Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
96 Cards in this Set
- Front
- Back
|
Define "Bioequivalence"
|
2 drugs that have both the same
-bioavailability -rate of absorption |
|
|
2 drugs that are Bioequivalent will have these 3 things that are the same
|
1. Peak height concentrations (Cmax)
2. Peak times (Tmax) 3. Area under curves (AUC) |
|
|
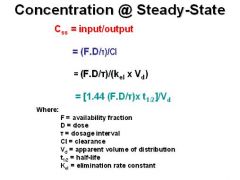
List the 3 equations for the Concentration at the Steady State
|
-
|
|
|
In Steady-state parameters, how many half-lives does it take to attain the Plateau state?
|
4-5
|
|
|
In steady-state parameters, is TIME to plateau dependent or independent of dose?
|
independent
|
|
|
In steady-state parameters, is the LEVEL of plateau proportional or unproportional to the dose?
|
proportional
|
|
|
In steady-state parameters, when are there no fluctuations?
|
with a continuous I.V. infusion
|
|
|
What blunts fluctuations in steady state parameters?
|
Slow absorption
|
|
|
What are fluctuations proportional to in steady-state parameters?
|
Dosage interval / half-life
|
|
|
What 3 things is Plateau concentration proportional to?
|
1. Dose / dose interval
2. half-life 3. F / Cl (availability fraction / clearance) |
|
|
What 2 things is Plateau concentration inversely related to?
|
1. Kel (elimination constant)
2. Vd (volume of distribution) *High Elimination rate constant = Low Plateau Conc. *High Vd = Low Plateau Conc. |
|
|
Definition: the maximum concentration attained after a given dose
|
Peak
|
|
|
Definition: the minimum concentration obtained prior to giving the next dose
|
Trough
|
|
|
What does Maintenance Dose depend on?
|
Clearance
|
|
|
What is another term for Dosing rate?
|
Maintenance dose
|
|
|
List 3 equations for calculating the Dosing Rate
|
1. (Css . Cl) / F
2. (Css . Kel . Vd) / F 3. (.693 . Css . Vd) / Half-life |
|
|
What does the Loading Dose depend on?
|
Volume of Distribution
|
|
|
What is the Equation for Loading dose?
|
(1.44 . Css . Vd) / F
*the higher the Vd = the higher the LD needs to be *the lower the Availability Fraction = the higher the LD needs to be |
|
|
How do you calculate the Rate of Infusion for IV infusion?
|
Ro = Css . Kel . Vd
*Rate of Infusion does determine the plasma level at the STEADY STATE *Double the Infusion Rate = Plasma Level of the drug at the Steady State is doubled |
|
|
How do you calculate the Loading Dose for IV infusion?
|
LD = Css . Vd
|
|
|
Why are loading doses given?
|
A loading dose may be desirable if the time required to attain steady state by the administration of drug at a constant rate (four elimination half-lives) is long relative to the temporal demands of the condition being treated
|
|
|
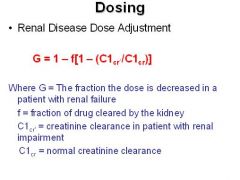
What is the equation for "Renal Disease Dose Adjustment"?
|
-
|
|
|
Definition: Study of the biochemical and physiological effects of drugs and mechanisms of actions
|
Pharmacodynamics
|
|
|
In dose-response relationships, what is the intensity of the response proportional to?
|
the number of receptors occupied or the concentration of drug-receptor complexes
|
|
|
What is INVERSELY related to the AFFINITY of drug for the receptor?
|
Dissociation constant (Kd)
- higher the affinity = lower the dissociation constant = less the drug will dissociate with the receptor |
|
|
What shapes do Log-dose response (LDR)curves typically have?
