Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
160 Cards in this Set
- Front
- Back
|
Normal thyroid follicles are filled with what gel like substance?
|
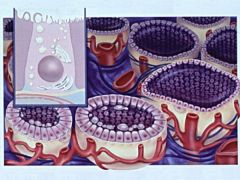
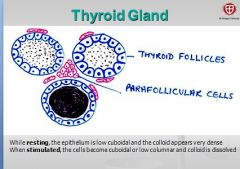
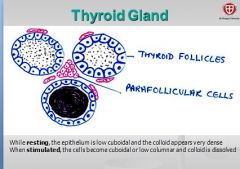
Filled with gel-like substance (colloid) and lined by cuboidal follicular cells.
- colloid is the secretory product of the follicular cell (extracellular storage!). |
|
|
When thyroid cells stimulated, what hormone is released?
|
Secretes thyroid hormones THYROXIN
FYI: When stimulated, epithelium becomes cuboidal or low columnar and colloid is dissolved. |
|
|
Parafollicular cells of the thyroid gland secrete what? function?
|
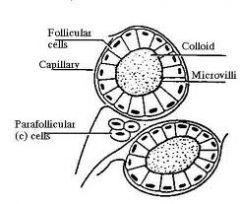
occur as single cells in the basal lamina of the follicle. Cells secrete Calcitonin (lowers blood calcium levels by suppressing bone resorption)
FYI: bone resorption = bone broken down and Ca+ released |
|
|
what is function of calcitonin?
where secreted from? |
Parafollicular cells of the THYROID secrete calcitonin which LOWERS blood calcium level by suppressing bone resorption
-so counteracts break down of bone by PTH (remember PTH = incr blood calcium, incr. bone resorption/remodeling) ~when think of calcitonin, think of making bone |
|
|
major integrating link between the
nervous and the endocrine systems. |
HYPOTHALAMUS
|
|
|
receives input from various other CNS regions such as ? (6)
|
input from -> e.g. thalamus, limbic system, cortex, RAS, and sensory signals from viscera and the eye.
|
|
|
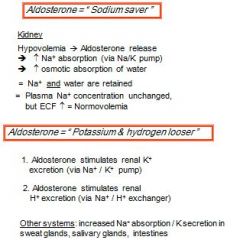
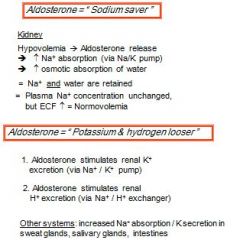
What does aldersterone do?
What ion absorption does it promote? At expense of what? |
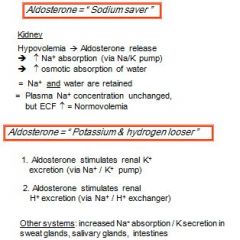
Aldosterone acts mainly on distal tubules and collecting ducts of nephron; stimulates:
- Aldosterone is a SODIUM SAVER! = promotes sodium absorption and K+ loss (Na/K pump) - Hydrogen loss (via renal Na+ / H+ exchanger) |
|
|
Part of CNS involved in emotions, stress, fear, control of hunger, thirst, sexual behaviour?
|
HYPOTHALAMUS
|
|
|
Part of CNS that largely controls homeostasis, e.g. osmolality, body temperature, and controls the autonomic nervous system?
|
HYPOTHALAMUS
|
|
|
is a “master” endocrine gland.
|
The Hypothalamus is a “master” endocrine gland. Its many neuroendocrines influence other CNS areas as well as various peripheral endocrine glands via the Pituitary Gland.
(in past learned pituitary gland is master but this prof says otherwise) |
|
|
The Hypothalamus is connected with the PITUITARY GLAND via the
|
hypophyseal stalk.
|
|
|
PITUITARY GLAND consists of what 2 parts?
|
1. ANTERIOR pituitary
2. POSTERIOR pituitary |
|
|
neurohypophysis extension of the hypothalamus is which part of pit.gland?
