Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
78 Cards in this Set
- Front
- Back
|
What are the risk factors for coronary artery disease?
|
advanced age
genetic predisposition HTN smoking DM dyslipidemia chlamydia infection? |
|
|
what are some helpful lifestyle adjustment to prevent CHD?
|
stop smoking
exercise contol bp control blood lipids eat fruits and veggies vitamin E vitamin E+C |
|
|
What is the plaque like in stable angina?
|
it is stable but narrows the lumen
|
|
|
what is the plaque like in unstable angina?
|
it is ruptured --> platelet aggrefation, thrombus formation, unstopped vasoconstriction
|
|
|
what is the plaque like in variant angina?
|
there is no plaque
|
|
|
What is class I angina pectoris?
|
ordinary physical activity does not cause angina. angina occurs w. strenuous, rapid, or prolonged exertion
|
|
|
what is class II angina pectoris?
|
slight limitation of ordinary activity
occurs on walking or climbing stairs rapidly, walking uphill, walking or stairs after meals, emotional stress walking >2 blocks on level and climbing >1 flight of stairs at a normal pace |
|
|
what is class III angina pectoris?
|
marked limitations of ordinary physical activity
angina on walking 1-2 blocks on level/climbing 1 flight at normal pace |
|
|
what is class IV angina pectoris?
|
inability to carry on any physical activity w/o discomfort
symptoms may be present at rest |
|
|
how do you classify unstable angina?
|
severity
clinical circumstances intensity of treatment |
|
|
When classifying unstable angina by severity, what is class I?
|
new onset of severe angina or increased freq of attacks.
no rest pain |
|
|
When classifying unstable angina by severity, what is class II?
|
angina at rest, subacute. angina at rest w/in past month, but not w/in preceding 48h.
|
|
|
When classifying unstable angina by severity, what is class III?
|
angina at rest, acute, or during the preceding 48h
|
|
|
when classifying unstable angina by clinical circumstances, what is class A?
|
secondary UA, symptoms secondary to an identified condition reducing myocardial oxygen supply or increasing demand
|
|
|
when classifying unstable angina by clinical circumstances, what is class B?
|
primary UA
|
|
|
when classifying unstable angina by clinical circumstances, what is class C?
|
post infarction UA
|
|
|
when classifying unstable angina by intensity of treatment, what is class 1?
|
minimal or no therapy?
|
|
|
when classifying unstable angina by intensity of treatment, what is class 2?
|
therapy of chronic stable angina
|
|
|
when classifying unstable angina by intensity of treatment, what is class 3?
|
maximum therapy, including IV nitrates
|
|
|
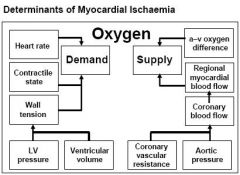
What are the determinants of myocardial ischemia
|
|
|
|
what drugs are used to treat angina?
|
nitrates
b-blockers ca channel blockers |
|
|
what combos of drugs are used to treat angina?
|
nitrate + B-blocker
|
|
|
What does an EKG look like during angina?
|
ST depression due to lack of O2
nitriates help keep O2 supply equal to demand |
|
|
What are the nitrates?
|
nitroglycerin
isosorbide dinitrate (ISdN) isosorbide mononitrate (ISMN) |
|
|
what do nitrates do?
|
relaxation of all smooth muscle including vascular smooth muscle
prompt relaxation of venous tone |
|
|
what are the effects of nitrates?
|
relaxation of venous tone --> decreased preload, enhancement of venous capacitance
decreases in arterolar resistance --> decreased afterload reduction in myocardial O2 demand improvement of redional distribution of coronary flow |
|
|
How long do nitrates take to act?
|
vasodilation w/in seconds
O2 correction w/in minutes |
|
|
How are nitrates administered?
|
Nitroglycercine: sublingual, buccal, transderma, IV
|
|
|
what are the adverse effects of nitrates?
|
headache, flushing
reflex tachycardia dizziness, weakness, cerebral ischemia tolerance |
|
|
when are nitrates used?
|
acute attacks of angina pectoris
anticipated attacks prolonged preventitve therapy (ISMN, ISDN) |
|
|
How do nitrates act?
|
they stimulate Guanylate cyclase
|
|
|
What is nitrate tolerance?
|
the nitrates become activated suing the glutathione system
tolerance results when this system is maxed out |
|
|
what factors prevent nitrate tolerance?
|
intermittent dosing
small doses infrequent doses provide nitrate free interval |
|
|
what factors induce nitrate tolerance?
|
continuous or prolonged nitrate exposure
sustained release large doses frequent doses |
|
|
what is a typical nitrate regimen?
