Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
48 Cards in this Set
- Front
- Back
|
describe the classical receptor theory (“occupancy theory”) of Clark.
|
“The intensity of drug effect (response) is proportional to the fraction of receptors occupied by the drug.
The law of mass action predicts that the rate of formation of Drug-Receptor complex (DR) is proportional to the concentration of Drug (D)and Receptor (R ) |
|
|
describe the concept of “spare receptors”
|
Modifications of the classical theory:
Spare receptors: Receptors are said to be “spare” for a given pharmacologic response when the maximal response can be elicited by an agonist at a concentration that does not result in occupancy of all available receptors. |
|
|
affinity efficacy
|
The propensity of a drug to bind with a receptor. k1/k2 is a measure of affinity; 1/KD (k dissociation)
|
|
|
intrinsic activity
|
The ability of a drug to initiate a response after binding to the receptors; --EFFICACY; K3
|
|
|
agonist
|
A drug capable of combining with receptors to initiate drug actions; it possesses affinity and intrinsic activity.
AFFINITY & INTRINSIC ACTIVITY E.G., MORPHINE; (K3=1) |
|
|
antagonist
|
Something opposing or resisting the action of another
AFFINITY NO INTRINSIC ACT (K3=0) e.g., NALOXONE |
|
|
partial agonist
|
Affinity with WEAK intrinsic activity (K3<1)- E.G., NALORPHINE;
|
|
|
ALLOSTERIC MODULATORS:
|
BINDS TO A DIFFERENT SITE FROM THE AGONIST: INCREASED OR DECREASED AGONIST REPONSE
Can be allosteric activator or antagonist e.g., bdz(BENZODIAZAPINE I.E. VALUM ,increased GABA EFFECT |
|
|
describe receptor-effector coupling
|
The binding of a drug with its receptor results in a conformational change (e.g. alteration of molecular configuration or charge distribution.) that triggers a chain of events leading to a pharmacological response.
|
|
|
describe different types of transmembrane signaling
|
1) INTRACELLULAR RECEPTORS for lipid-soluble agents (e.g. corticosteroids; sex hormones; thyroid hormone).
2)TRANSMEMBRANE RECEPTORS bound to a protein tyrosine kinase or other enzymes: (e.g. insulin, epidermal growth factors). 3) CYTOKINE RECEPTORS bound to a separate tyrosine kinase (JAK): Activation of STAT transcription molecules ( e.g. interferons, interleukins) 4) Receptors located on MEMBRANE ION CHANNELS: Ligand-gated ion channels—e.g. acetylcholine, GABA, excitatory AA. 5) Cell-surface receptors coupled to an effector enzyme by G proteins: Altered intracellular concentrations of “second messengers”. e.g. cyclic adenosine-3’, 5’-monophosphate (cAMP)Ca++/phosphoinositide |
|
|
describe the structure-activity relationship (SAR) of drugs
|
Affinity and intrinsic activity of a drug are intimately related to its chemical structure (“receptor selectivity”).
Relatively minor modification in the molecule may result in major changes in pharmacological properties; determined by stereospecificity, specific functional groups, etc. Ex: Adrenergic agonist/antagonists |
|
|
Receptor Type:Steroid
give Action: Location: Drug Example |
Action: Modulates gene expression in nucleus
Location: cytoplasm or nucleus Drug Example: Estrogen, corticosteroid, thyroid hormone |
|
|
Receptor Type: ion channel
give Action: Location: Drug Example |
Action: opens to permit ion diffusion
Location: cell membrane Drug Example: Acetycholine on nicotinic acetycholine receptor |
|
|
Receptor Type:Transmembrane Tyrosine Kinase
give Action: Location: Drug Example |
Action: phosphorylates cytoplasmic protiens
Location: cell membrane Drug Example: Insulin |
|
|
Receptor Type:JAK-STAT
give Action: Location: Drug Example |
Action: Activates a cytoplasmic protein kinase (STAT)
Location: Cell membrane & cytoplasm Drug Example: Cytokines |
|
|
Receptor Type:G-Protein Coupled
give Action: Location: Drug Example |
Action: Activates a membrane G protein that modulates an enzyme or channel
Location: Cell membrane Drug Example: Norepinephrine, Acetycholine (on a muscarinic receptor) |
|
|
in dose response curve
|
response is proportional to dose
|
|
|
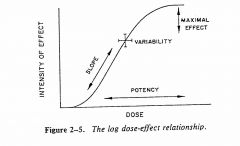
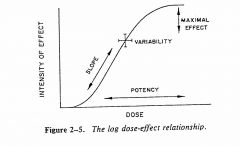
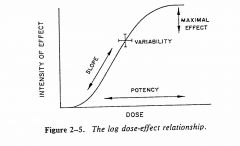
Graded dose-response curve is:
|
The log dose-effect relationship in 1 PATIENT
ALLOWS YOU TO COMPARE POTENCY OF DIFFERENT DRUGS by COMPARING EC50 |
|
|
Potency refers to the concentration (EC50) or dose (ED50) of a drug required to produce 50% of its maximal effect; the lower the dose required to produce a given effect, the higher the potency.
|
Signicance of potency in graded dose-response curve
|
|
|
The maximal effect
Efficacy of a drug may be limited by its propensity to produce a toxic effect. |
Signicance of maximal efficacy in graded dose-response curve
|
|
|
Slope reflects the mode of action of a drug AKA-- describes drug binding to its receptors.