What tissues/structures does it have? |
POSTERIOR pituitary
consists of nervous tissue stores and releases the 2 hypothalamic hormones produced in the Nucleus supraopticus and Nucleus paraventricularis: |
|
|
Nucleus supraopticus and Nucleus paraventricularis release what 2 hypothalamic hormones ??
|
the 2 hypothalamic hormones produced in the
Nucleus supraopticus and Nucleus paraventricularis: ADH and Oxytocin |
|
|
formed from Rathke’s pouch = glandular epithelium
produces and secretes hormones under hypothalamic control |
ANTERIOR pituitary = adenohypophysis
|
|
|
also called vasopressin
|
ADH
|
|
|
Glucocorticoids = ?
What do they control? Example(s) ? |
any hormone of adrenal cortex that affects carb,fat, and/or protein metabolism; chiefly cortisol and corticosterone
|
|
|
ADH and Oxytocin synthesized where?
|
hypothalmus
|
|
|
ADH and Oxytocin stored and RELEASED from where?
|
Most of it is stored in the posterior pituitary (neurohypophysis) to be released into the bloodstream
|
|
|
Does hypothalmus also regulate ANTERIOR pituitary = adenohypophysis?
|
Yes
|
|
|
Releasing Hormones (RH) and/or Inhibiting Hormones (IH) come from where? Target organ?
|
hormones produced in hypoth. go to ANTERIOR PITUITARY
RHs / IHs reach the Anterior Pituitary gland (via – hypophyseal portal system) |
|
|
RHs /IHs stimulate/inhibit the production and release of hormones from the ?
What are these type of hormones known as? (hint: movie '___ thunder' with stiller, j.black, and t.cruise) |
from the anterior pituitary gland into circulation = Tropic Hormones (mostly)
Tropic Hormones |
|
|
These tropic hormones in turn stimulate a peripheral endocrine gland to produce /
release its own hormones. |
These tropic hormones in turn stimulate a peripheral endocrine gland to produce /
release its own hormones. |
|
|
Where are 5 stimulating/releasing hormones that the hypoth. makes?
Hint: gd cn G Tt P |
Gnrh
Crh GHrh Trh Prh |
|
|
GnRH = ?
GHRH = ? |
GnRH = Gonadotropin R.H.
GHRH = Growth Hormone Rel. Hormone |
|
|
Gonadotropin Stimulates?
Which in term stumulates? |
Gonadotropin RH. stimulates A.P. to produce FSH and LH!!!
..gonads to make sex hormones |
|
|
Another name for growth hormone
|
Growth h. = Somatotropin
= Somatotropic Hormone = ST(H) |
|
|
Obviously GHRH stimulates AP to GH..but what peripheral gland does growth hormone stimulate?
|
Liver (and direct effects) to make Somatomedins,
which works on multiple tissues |
|
|
Corticotropin = Adreno-corticotropic hormone = ACTH
stimulates what organ? to make what? |
adrenal cortex to synthesize Glucocorticoids (aka cortisol)
|
|
|
Targets of ACTH?
|
many targets
|
|
|
What is TRH?
|
TRH = Thyrotropin Releasing Hormone
|
|
|
Where does Thyrotropin come from?
|
ant. pituitary
|
|
|
Where does TSH come from?
|
Ant.Pit.Gland
Thyroid stimulating hormone and thyrotropin are same thing |
|
|
TSH stimulates thyroid to stimulate what?
|
T3
T4 |
|
|
Where are some INHIBITING hormones that the HYPOTHALMUS. makes?
|
GHih (counteracts GHrh)
Pih (counteracts Prh) |
|
|
Prostaglandins made in the ?
What is target organ? |
Ant.Pituitary gland
direct effects (e.g. mammary gland) |
|
|
Which part (inner OR outer layer) makes the mineralcorticoids?
Which part (inner OR outer layer) makes the glucocorticoids? |
Zona glomerulosa (outer portion of AC) makes the mineralcorticoids!
Zona fasciculata (middle layer) makes the glucocorticoids! |
|
|
Low levels of calcium stimulates ?
|
Low levels of calcium stimulates release of PTH from chief cells of parathyroid gland. In addition to its effects on kidney and intestine, PTH also increases activity of osteoclasts to release calcium from bone, by stim. bone resorption.
|
|
|
What is primary mineralcorticoids?
|
Aldosterone (makes up 90% of mineralcorticoids) secreted from outer layer (Z.G.) of A.C.
