![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back

Define what Retained Foetal membranes are? |
Partial or completely retained membranes >12 hours post partrum. Failure of normal third stage labour. |
|

What is the incidences of RFM in most herds? |
3-10% |
|
|
Aetiology of RFM? |
Failure of the foetal cotyledonary villi to seperate from the maternal caruncles and/or primary uterine inertia. |
|

What are factors predisposing to RFM? |
1) Premature parturition- Immature placentomes -twins, late abortions, induced births (Steroids) 2) Oedema of the chorionic villi due to trauma- dystocia, caesarean, following uterine tosion. 3) Pathological inflammation- e.g. placentitis by bacillus licheniformis 4) Uterine inertia- Hypocalcaemia, hyposelenaemia, hydrops, twins. |
|

Clinical signs of retained foetal membranes? |
Putrid placenta handing out from vulva can be inside also. She may be straining to pass the placenta. Usually not systemically unwell unless she develops puerperal metritis. |
|

Sequalae of events of retained foetal membranes? |
Spontaneous expulsion usually after 5-10 days. Can go on to develop acute puerperal metritis as the RFM decrease phagocytic function. No impact on fertility unless associated with metritis. |
|
|
Methods to treat a cow with RFM? |
1) Manual removal 2) Ecbolic drugs- Oxytocin, PGF2a, calcium salts. 3) Intrauterine antibiotics/ pessaries. 4) Systemic antibiotics. |
|
|
How do we manually treat RFM? |
Gentle manual traction only. Best attempt manual removal 3-5 days after. C/I if doesnt come away easily or with metritis. |
|
|
What is the incidence of cystic ovarian disease in cattle? |
5-30% Usually 20-60 days post partrum. Often in 2nd-3rd lactation high yielding cows. |
|
|
What are the economic and production implications of cystic ovarian disease? |
Takes longer to get a cow in calf so leads to financial losses. |
|

What is the definition of cystic ovarian disease? |
Fluid filled structure >2.5 cm in diameter present for >10 days on one or both ovaries in the absence of a CL. |
|
|
Name the two types of cysts? |
1) Follicular cysts. 2) Luteinised/ Luteal cysts. |
|

What are follicular cysts? |
Thin walled, non progesterone producing cysts. |
|

What are luteinised cysts? |
Thicker walled, progesterone producing, look like doughnuts. |
|
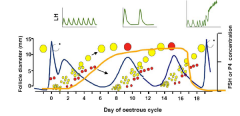
Aetiology of cystic ovarian disease? |
Failure of the LH surge around time of normal ovulation. Or Failure of a follicle to respond to LH. The follicle thus fails to ovulate becomes atretic continues to grow and forms a cyst. |
|

What are reasons for failure of the LH surge?
|
1) Stress!!!!!! 2) Metritis/endometritis. 3) B- carotene deficiency- High conc/ low greens. 4) Plant based oestrogens. |
|
|
How does stress lead to a failure of the LH surge? Examples of stress? |
Causes the release of CORTISOL which interferes with hypothalmus/pituatary interaction and blocks or delays normal LH surge or may alter LH receptor activity.
NEB Change of diet. High yield. Transport. |
|
Clinical signs of follicular cysts? |
Anoestrus mainly.
Occasional nymphomania- irregular or recurrent oestrus. |
|
|
Signs of luteal cysts? |
Anoestrus |
|

How can we diagnose ovarian cystic disease? |
Most detected on routine pp checks. Rectal palpation. Milk/blood progesterone assay - <2ng/ml follicular cyst > this luteal cyst. Rectal ultrasound. |
|

|
Follicular cyst and normal follicle. |
|

|
Lutenized cyst and a normal follicle. |
|
|
How can we treat a cow with a cyst? |
GnRH- induces the LH surge. Human chorionic gonadotrophic hormone. Progesterone- Prid/cidr. Prostaglandin F2a. Manual rupture. |
|
|
If you are absolutely positive the cyst is luteal what can we use to get rid of it? |
Prostaglandin. |
|
|
If positive it is a follicular cyst what can we use to treat it? |
Prid/cidr for 10-12 days then remove and get oestrous in 2-3 days. |
|
|
If you are unsure of the cyst type how can you treat it? |
GnRH +/- PG in 7-14 days if not seen in oestrus insert a PRID/CIDR for 10-12 days and inject PG on removal |