: Determine the min threshold for identifying words (old and new), priming helps identify old words. Then there is a recognition phase. This test revealed that declarative and non-delcarative memory rely on different systems. |
|
|
Semantic v episodic |
Semantic memory can be kept intact without the associated episodic memory intact |
|
|
What occurs if the inhibition to the antagonist muscle does not occur? |
The arm will return to its initial position because the stretch that occurs at the contraction of the bicep (in this case) causes the tricep to stretch. The stretch reflex then pulls your arm back to its original position |
|
|
|
parietal cortex - abstract planning of motor goals. SMA & premotor cortex - repspon. Motor cortex - execute movements |
|
|
Nondeclarative vs declarative for Parkinson’sdisease vs amnesics |
Task: implicit learning through trial and error: which of these cards results in a sunny day or rainy day. Get a card, guess rain or shine until you learn which is which (each card have diff probs for each weather thing). Amnesic subjects get better and better at this while the PD patients do not show procedural learning here. The other part of the task was asking the patients questions about the session. Amnesics could nto answer these questions, while PD patients performed just fine in this area. Double dissociations between performance and knowledge |
|
|
How do apraxia and ataxia differ |
Apraxia: problem in generating coordinated, purposeful actions due to loss of muscle control (especially in mimicing). Ataxia: problems in coordinating fluid movements (poor timing and coordination) |