AMC |
|
|
What is primary Glucocorticoids made by adr. cortex?
|
Cortisol (95% glucocorticoids secreted in mammals)
GC |
|
|
What 2 components are required to make thyroid hormone?
|
- amino acid tyrosine and iodine
|
|
|
How does Iodide (I-) gets into thyroid cell ?
Where does it go? in what form? |
Iodide uptake into thyroid cell via active pump btw. thyrocyte and blood vessel
Enters colloid space in follicle, Iodide oxid. by perixidase into iodine |
|
|
TGB? made where?
primary component of ____? |
thyoglobulin, made in follicular cells, is glycoprotein containing lots of tyrosine AA's
it is primary component of colloid |
|
|
difference between T1 and T2
where does all this happen? |
(iodine joins the TGB)
T1 contain only 1 iodine; T2 contains 2 iodines (still in colloid) |
|
|
what happens when form T3 or T4?
Which is find in higher conc.in plasma? |

T1&T2 are mere primary peptide chains - condense, fold over and form secondary structures, couple with eachother
(still in colloid) T4 makes of 93% in thyroid hormone in plasma? |
|
|
storage form of thyroid hormone
active form of thyroid hormone? what does it do? |
T4
T3 (active hormone; T4 is converted to T3 after enters target cell) |
|
|
Thyroid hormones are controlled via the ____?
|
Hypothalamic–Pituitary–Thyroid Axis
|
|
|
Hypothalamic TRH release is
- stimulated by _? - inhibited by _? |
Hypothalamic TRH release is
- stimulated by COLD - inhibited by stress (sympathetic n.s.) |
|
|
TRH stimulates anterior pituitary to
synthesize and secrete __ |
TSH
|
|
|
T3 or T4 is lipophilic?
transported by? |
yes
Binding of lipophylic T4 & T3 to plasma proteins (~99%), e.g. thyroxin-binding protein (& albumin); half-life of T4 in dogs: 12-14 hours half-life of T4 in man: ~6 days |
|
|
TSH stimulates thyroid gland to
synthesize and secrete thyroid hormones through: what mechanisms? |
- stimulation of iodide pump
- stimulation of iodination of tyrosine - stimulation of TGB proteolysis - stimulation of growth of thyroid cells (can lead to gland enlargement) |
|
|
Increased levels of ___ inhibit further release of
TSH -> by decreasing_____? |
Increased levels of circulating thyroid hormones inhibit further release of
TSH (by decreasing TRH receptor no.) |
|
|
Thyroid hormone affect on basal metabolism?
|
INCREASES metabolic rate:
nutrient utilization up ATP formation up oxygen consumption up HEAT production up |
|
|
True or False: High levels of thyr.hormone lower blood cholesterol.
|
FALSE
incr. lipolysis incr. beta oxidation incr. bile secretion -> lowers blood cholesterol -> geared towards supplying fat for energy |
|
|
Signs of thyroid hormone deficiency on skin?
|
HD: follicle atrophy ->
bilateral ALOPECIA myxedema (edema under skin) pigmentation |
|
|
name for non-neoplastic hyperplasia of thyroid gland
cause? |
goiter
iodine deficiency, or goitergenic substances like cabbage, etc. |
|
|
How would you explain animal which has all symptoms of hypothyroidism but has normal levels in plasma?
|
T4 is converted to T3 intracellularly, so could be a problem with intracellular mechanism
|
|
|
Other ways of hypothyroidism aside from testing T4 level?
|
1. inject TSH and see if T4 levels go up
2. inject thyroid hormones themselves and see if they are used |
|
|
True or False: These are symptoms of old cat with hyperthyroidism?
* hyperactivity, nervousness (10% of cats are apathetic) * body temperature down and skin temp. decreased * tachycardia; hypertension (retinal detachment) * diarrhea; polyuria / polydipsia (thirst) (b/o medullary washout) * skin changes (matted hair or alopecia) |
all true, except body temp. would NOT go down
* would see heat intolerance and INCREASED skin temp. Remember: metabolism / functions are accelerated in all organs! |
|
|
What causes activates trx of genes in virtually all tissues? And also stimulates following:
* synthesis of many enzymes, structural & transport proteins * general increase of metabolic activities in many tissues |
Thyroid hormone
|
|
|
Causes of hypothyroidism in dogs?