|
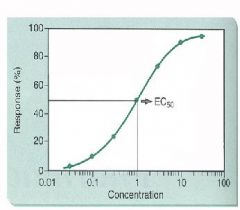
S-shaped or sigmoidal
|
|
|
Define "Graded Responses"
|
measures an increase in response in an individual as dose is increased
|
|
|
Define "All-or-None (Quantal)" responses
|
Number of individuals within group responding to a given dose; endpoint is set and an individual is either a responder or non-responder
|
|
|
For an All-or-None response, a normal histogram is usually this shape
|
Bell-shaped
|
|
|
Definition: in All-or-none responses, this is the dose to which 50% of subjects respond
|
Median effective dose (ED50)
|
|
|
What is the Therapeutic Index?
|
the ratio betwen the toxic dose and the therapeutic dose, used as a measure of the relative safety of the drug for a particular treatment
*Large ratio = High TI |
|
|
What is the equation for Therapeutic Index?
|
TI = LD50/ED50
= Lethal dose / Effective dose |
|
|
T or F: the higher the Therapeutic Index, the safer the drug
|
True
- TI = LD50/ED50 - means the LD and ED are far from eachother |
|
|
What is the equation for Margin of Safety?
|
LD1 / ED99 = dose to which it is lethal to 1% / dose to which it is 99% effective
*the higher the MS, the safer the drug |
|
|
A and B = full agonists
C = partial agonist |
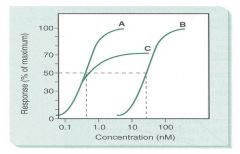
Define A, B, and C as partial or full agonists
|
|
|
Definition: the propensity of a drug to bind with a given receptor and is inversely related to Kd
|
Affinity
|
|
|
Which has a higher affinity, a drug with a Kd of 10^-7 M for a receptor or one with a Kd of 10^-6?
|
10^-7
|
|
|
Definition: comparative expression relating the dose required to produce a particular effect of given intensity relative to a standard reference
|
Potency
|
|
|
Which is more potent, a drug that exerts 50% of its maximal response at 10^-7 M or 10^-6 M?
|
10^-7
|
|
|
Definition: Measure of how well a drug produces a response
|
Efficacy
|
|
|
Synonym for Efficacy
|
Intrinsic value
*max efficacy is assigned 100% *Intrinsic value is assigned 1.0 |
|
|
Definition of an Agonist
|
stimulates a receptor, provoking a biological response
|
|
|
Definition of a Partial Agonist
|
provokes a maximal response somewhat less than a full agonist
|
|
|
Describe an "Inverse Agonist"
|
based on the concept that there is ongoing basal signal transduction occurring which is reduced by the inverse agonist
|
|
|
Define a Competitive Antagonist
|
Interaction of an Antagonist with a receptor does not result in stimulus for biological response, but will block the effect of agonist binding at same receptor site
|
|
|
How does one overcome the effects of Competitive Antagonist?
|
increase the dose of the agonist
|
|
|
As the concentration of the antagonist increases, does the Emax (max effect) change?
|
NO
|
|
|
What is the Efficacy (Intrinsic activity) of a Competitive Antagonist?
|
0
|
|
|
What will be the effect of a fixed dose of a Competitive Antagonist in a dose-response curve
|
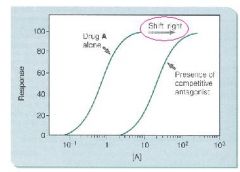
cause a parallel shift for an agonist to the right
|
|
|
With Noncompetitive Antagonists, can the effect be completely overcome by increasing the agonist concentration?
|
No
|
|
|
What is decreased in the presence of Noncompetitive Antagonists?
|
number of functional receptors
|
|
|
What happens to Emax as the concentration of noncompetitive antagonists increases?
|
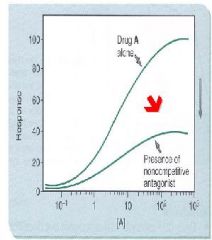
decreases because of fewer functional receptors available
|
|
|
What happens to the Dose-response curve with the presence of Noncompetitive Antagonists?
