![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
Pemoline- side effect? |
rare hepato-toxicity |
|
|
describe the steps in fine motor development from 4 m to 16 m |
4 m: reaches for an object, grab it. bring to mouth 5 -6 m: transfer object from side to side 7- 8 m: bangs object on the table 9-10 m: pincer grasp (first 3 fingers, then 2 ) 11 -12m: take out pegs from box, start putting in. 12 -14m: put pegs in hole, scrible 14- 16m: put box one on top of the other to built a tower |
|
|
List 8 parameters suggesting inherited metabolic epilepsy |
1. consanguinity 2. onset in the neonatal period 3. poor feeding 4. lactic acidosis 5. myoclonic sz. 6. apneic spells 7. EEG: burst suppression, generalized spike-wave 8. poor response to traditional AED |
|
|
Biomarkers for Pyridoxine dependent epi |
elevated levels of alpha-AASA & pipecolic acid eleveated levels of pyridoxal 5 phosp. in CSF mutation analysis of ALDHTA1 |
|
|
Other etiologies responsive to pyridoxine? |
1. infantile spasm 2. KCNQ2 mutations epi. |
|
|
Which of the following drugs does not cause withdrawal effect after prolonged use? |
Methyl phenidate Dextroemphetamine propanolol venlafaxine |
|
|
what is the current recommendations of the AAP and the american heart association regarding cardiac screening /ECG prior to the use of stimulants |
AAP: consider cardiologic assessment according to personal / family hx. AHA: ECG prior to tx. to measure QT distance |
|
|
List the branches, leaving the facial nerve from the acoustic canal to the stylo-mastoid process |
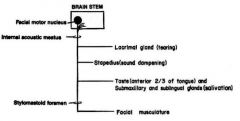
1. Tear (lacrimal) 2. Hear (stapedius) 3. Taste (2/3 anterior tounge) |
|
|
Glut-1 def. characteristics |
1. Glu in CSF <40 or Glu ration <0.4 CSF:serum 2. 90% of pt. develop epi, most common early onset abscence 3. EEG shows focal or generalized attenuation but may be normal 4. MRI- cerebelar atrophy 5. microcephaly, ataxia, dev. delay |
|
|
Glut-1 def. therapy |
1. rapid response to ketogenic diet 2. trials to use anaplerotic agent: Trihepanotin 3. Avoid drugs that inhibit the transporter: Phenobarb, diazepam, theophylline and caffeine, alcohol, valporate. |
|
|
Optokinetic drum can indicate what? |
Inability to fixate due to visual impairment or difficulties with fixation (strabismus) |
|
|
which CN close the eyes? which one opens? Ptosis due to horner - signs? |
CN 7 close the eye, CN3- open. Horner syn.: ptosis, miosis - better appreciated in darkness, an-hydrosis. If the injury is above superior sympathetic ganglion (foramen magnum level) no anhydrosis will be present |
|
|
which CN leaves the brain stem to the contra-lateral side? What's distinguish CN7 in his trail in the pons? |
1. CN4 (punished by reduced responsibilities..) 2. CN 7 tract leaves the nucleus direction the 4th ventricle, only after a round-about leaves the pons anterior-lateral, same as other CN |
|
|
Which CN are pure motor? |
CN3 - Oculomotor CN4 - Trochlear CN6 - Abducense CN11 - accessory (social climber, goes up from C1) CN12 - Hypoglossal: the engine under the tongue |
|
|
What stimulant drug is used for other indication, not just ADHD? |
Modafinil- for narcolepsy |
|
|
Gender differences in ornitine transcarbamylase def.? |
Males present in the neonatal period with encephalopathy and sz. - die young. Females (heterozygoes) typically present during childhood with less severe presentation |
|
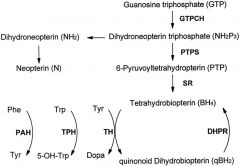
what pathway described in the graph? Which enzymes causes neurotransmitters realted encephalopathy? Which defects can be treated? |
The tetra-hydro biopterin pathway, an essential component in the production of dopamine, NE, serotonin. The most common defect: 6 pyruvoyl-BH4 synthetase The second: DHPR. For DHPR def. treat with folinic acid (leukoverin) For 6-P-BH4: L-dopa, 5-hyroxy triptophan |
|
|
What is the first step in the diagnosis of neonatal/early onset epileptic encephalopathy? |
MRI : directs to one of 3 groups: 1. Normal or non-specific findings 2. malformations of cortical development 3. vascular or traumatic etiology |
|
|