Typical hormone levels? |
mostly defects of the thyroid gland (autoimmune, lymphocytic infiltration or iodiopathic atrophy)
In dogs 95% cases caused by destruction of follicular cells due to autoimmune inflammation. Typical findings are incr. conc. of TSH and low T4, may also be aB against TGB thyroperox. in blood |
|
|
True or False: These are signs of hypothyroidism?
- skin alterations are most common: (alopecia) - myxedema = accumulation of hyaluronic acid in face and tail and folded skin (sometimes in nerves) - reproductive dysfunction intolerance; heat seeking |
True
Most importantly in hypothyroidism -> reduction of metabolic rate: lethargy; weight gain; exercise Remember: metabolism / functions slow down! |
|
|
Why does Cholesterol increase in hypothyroidism?
|
Cholesterol: Increase, because there is a lack of liver enzymes due to a decreased lipolysis. This means that the body is not digesting all of the fats in the diet so cholesterol levels would be elevated in blood. Fat filled feces would also be seen (according to Sjaastad p.217 constipation and passage in intestine reduced in hypoth.)
|
|
|
Why does Cholesterol decrease in hyperthyroidism?
|
Decreased cholest. due to a stimulation of lipolysis. Almost all fats in the body would be broken down
TH stim. production of bile juice. so micelle form. and fat abs. liver excretes of xs cholesterol w/bile as waste....so blood levels of chol. decline at high thyroid levels |
|
|
Why wud urea (in plasma) increase in Hyperthyroid cat?
|
high; more proteolysis -> more deamination of proteins, more conversion to urea
liver not functioning well? |
|
|
TSH level in hyperthyroid cat?
|
low, b/c T4 inhibits APG?
|
|
|
Dog got contraceptive treatment
(progesterone) for the past 2 years. Owners calls b/c heard that ***** might develop serious side effects causing her joints or bones to “grow funny”. Which condition have these owners heard about? . In this case, what causes this condition? |
Acromegaly
Progesterone-increased GH, can affect joints. Long standing progesterone levels cause GH to be released, if she is beyond sexual maturity, bone epiphysis are closed, so bones would growth in width, not length |
|
|
List / explain the clinical signs that can be associated with Acromegaly
disorder? |
Acromegaly or hypertrophy of extremities, frontal bone and mandible (membranous bones), increased interdental space (loss of teeth), increase muscle growth. Arthrosis & arthritis due to increase in CARTILAGE growth throwing off statics of joint.
Fluid retention due to a build up of proteins circulating in blood; increases osmoregularity. Secondary diabetes could develop due to progesterone’s increase in insulin resistance. This leads to hypertrophy of heart. |
|
|
progesterone is normally released when?
|
In pregnant *****, progesterone released during pregnancy; stimulates hypothalamus to produce GH-RH (growth hormone releasing hormone). Growth hormone makes pregn.***** slightly insulin res. (hyperglycemic) which ensures fetus gets adequate glucose, etc. Remember fetus counts as glucose dependent tissue!
|
|
|
Why are young, growing animals usually thin?
|
GH is lipolytic hormone
growing animal need protein for muscle/bone development; not fat |
|
|
Tropic effect of GH?
|
Tropic/indirect effects (inducing release of another hormone from target tissue) on liver to produce "somatomedin" aka Insulin-like Growth factors
These are IGF effects are typical protein ANABOLIC effects, mitotic rates, A.A. uptake, |
|
|
Direct effect of GH?
|
* stimulates hormone sensitive lipase, to force body to use fat as energy source
* in contrast spares glucose (excess can lead to insulin resistance - DM type 2!) for unknown reason, and spare protein |
|
|
Where are Somatotropins made?
|
Growth hormone (=Somatotropin) is an anterior pituitary (protein) hormone, produced by acidophils
|
|
|
Where are somatomedins made?
|
liver produces
somatomedins (or insulin-like growth factors = IGF) upon stim. from GH (somatotropin) |
|
|
True or False:
Somatotropin is hyperplastic & hypertrophic |
True
Somatotropin is growth hormone |
|
|
GROWTH HORMONE DEFICIENCY in young dog?