|
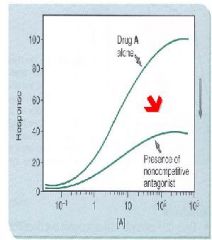
nonparallel, downward shift for the agonist to the right
|
|
|
Give 2 examples of when partial agonists act as inhibitors to a full agonist
|
1. Acebutolol is a partial agonist at the B1-adrenoreceptor
2. Selective Estrogen receptor Modulators - Tamoxifen - Clomifene - Raloxifene *As the partial agonist displaces the full agonist from the receptor, the response is reduced - the partial agonist is acting as an ANTAGONIST |
|
|
Define Potentiation
|
the effect of 2 drugs is greater than predicted from individual effects
|
|
|
Give 2 examples of Potentiation
|
1. Physostigmine (an AChEI) potentiates the response to ACh
2. Cocaine (uptake I blocker) potentiates the effects of NE and Epi |
|
|
What effect does Potentiation have on the Dose-response curve?
|
shifts the agonist to the left
|
|
|
Time it takes for steroids to cause a response
|
Hours
|
|
|
Time it takes for Insulin and Growth Factors to cause a response
|
Minutes
|
|
|
Time it takes for IL-2 and Cytokines to cause a response
|
Minutes
|
|
|
Time it takes for Nicotine to cause a response
|
Milliseconds
|
|
|
Time it takes for Epinephrine to cause a response
|
Seconds
|
|
|
Nicotinic/ACh receptors are this kind of receptor
|
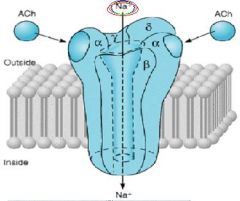
Ionotropic --> Sodium channel
|
|
|
GABA--Benzodiazepine receptors are this kind of receptor
|
Ionotropic -> Chloride channel
-Hyperpolarization - Inhibitory |
|
|
Glutamate/AMPA receptors are this kind of receptor
|
Sodium channel
-Depolarization -Excitatory |
|
|
Glutamate/NMDA receptors are this kind of receptor
|
Ionotropic = Calcium channel
-Depolarization -Toxicity -Excitotoxicity |
|
|
What do G proteins bind to and what do they couple with?
|
Bind to GTP
Couple with "7-TM receptors" or "Serpentine receptors" |
|
|
In G protein-coupled receptors, agonists promote the release of what?
|
GDP which allows for the attachment of GTP to nucleotide-binding site
|
|
|
In G-protein couple receptors, when GTP is bound what is the G protein capable of?
|
regulating an enzyme or ion channel
|
|
|
In G Protein-Coupled receptors, how is the signal terminated?
|
hydrolysis of GTP to GDP
*slow hydrolysis of GTP allows signal to persist long after the ligand has dissociated from the receptor |
|
|
What does Gs stimulate?
|
Adenylyl Cyclase
|
|
|
What does Gi do?
|
inhibits Adenylyl Cyclase and opens K+ channels
|
|
|
What does Gq do?
|
stimulates phospholipase C
|
|
|
What does Go do?