Early onset epileptic encephalopathy when MRI is non-contributing, what lab. study will you order? |
1. Biochemical studies: basic metabolic+ creatine/GAA, pipecolic acid, alpha aminoadipic semialdehyde=AASA, copper/ceruloplasmine, homocystein, biotinidase. 2. CSF (4 hour post prandial): Glu, AA, lactate, pyruvate, neurotransmitters, P5P, 5-MTHFR |
|
|
In which cases your work up might change? |
In cases with malformations, systemic findings or clinical features suggesting of a specific etiology. |
|
|
What are the therapeutic interventions in children with creatine synthesis disorders? |
Creatine and ornithine supplement. Restrict arginine from the diet |
|
|
First line tx. in Othahara EIEE ? |
corticosteroids and keppra |
|
|
First line in ESES? |
corticosteroids and Clobazam |
|
|
Epileptic encephalopathy - definition? |
The epileptiform abnormalities are believed to contribute to progressive disturbances in cerebral function. (ILAE) |
|
|
The most common sz. type in EIEE (Othahara)? typical EEG? |
Tonic sz. Burst suppression while awake or sleep |
|
|
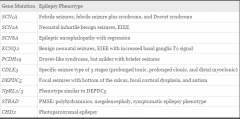
Genetic mutations in EIEE? |
EIEE1=ARX (aristaless related homeobox) Xp22 EIEE2=CLDK5, Xp22 EIEE3=SLC25A22 EIEE4=STXBP1 |
|
|
Early myoclonic epilepsy - what's the main difference from EIEE? |
1. Sz. semiology: in EIEE=tonic and EME=erratic myoclonus 2. EEG: inEIEE - burst suppression while awake and sleep. EME - burst suppression only in deep sleep 3. Causes in EME are mostly metabolic (NKH, Zwellger, MoCO def., organic acidemia) and genetic in EIEE |
|
|
Epilepsy of infancy with migrating focal sz. Describe clinical signs |
sz. activity migrates from one place to another within the same episode Sz. refractory to tx. genetic - gain of function mutation in KCNT1 gene |
|
|
Current knowledge re. west syn. etiology: Prevalence: |
40% stractural/ metabolic/ neurocutaneous Genetic - 30%? unknown 0.25-0.4:1000 |
|
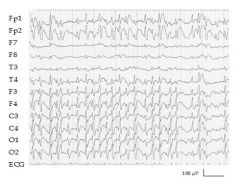
4 yO boy presented with deterioration in his behaviour and language skills during the past 2 months. EEG recording during sleep showing epiletiform activity in more then 85% of non REM sleep |
CSWS is characterized by an impairment of neuropsychological abilities, frequently associated with behavioral disorders (reduced attention span, hyperkinesis, aggressiveness and difficulty interacting with the environment), hyperactivity, learning disabilities and, in some instances, psychotic regressions. These mental and behavioral disorders can persist even after CSWS has ceased. Their severity and persistence seem to be correlated with the duration and severity of ESES |
|
|
Genetic mutations related to ESES? |
GRIN2A MeCP2 KCNA2 n |
|
diagnosis? major sz. types? |
LGS tonic-axial, atonic, abscence 1-4% of epilepsies under 5 y 70% of cases are symptomatic. From those with no metabolic/ stractural/ post TBI - few pt. were found to have GABRB3 mutation |
|
|
which mutations involved in prolonged tonic or prolonged clonic sz. ? CDLK5 |
|
|
Criteria for ESES |
new onset sz., may be all types but not tonic sz. (in 50% of children 1st sz. is nocturnal and unilateral) deterioration in behaviour EEG- more then 85% of recording during non REM sleep is slow wave-spikes ages: 2m- 12 y, mostly 4-6 y Previous hx. can be positive for ID, neurologic deficits but not epileptic encephalopathy. |
|
|
What a child is normally not doing by 2 years of age? |
1. built a tower 6 blocks 2. uses "I" and "you" in a short sentance 3. draw a circle when asked for 4. constuct a train of 4 cubes |
|
|
A pt. with a tumor experience loss of pain and temp. sensation in the left leg and spastic paralysis of the rt. leg. Where is the tumor? |
Pressing the Rt. lateral side of the spinal cord, compressing the cortico-spinal tract and the rt. spino-thalamic tract |
|
|
Loss of pain-temp on the lt, side and paralysis and loss of sterogenesis and proprioception in the rt. side- all belw neck. Where is the lesion? |
Hemisection of the rt. side - Brown Sequard |
|
|
What sensory tracts will be preserved following stroke of ant. spinal artery? |