|
Dwarfism: inherited deficiency of GH and/or somatomedins
delay in physical maturity, keep puppy coat |
|
|
GROWTH HORMONE DEFICIENCY if occurs later in life ?
|
Early Aging
caused by: damage to pituitary cells (tumor,hemorrhage, radiation) OR if have liver disease -> no IGF also early aging |
|
|
Panhypopituitarism
|
tumor,hemorrhage, radiation usually don't only affect cells producing GH
none of hormones produced in ant. pituitary gland are made |
|
|
IS there any overlap in the function of mineralcorticoids and Gluco-
corticoids? |
Yes, Cross activity exists between some members of the mineralocorticoid and
glucocorticoid group |
|
|
True or False:
Each cortical zone is controlled by a separate mechanism ! (Zona glomerulosa, Zona fasciculata) |
True, but some cross reactivity
|
|
|
Corticotropin aka ?
|
Corticotropin or ACTH
|
|
|
Stress stimulates hypothalamus to release
|
Corticotropin Releasing Hormone
|
|
|
CRH stimulates release of ___ from ___?
ACTH stimulates release of ____ |
CRH stimulates release of CORTICOTROPIN = ACTH from anterior pituitary
Cortisol (and androgens) |
|
|
Main stimuli which lead to release of cortisol?
|
stress (epinephrine)
metabolic stress (hypoglycemia) pain, fever, inflammatory mediators - histamine, pyrogens |
|
|
How does cortisol help bring up blood glucose?
(remember hypoglyc. is one of stimuli for cortisol release) |
These are anabolic effects of glucocorticoids!
>need to provide fuel (glucose) to muscles/brain with energy 1. mostly gluconeogenesis (from amino acids) 2. strangely glycogenesis also because gluconeogenesis generates so much glucose in liver; some goes to storage* (*Prerequisite for glucagon’s glycogenolytic effects) |
|
|
Where do anabolic effects of glucocorticoids take effect?
|
gluconeogenesis in LIVER
|
|
|
Besides stress-related release, ACTH & Cortisol secretion also follow a circadian rhythm:
In dog cortisol highest in AM or PM? In cat cortisol highest in ? |
AM - highest activity level
PM - higher cortisol for cat |
|
|
Cortisol exerts negative feedback on ___ release
|
Cortisol exerts negative feedback on CRH (hypoth.) and ACTH (apg) release
FYI: CRH is CORTICOTROPIN (ACTH) releasing hormone |
|
|
Why might artificial or synthetic corticoids be used clinically?
|
fewer side effects (cross reactivity) than natural steroids
|
|
|
Glucocorticoids/CORTISOL promote Gluconeogenesis
(from amino acids); but where do AA's come from? |
* liver supplies some
* but mostly via proteolysis from peripheral tissues/muscle (not CNS & cardiac muscle) |
|
|
Name other catabolic affects of Glucocorticoids/CORTISOL:
Where does this occur? |
Extra-hepatic tissue
=========================1. Decreased Glucose uptake (in muscle and fat tissue = insulin resistant effect); muscle must rely on fat 2. Increased Proteolysis 3. Lipolysis Redistribution of fat (abdomen) |
|
|
Animal under high-standing Glucocorticoids (for long time), what happens to liver?
|
liver enlarges, becomes full of glycogen and fat
|
|
|
What happens to GH production in older animals?
Why significant? |
decreased GH production
prof. says mitotic tissues are not maintained -> tissue aging...whatever just go along with it |
|
|
glucocorticoids’ effects on GI?
|
HCl and appetite up; but mucus down
GC's are also anti-inflammatory unfortunately so PGE2 and all prostaglandins down, leads to ulcers |
|
|
glucocorticoids’ effects on blood glucose?
|
* hyperglycemia;
* insulin resistance -> steroid diabetes aka secondary diabetes fyi: called steroid diabetes b/c caused by GC's which are steroids |
|
|
glucocorticoids’ effects on CNS/ apg?
|
drop in synthesis of all these: ACTH,ADH,TSH,GH,
FSH/LH (leads to "Panhypopituitarism") |
|
|
2 types of neutriphils?