AKA-- its COUPLING/SIGNAL MECHANISM 2) Slope has some relationships to margin of safety of drug. i.e., STEEP SLOPES =DRUG IS MORE DANGEROUS, E.G, PHENOBARB HAS STEEPER SLOPE THAN VALIUM |
Signicance of slope in graded dose-response curve
|
|
|
differentiate between characteristics of a competitive antagonist (“surmountable”) and an irreversible antagonist (“insurmountable”)
|
0
|
|
|
Competitive Antagonism: “Surmountable”
|
RIGHT SHIFT
DECREASE POTENCY SAME MAX |
|
|
Irreversible Antagonism: “Insurmountable”“noncompetitive”
|
LOW MAX
IRREVERSABLE SAME ED50 |
|
|
predict the effect of a competitive antagonist on the dose-response curve of an agonist
|
RIGHT SHIFT
DECREASE POTENCY SAME MAX |
|
|
predict the effect of an irreversible antagonist on the dose-response curve of an agonist.
|
LOW MAX
IRREVERSABLE SAME ED50 |
|
|
distinguish between pharmacological antagonism, physiological antagonism and chemical antagonism.
|
--
|
|
|
pharmacological antagonism
|
when two drugs compete for the same receptor site
|
|
|
Physiological antagonism (FUNCTIONAL ANTAGONISM)
|
when two drugs act on different receptors to cause opposite effects on the same physiologic function
E.G., EPI IN ANAPHALAXIS (BRONCHIODIALATION VS BRONCHIOONSTRICTION) |
|
|
Chemical antagonism
|
when one drug antagonizes the actions of a second drug by binding to and inactivating the second drug.
E.G., EDTA VS LEAD, HG ANTACIDES VS TETRACYCLINES |
|
|
define variance, quantal dose-response curve, median effective dose (ED50),median lethal dose (LD50), and therapeutic index (TI).
|
---
|
|
|
Variance:
|
Differences in the magnitude of response among individuals given the same dose of drug.
|
|
|
Quantal dose-effect curve:
|
Select an end point or a specified effect and determine the number of individuals at each dose who show the specified effect (“all-or-none”). Plot as a cumulative frequency distribution.
|
|
|
median effective dose (ED50)
|
The dose of a drug required to produce a specified intensity of effect in 50% of individuals.
|
|
|
Median lethal dose (LD50):
|
The dose of a drug required to produce death in 50% of individuals.
|
|
|
Therapeutic index
|
LD50/ED50 or TD50/ED50
(50% lethal dose over 50% median effective dose OR 50% toxic dose over 50% median effective dose) large TI means drug is safer (AKA more desireable) small TI less safe (less desireable) |
|
|
define supersensitivity, tolerance, tachyphylaxis, desensitization, “downregulation” and “up regulation”.
|
--
|
|
|
supersensitivity
|
An antagonist may increase the number of receptors in a critical cell or tissue by preventing down-regulation caused by an endogenous agonist. When the antagonist is abruptly withdrawn, one can get an exaggerated response or supersensitivity to an endogenous agonist.--E.G., PROPRANOLOL
Supersensitivity may result from “up-regulation” or synthesis of additional receptors. |
|
|
tolerance
|
Exposure to an agonist ligand may result in “down-regulation”---an actual decrease in number of receptors. This process may contribute to “pharmacodynamic tolerance”. --E.G., MORPHINE
|
|
|
Hyperreactive
|
If a drug produces its usual effect at a very LOW dosage
|
|
|
Hyporeactive:
|
If unusually LARGE doses of the drug are required to produce the effect.
|
|
|
Tolerance:
|
Hyporeactivity that develops as a result of continued EXPOSURE to the drug.
|
|
|
Tachyphylaxis
|
Hyporeactivity that develops RAPIDLY after administration of only a few doses of a drug-- “ ACUTE TOLERANCE”
|
|
|
desensitization
|
refers to a reversible and decrease of responsiveness in the presence of the agonist: Multiple mechanisms include phosphorylation of the receptor, destruction of the receptor,or its relocation within the cell.
|
|
|
“downregulation”
|
an actual decrease in number of receptors.
|
|
|
“up-regulation”
|
synthesis of additional receptors.
|
|
|
selectivity
|
The relationship between the doses of a drug required to produce undesired and desired effects
The therapeutic index (TI) of a drug reflects its selectivity. A LARGE TI is desirable |
|
|
risk-to benefit ratio
|
1)ALL drugs carry some degree of risk, esp. when given in high enough dose.
2) Some drugs carry a very HIGH degree of risk: Some drugs have very steep dose-response curves or a low therapeutic index. (e.g., Warfarin) 3) Potential benefits must be considered when using drugs, esp. drugs with high toxicity. |