|
NTG patch, remove for 10-12 h/d
ISMN - 2 daily doses 7 hrs apart |
|
|
What is the PO bioavailability of ISMN?
|
95%
|
|
|
what is the PO bioavailability of ISDN?
|
20%
|
|
|
Does ISDN or ISMN undergo first pass metabolism?
|
ISDN
|
|
|
what is the onset of effect, PO, for ISDN and ISMN?
|
10-30min
|
|
|
what is the half-life of ISDN?
|
30-40min
|
|
|
what is the half-life of ISMN?
|
3.5-6 h
|
|
|
what is sodium nitroprusside?
|
ferrocyanide compound
|
|
|
what does sodium nitroprusside do?
|
direct NO donator --> VERY effective, immediate acting vasodilator
|
|
|
what is the half-life of sodium nitroprusside?
|
< 3 min
|
|
|
why must sodium nitroprusside be protected from light?
|
it will get converted to cyanide then thiocyanide
|
|
|
when is sodium nitroprusside used?
|
in ICU and emergency setting
controlled hypotension during surgery special form of severest cardiac failure |
|
|
when should sodium nitroprusside use be cautioned?
|
when patient has borderline systolic bp
myocardial ischemia in absence of heart failure hepatic or renal insufficiency |
|
|
what are adverse effects of sodium nitroprusside?
|
severe nausea, vomiting, headache, CNS distrubances
|
|
|
what are the toxic effects of sodium nitroprusside?
|
cyanide intoxication
|
|
|
how long can sodium nitroprusside be used for?
|
some hours then must be discontinued
|
|
|
What is coronary steal?
|
1. branches of a coronary artery compete for blood flow
2. tissue distal to partially obstructed branch msy maintain sufficient perfusion by maximal dilation of vessels 3. distal to unobstructed vessel arterioles maintain some tone 4. in presence of vasodilator all vessels dilate - pressure everywhere drops 5. distal to obstructed vessel may not get enough perfusion |
|
|
Which calcium channel blockers can be used for angina?
|
verapamil
diltiazem nifedipine |
|
|
what is the PK of Ca channel blockers?
|
PO, IV
highly bound by serum proteins |
|
|
how are Ca channel blockers metabolized?
|
hepatic
|
|
|
how are ca channel blockers excreted?
|
renal
|
|
|
What is the MOA of ca channel blockers?
|
block L-type Ca channels
|
|
|
what effects do Ca channel blockers have?
|
cardiodepressant effects
arteriolar vasodilation |
|
|
what are the adverse effects of dihydropyridines (nifedipine)?
|
due to excessive vasodilation:
dizziness, headache, flushing, digital dysathesia, nausea, peripheral edema, constipation, reflex tachycardia |
|
|
what are the adverse effects of verapamil?
|
bradycardia - slow SA and AV conduction
|
|
|
what are the adverse effects of diltiazem?
|
bradycardia - slow SA and AV conduction
|
|
|
What can Verapamil be used for?
|
angina
HTN arrhythmia |
|
|
What can Diltiazem be used for?
|
angina
HTN arrhythmia |
|
|
what can Nifedipine and other dihydropyridines be used for?
|
angina
HTN |
|
|
What B-blockers can be used in angina pectoris?
|
propanol
atenolol metoprolol |
|
|
what do B blockers in angina do?
|
are effective in reducing the severity and frequency in exertional angina
somewhat effective in unstable angina |
|
|
what are the effects of B-blockers?
|
negative inotropic
negative chronotropic reduced systolic blood pressure during exercise |
|
|
what is the net effect of B-blockers?
|
reduced myocardial oxygen demand
|
|
|
What is the benefit of B-blockers post MI?
|
is cardioprotective - given early and taken for 2-3 yrs (B1 selective)
|
|
|
What conditions are B-blockers CI?
|
vasospastic angina - may worsen condition
|
|
|
What drug should be used in exertional angina?
|
B-blocker
|
|
|
what drug should be used in vasospastic angina?
|
Ca channel blocker
|
|
|
what drug should be used in angina w/ a COPD?
|
Ca channel blocker
|
|
|
what drug should be used in angina with a ventricular arrhythmia?
|
B-blocker
|
|
|
which drug should be used for angina in patients under 40?
|
B-blocker
|
|
|
which drug should be used for angina in patients over 65?
|
Ca channel blocker
|
|
|
What is the main effect of nitrates in angina?
|
decrease preload
|
|
|
what is the main effect of Ca channel blockers?
|
decrease afterload - may also have negative inotrpic effects
|
|
|
what is the main effect of B-blockers?
|
negative inotropy, may also decrease afterload
|