|
circulating pool
marginal pool |
|
|
glucocorticoids’ effects on LEUCOGRAM?
|
Lymphos & Eos numbers drop
Neutriphil (from marginal pool) increases in number in circulation platelet number increases RBC number increases |
|
|
Is the overall amount of neutriphils increasing in number?
|
No, neutrilphils from marginal pool avoid selectin-dependent capture due inhibition of binding by cortisol; consequently more neutriphils enter from marginal pool
|
|
|
Glucocorticoids prevent release of inflammatory mediators, e.g. from ?
|
from lysosomes, macrophages,
monocytes |
|
|
physiological controller of inflammatory processes
|
Glucocorticoids
|
|
|
Glucocorticoids reduce / prevent inflammations and resolve existing inflammations, probably by ?
|
deactivating inflammatory mediators
|
|
|
pre-pro-hormone of ACTH is called ?
|
Pro-Opio-MelanoCortin = POMC
|
|
|
When GC's enter cell, induce protein synthesis of ____, group of intracellular proteins which bind to trx. factors like nuclear factor kappa B to inhibit synthesis of interleukin
|
lipocortin, protein which inhibit enzymes (like phospholipase A2 and COX1/2) in cytoplasm which convert arachdonic acid to prostanglandins
|
|
|
NF kappa B is inhibited by ___?
|
cortisol receptor complex
|
|
|
True or False
Collagen synthesis increased by Glucocorticoids |
False; Collagen synthesis (part of wound healing) is inhibited by GC's
|
|
|
Which type of immune response is affected or inhibited to a greater extent: by glucocorticoids: cell mediated or humeral?
|
cell mediated immune response (T cells)
|
|
|
The cleaving of POMC gives rise to several active polypeptides:
|
1. α-MSH ( Melanocyte Stimulating Hormone)
2. β-ENDORPHIN (another stress factor to reduce incoming pain) 3. CLIP = Corticotropin-Like Intermediate Peptide 4. ACTH - controls release of Cortisol - is also crucial to maintain the viability of the entire adrenal cortex !! |
|
|
α-MSH does what?
overproduction of MSH? |
darkening of skin/mucosa
dark blotches on mucosa! |
|
|
CLIP function?
|
Not much - probably little physiological function; but pathological effects in horses similar to ACTH (aka Corticotropin)
|
|
|
ACTH another piece cleaved off from POMC is important why?
|
In addition to controls release of Cortisol,
ACTH required to maintain viability of entire adrenal cortex!!!! Disorders of ACTH production can affect all POMC compounds !! Also req. for production of mineralcorticoids? |
|
|
What might cause drop in ACTH production for long period of time?
What must been considered when treating with GC's? |
if animal treated for long period of time with GC's, tissues which make ACTH can shut down completely - entire adrenal cortex is in jeopardy
|
|
|
Hyperadrenocorticism aka?
Excess of what? |
Cushing’s Syndrome
excess of glucocorticoids |
|
|
Causes Cushing’s Syndrome aka Hyperadrenocorticism ?
|
1. Adenomas of adrenal glands -> excess cortisol (rare)
2. Adenomas of ant.pituitary 3. Iatrogenic = prolonged glucocorticoid therapy 4. HORSE: Pituitary Pars intermedia tumors produces P.O.M.C (and excess amounts of active metabolites) |
|
|
Which Adenomas of Cushing's is more common?
What is pathway here? What is it in excess here? |
Adenomas of ant.pituitary gland more common
Adenomas of ant.pituitary -> excess ACTH -> cortisol (common) |
|
|
Cushing’s Syndrome caused by prolonged GC treatment?
|
Latrogenic Cushing's
|
|
|
Adenomas of adrenal glands: what is pathway here?
|
Adenomas of adrenal glands -> excess cortisol (rare)
|
|
|
____ is thought to increases the ACTH efficiency 6x
|
CLIP
|
|
|
90% are ___?
|
90% are pituitary-dependent = PDH;
|
|
|
What animals is Cushings common in?
|
common in middle-aged to old dogs (boxer, poodle, terrier,dachshund), also in ponies (not horses), very rare in cats
|
|
|
PATHOPHYSIOLOGY of hyperadrenocorticism?
|
PROTEOLYSIS, LIPOLYSIS, (like in diabetes), redistribution of fat, Hepatomegaly (enlarged liver), DM3 in cats&horse (see section for symptoms!), PU/PD, ADH receptor gone, so can't reabs. H2O
|
|
|
HIRSUTISM
unusual because? |
slow hair shedding
in horses b/c in dog lose hair, color of fur gone |
|
|
These are all symptoms of final stages of what?