|
closes Ca+ channel
|
|
|
Explain the Adenylyl Cyclase system
|
Gs
- agonist binds receptor, couples the G-protein GTP binds causing alpha subunit to dissociate with Beta/gamma - alpha/GTP stimulate Adenylyl Cyclase which converts ATP to cAMP - cAMP activates PKA Gi = inhibits AC |
|
|
List 7 stimulatory agonists for the Adenylyl Cyclase system
|
1. ACTH
2. Beta-agonists (isoproterenol) 3. Glucagon 4. FSH 5. PGE2 6. Thyrotropin 7. Dopamine D1 agonists |
|
|
List 3 inhibitory agonists of the Adenylyl Cyclase system
|
1. Alpha-2 agonists = Clonidine
2. Muscarinic M2 agonists 3. Dopamine D2, D3, and D4 agonists **MAD 2's** |
|
|
Explain the model of desensitization
|
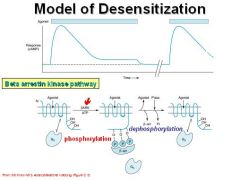
-Beta arrestin kinase phosphorylates the internal domain of the receptor when agonist binds
-When it's P'ed, beta arrestin binds and blocks coupling to Gs protein |
|
|
Explain the Polyphosphoinositide Signaling system
|
1. agonist binds to receptor and activates Gq protein
2. Gq activates Phospholipase C 3. PLC cleaves PIP2 into DAG and IP3 -DAG activates PKC -IP3 releases Ca+ -> Calmodulin-Ca+ |
|
|
List 5 receptors that activate the Polyphosphoinositide signaling system
|
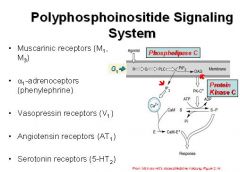
1. Muscarinic receptors M1 and M3
2. alpha-1 adrenoceptors 3. Vasopressin receptors (V1) 4. Angiotensin receptors (AT1) 5. Serotonin receptors (5-HT2) |
|
|
What do muscarinic receptors bind?
|
ACh and muscarine
|
|
|
What do Alpha-1 adrenoceptors bind?
|
Norepinephrine
Phenylephrine *PIP2 signaling system |
|
|
What do Growth Factors signal through?
|
Protein Tyrosine Kinase Signaling
|
|
|
Examples of agonists that signal through Tyrosine Kinase receptors
|
1. PDGF
2. Insulin 3. Epidermal Growth Factor **Insulin and Growth Factors |
|
|
Explain the Receptor Tyrosine Kinase signaling system
|
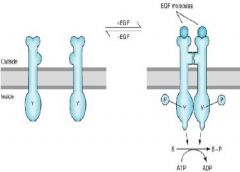
1. agonist binds
2. semi-distant receptors dimerize and autophosphorylate 3. Phosphorylation of downstream substrates |
|
|
What do Cytokines signal through?
|

Receptor Tyrosine Kinases linked to the JAK/STAT pathway -> dimerized STAT goes to nucleus
|
|
|
List 6 ligand responsive Transcrtiption Factors (Nuclear Receptors)
|
1. Glucocorticoids
2. Mineralcorticoids 3. Sex steroid hormones 4. Vitamin D 5. Thyroid hormone 6. Retinoid acid |
|
|
Explain the mechanism of Glucorticoid signaling
|
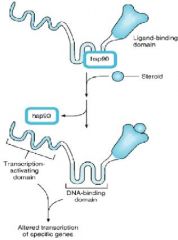
1. Steroid binds to Ligand-binding domain
2. Regulator protein is released 3. Tsc-activating domain and DNA-binding domain are exposed 4. Modification of gene expression |
|
|
Describe 2 ways in which Glucocorticoids are anti-inflammatory
|
1. induce synthesis of Lipocortin, an inhibitor of Phospholipase A2 (cleaves off Arachidonic acid)
2. decrease the up-regulation of COX-2 driven cytokines |
|
|
Where is Nitric Oxide formed?
|
Endothelial cells
|
|
|
What is NO's mode of action?
|
it diffuses through plasma membrane of Smooth Muscle cells activating Guanylyl Cyclase, converting GTP to cGMP
|
|
|
What does NO activate?
|
Guanylyl cyclase
|
|
|
What does cGMP activate?
|
Protein kinase G -> vasodilation
|
|
|
Where is iNOS found?
|
Professional killer cells
|
|
|
What is the substrate for NO?
|
Arginine
|
|
|
How can NO be toxic?
|
it reacts with Superoxide, forming the toxin Peroxynitrite
|