Proprioception- stereognosia and light touch - nucleus gracilis and cuneata |
|
|
Bilateral paralysis with muscle atrophy & bilateral loss of pain and temp. sensation below C8-T1: where is the lesion? |
syringomyelia affecting the decussation of the pain and temp. tracts and pressing the ant. horn cells, causing LMN paralysis |
|
|
Total sensory loss of s given drematome - where is the lesion? |
The entrance of the sensory fibers (affarent) to the spinal cord ( most unlikely that any solicits damage will occur. |
|
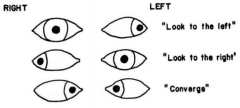
describe? where is the lesion? |
Rt. Internuclear ophtalmoplegia medial leminscus fasciculus |
|
|
pt. with difficulties in vertical gaze and no convergence. where the lesion is placed? common causes? |
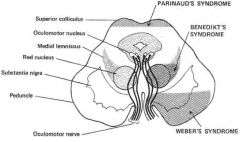
Parinaud syn. tumors of the pineal gland that compress the midbrain, Dilatation of the 3rd ventricle MS/ADEM |
|
|
Genetics of Friedrich's ataxia |
AR. The gene Fraxatin located on chromosome 9. The defect is attributed to an abnormally expanded GAA repeat in intron 1 of FXN. The longer the repeats area, the earlier symptoms are noticed. |
|
|
13 yO girl presented with ataxia, dysarthria and distal limbs weakness. On exam.- loss of deep tendon reflexes but positive babinsky sign. Diagnosis? clinical criteria? |
Friedrich's ataxia * progressive ataxia * dysarthria * muscle weakness * loss of proprioception+position sensation * a or hypo reflexia * onset prior the age 25 |
|
|
Congenital myasthenia |
* starts in infancy: 0-2 y * feeding difficulties * respiratory dysfunction * ophthalmoparesis * ptosis * hypotonia and limb fatigability * slow development |
|
|
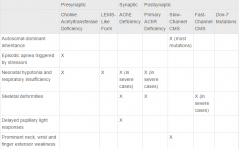
How to distinguish between the different mutations? |
|
|
|
What are the presynaptic types? |
1. Paucity of synaptic vesicles and decreased quantal release 2. Congenital myasthenic syndromes with episodic apnea (choline acetyltransferase deficiency) 3. Lambert–Eaton syndrome-like form |
|
|
Choline acetyl transferase defficiency (ChaT) - clinical signs? |
present at birth/ present in childhood Present @ birth: hypotonia, poor feeding, respiratory difficulties. Present @ childhood: apneic spell while sick/ emotional stress/ vomiting episode. May present ptosis and hypotonia as babies, but no eye movements abnormalities. |
|
|
Antibodies to AchR, anti MuSk, anti AchE can be found in which of the congenital MG? |
None - it's not an autoimmune disorder |
|
|
What is the most common type of cong MG in Israel? |
Rapsyn is a postsynaptic peripheral membrane protein that anchors the nicotinic acetylcholine receptor to the motor endplate. CMS patients of Iraqi and Persian Jewish origin, carry a common founder mutation in the E box of the RAPSN promoter region causing a spectrum of Achtylcholine receptor defect. |
|
|
Clinical worsening with Acetylcholine inhibitors is found in: |
* synaptic defect: Acetylcholine deficiency * post synaptic slow channel unit in the acetylcholine receptor * post synaptic Dok-7 mutation in the acetylcholine receptorxc |
|
|
The cold caloric test: clinical purpose? physiologic background results? |
inject cold water to the ear and watch the eye's response. Serves the clinician to differentiate levels of consciousness. The first and slow phase of the nystagmus is mediated by the brain stem and it's towards the ear where the water were injected. The second and fast response is cortically mediated, away from the cold water. When there is no response- means no brainstem reflex. |
|
|
13 y O girl complains of parasthesia sensations in rt. arm and optic neuritis. 4 months earlier she was admitted to another hospital due to bilateral lower limbs weakness and urinary incontinence that resolved almost completely. DD possible diagnosis? |
D.D. 1. Transverse myelitis - relapsing 2. Relapsing ADEM 3. MS No encephalopathy -can not be ADEM, for NMO - time difference between both episodes can be months till years. |
|
|
list 3 leukodystrophies for which BMT is offered in early stages of disease |
Krabbe Adrenoleukodystrophy Metachromatic Leukodystrophy |