IMMUNODEPRESSION POLYPHAGIA PITUITARY GLAND DEPRESSION (TSH,FSH,LH, GH) -> Panhypopituitarism BEHAVIORAL CHANGES (docility in horses caused by endorphins) GASTRIC ULCERS HYPERPIGMENTATION (sometimes, if ACTH ) LAMINITIS / Horses |
Cushings - can get everything
e.g. DM3, hypothyroidism, reproductive failure (lack of LH, FSH), early aging (GH) |
|
|
TREATMENT of PDH
|
(Surgical removal of tumors; difficult so usually only in people)
> Preferred method via suppression of adrenocortex with mitotane (poison) therapy (=DDD insecticide) selectively suppress/destroy from of adrenal cortex * enz. inhibitors also available (safer) ~showed pics of dog whose fur grew back |
|
|
"Moon Face" =
|
Cushings Disease
|
|
|
How might Cushings lead to LAMINITIS / Horses ?
|
In Theory:
hypoglycemia ->Endothelins release -> vasoconstriction -> damage/hypoxia in digital joints -> LAMINITIS / Horses |
|
|
Main stimulus for ALDOSTERONE synthesis?
|
HYPOVOLEMIA & Low Blood Pressure -> Renin (released in kidney) -> converted to Angiotensin -> ALDOSTERONE
|
|
|
Other stimuli of leading to aldosterone secretion? (hyper___)
|
* Is also stimulated by HYPERKALEMIA
* moderately stimulated by hyponatremia (low Na+) |
|
|
WHICH tissues respond to aldersterone? (name 3; 2 are glands))
|
large intestine, salivary glands, sweat glands
|
|
|
If lack aldersterone, lose ___ and ____. Clinical sign owner might recognize? (basically seen with every endocrine dz)
Too much alderstorone, affects blood volume how? BP? Preload? |
loss of Na+ and water, PU/PD
blood volume increases, preload incr., BP up |
|
|
Most powerful method of reducing excess BP?
|
diuresis
|
|
|
Main cause of (Hyperaldosteronism)
|
* Causes?
1. any condition which cause polyuria 2. infarction of kidney (kidney thinks it's hypervolemic but isn't) 3. Main cause -> cyst formation in kidney (polycystic renal disease = PRD) grow over time, pressure up (a.) with renal dysfunction (b.) w/o RD |
|
|
renin is vasodilator?
|
no vasoconstrictor and become angiotensin blas
|
|
|
PRIMARY HYPOADRENOCORTICISM =
which hormones low? |
ADDISON’S DISEASE
= deficiency in adrenal cortex hormones -> Glucocorticoids (first) and Mineralocorticoids (later) are reduced |
|
|
Why concerned about hypertension?
|
endothelial lining, brain damage, etc
|
|
|
What happens to K+, Na+, H+ levels in blood in dog with Addison's? Why?
|
With Addison’s (Primary Hypoadrenocorticism) -> decreased mineralocorticoid e.g. Aldosterone -> get hyponatremia (no more “sodium saver”) and hyperkalemia and acidosis (more H+!)
Note: Glucocorticoids also decreased..obviously |
|
|
What animals is HYPOADRENOCORTICISM = ADDISON’S DISEASE more common in?
- specifically type involving immune mediated destruction of cortex |
(youngish fem. dogs)
- immune mediated destruction of cortex |
|
|
Other causes of HYPOADRENOCORTICISM = ADDISON’S DISEASE?
|
2. OVERTREATMENT for Cushings - mitotane induced adreno- cortical necrosis (mitotane therapy)
3. - long standing cortisol therapy -> depression of ACTH -> cortex atrophy > GLUCOCORTICOID Deficiency -> hypoglycemia, can't control inflammatory processes > MINERALOCORTICOID Deficiency: |
|
|
most powerful hormone controlling
plasma calcium and phosphate levels via: |
PTH is the most powerful hormone controlling
plasma calcium and phosphate levels via: |
|
|
MINERALOCORTICOID Deficiency:
leads to what electrolyte changes in plasma? |
(NO ALDERSTERONE)
Na+ & WATER loss, K & hydrogen retention -> Na/K plasma ratio less than 20 (normal 30-40) (so too much K+!!!!!) |
|
|
What stimulates release of PTH? (2 things)
|
1.Hypocalcemia:
2. Hyperphosphatemia: |
|
|
Net effect of PTH = plasma ___ increases, plasma ____ decreases
|
Plasma Calcium increases
Plasma Phosphate DECREASES |
|
|
PTH stimulates?
|
1. Stimulates bone mobilization (resorption) = increases plasma Ca and P
2. Stimulates renal calcium absorption = increases plasma Ca 3. Inhibits renal phosphate absorption = decreases plasma P 4. Stimulates activation of Vit. D = increases plasma Ca via GI absorption |
|
|
D-Hormone =
|
Calcitriol
|
|
|
Activation to D hormone occurs
in what 2 places? Requires? |
liver and kidney
requires PTH |
|
|
Calcitriol actions?
|
Actions:
1. increases intestinal and renal calcium and phosphate absorption 2. increases mobilization of bone (in high concentrations) |
|
|
Calcitonin stim. by?
|
- Stimulated by hypercalcemia
- Decreases activity and proliferation of osteoclasts |
|
|
Calcitonin favors __formation?
|
Favors bone formation
Decreases calcium and phosphate levels |
|
|
Calcitonin seems more important in what age group?
|
Calcitonin seems more important in young animals than adults and the
removal of thyroid gland / C cells has little effect on Ca balance |
|
|
Calcitonin secreting C-cells located where?
|
between thyroid follicle cells
|
|
|
Compensatory Hyperparathyroidism can be caused by ? (name 3)
|
1. Lack of dietary Vit D or lack of UV exposure -> reduced Ca absorption -> crooked legs
2. Dietary Ca/P imbalances 3. Renal Diseases with insufficient P excretion |
|
|
In all 3 cases of Compensatory Hyperparathyroidism, body releases ____ and mobilizes ____ from bone tissue.
If longterm, leads to ____ of bone. |
body releases PTH and mobilizes Ca from bone tissue
plasma Ca returns to low/normal if long-term, leads to softening of bone = DEMINERALIZATION = Compensatory Hyperparathyroidism |
|
|
Bran Disease or Big Head in Horses cause by ?
|
Dietary hyperparathyroidism
- on pasture grasses high in oxalates, which binds Ca - on high bran diet = excess P |
|
|
6 months old beagle / Rubberjaw caused by?
|
Renal Hyperparathyroidism
|
|
|
Milk fever = ?
Due to ? |
Parturient Paresis
Acute hypocalcemia within 72 hrs p.p. due to rapid loss of Ca via milk |
|
|
Why doesnt PTH release help?
|
PTH is released, but osteoclasts are reduced
in numbers or inactive due to dry period; takes time for them to reactivate -> Bone cannot respond fast enough -> acute hypocalcemia |
|
|
Signs of milk fever?
|
increased conductivity of Na channels -> excitability, tremors, seizures, tachycardia
- laccid paresis (may be caused / exacerbated by concomitant Mg increase) |
|
|
Prevention of milk fever?
|
feed diet low in Ca+ just before animal gives birth, to force reactivation of osteoclasts!
|
|
|
Messed up Na/K+ ratio is a sign of? (low K+)
|
HYPOADRENOCORTICISM = ADDISON’S DISEASE
|
|
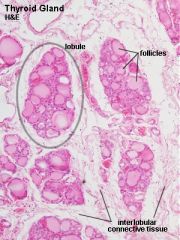
*skip -> What is contained in the lobule of the thyroid gland?
|
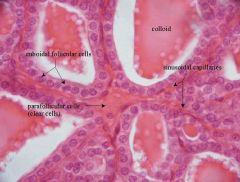
What is contained in the lobule of the thyroid gland?
- thyroid follicles, parafollicular cells, dense networks of sinusoidal capillaries. |