Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
22 Cards in this Set
- Front
- Back
|
In a pedigree, what are the standard symbols for male, female, unknown sex, pregnancy, adopted, deceased, affected, X-linked carrier, consanguineous union, sibship, infertility, divorced/separated, miscarriage (unaffected), miscarriage (affected), termination of pregnancy (unaffected and affected), dizygotic twins, monozygotic twins, proband, no children?
|
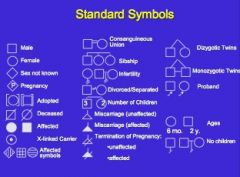
Here
|
|
|
What is the definition of genotype? Phenotype? Penetrance?
|
Genotype: Genetic composition at a given location (allele) in the genome.
Phenotype: Observable expression of a genotype (morphological, clinical, biochemical) Penetrance: Probability that an individual carrying a specific genotype will express the phenotype. May be complete (100%, like sickle cell) or incomplete (<100%) |
|
|
What are some reasons for reduced penetrance:
|
1.) Developmental Processes -- Other factors (like environmental, other genes required, exposure, sequence of events) beyond genetic change is required to cause phenotype (Ex: holoprosencephaly)
2.) Time related – Findings have an onset in older age (ex: Huntington disease, colon cancer) 3.) Sex limited – ex: male pattern baldness |
|
|
What is expressivity? Why does it vary?
|
Expressivity is the degree to which the phenotype is apparent (i.e. SEVERITY of the disease) Thus – even if the penetrance is 100%, the severity of the phenotype is not the same in every individual. (Ex: Down’s syndrome → may or may not have heart disease, varying levels of mental retardation per individual.)
Reasons for variance: “Intrafamilial variability” → modifier genes, environment, stochastic (non-deterministic – “a state does not determine the next state”) “Interfamilial variability” → all of the above, plus allelic and locus heterogeneity → the mutation itself falls on a spectrum. May be milder in some cases, while other mutations lead to complete loss of function. |
|
|
What is Allelic Heterogeneity? What is locus heterogeneity? Give examples of each
|
Allelic: Different mutations at the same locus. (leading to similar pattern of traits, though possibly with different severities)
**(EX: Hbb S (Glu6Val) = classic sickle cell disease; Hbb C (Glu6Lys) = less severe sickle cell disease) Locus: Mutations at different loci leading to the same (or similar) phenotype. **(EX: BRCA1 & BRCA2 genes → different alleles, same result) |
|
|
What is phenotypic heterogeneity? Give an example.
|
Mutations in one gene can cause different phenotypes.
Ex: Different mutations in same gene for RET (Receptory Tyrosine Kinase) can cause both 1.) Hirschsprung disease (no parasympathetic innervation to distal colon) or 2.) Multiple Endocrine Neoplasia 2 (Endocrine tumors). |
|
|
What is pleiotropy? Give an example.
|
A single abnormal gene produces diverse phenotypic effects (especially in multiple organ systems). (SYNDROMIC)
EX: Marfan syndrome affects the eye, bone, heart, etc. Also, Down Syndrome. |
|
|
What are the 5 modes of inheritance?
|
Autosomal recessive
Autosomal dominant X linked Mitochondrial inheritance Multifactorial |
|
|
What are some characteristics associated with an autosomal dominant inheritance?
|
*Affected person usually has at least one affected parent.
*Affects both sexes equally (unless it’s a sex-linked phenotype like baldness) *Transmitted by either sex *Child of an affected parent has a 50% risk of inheriting the disease. |
|
|
What are examples of exceptions to the rules of autosomal dominant transmission? (i.e. reasons for not seeing same phenotype in multiple generations)
|
*It’s a new mutation (ex: lethal autosomal dominant)
*It has low penetrance *Expressivity is variable *Germline mosaicism (in this case, you may see affected children with unaffected parents) |
|
|
Lethal autosomal dominant conditions are usually _______ mutations.
|
De novo (NEW!!!!) → so you won’t see population differences in these.
|
|
|
In X-linked disorders, there cannot be _____ to ______ transmission. Why?
|
Male-to-male
Because fathers always contribute the Y chromosome to their sons. |
|
|
What are the characteristics of autosomal recessive traits?
|
*Affected individuals usually born to unaffected parents.
*Affects either sex. *Observed more frequently with consanguinity *25% risk of having an affected child if both parents are carriers “Out of the blue” mutations are often autosomal recessive. 1:2:1 ratio (normal : carrier : affected) |
|
|
Almost all inborn errors of metabolism are _______ inherited. Why?
|
Autosomally recessively.
Having 50% of the enzymatic activity is usually OK to get by (there’s usually excess of enzymes) |
|
|
What is X linked recessive. Which sex is more affected and why?
|
Carried on sex chromosome (instead of autosome).
Men are more affected b/c they only have one X chromosome, so they’re “flying more unprotected” |
|
|
What types of disorders are observed more frequently with consanguinity?
|
Recessive
|
|
|
What are the characteristics of X-linked Recessive Inheritance?
|
*Usually affects males
*Affected males usually born to unaffected parents *May be other affected male relatives on the MATERNAL side of the family *No male-to-male transmission |
|
|
When might a female show signs of an X-linked recessive disorder?
|
1.) Unfavorable lyonization. (Lyonization is the silencing of one of the female X chromosomes → a.k.a. “X-inactivation”) This is so that females have the same amount of X gene products as males. The process is random, so if by CHANCE the female is a carrier for an X-linked disorder and the bulk of the good X genes get turned off, a female could show signs of the disorder.
2.) Homozygous for the mutation → both mother and father transmit a mutated X. Especially true for common traits (ex: red-green color blindness) 3.) Uniparental Isodisomy → inherit both Xs from your mother. (Rare) 4.) Chromosomal abnormalities → i.e. 45X or 46 XY females |
|
|
What is lyonization? What is uniparental isodisomy?
|
Lyonization → X-inactivation. Happens in females to silence X genes to have the same amount of gene product as males.
Uniparental isodisomy → females inherit BOTH X’s from mother. |
|
|
What are some differences between X linked dominant and X linked recessive? What would you see on a pedigree for a LETHAL X-linked dominant condition? How does X linked dominant differ from autosomal dominant?
|
Heterozygous females CAN be affected in XLD. Males are often more affected, but not always. Some XLD are MALE LETHAL → so on the pedigree you’ll see no affected males, a female to male progeny ratio of 2:1 overall (i.e. there is a paucity of males), and an increased incidence of miscarriages and infertility.
Difference between X linked dominant and autosomal dominant: Still no male-to-male transmission in X linked dominant, but there is in autosomal dominant. |
|
|
What is incontinentia pigmenti? What kind of inheritance has taken place? Why do the children affected look the way they do?
|
This is a lethal X-linked dominant disorder. Since this is lethal in males, you’ll only ever see heterozygous females with a mosaic patern = “Zebra skin.” The females who have this have stripes of hyperpigmented skin – the stripes are a result of the X-inactivation process (think calico cat).
|
|
|
What are the characteristics of mitochondrial inheritance? What can be done as a preventative measure?
|
*Inherited ONLY from the MATERNAL line.
*Both Males and Females may be affected *Huge VARIABILITY IN EXPRESSION: Phenotype dependent on % abnormal mitochondria per cell (heteroplasmy) & energy requirement of the cell *Can affect any organ (CNS, heart, GI, any combination) Embryos can be synthesized with genetic material from two mothers. Currently being done in the U.K. “Pronuclear Transfer” → get rid of bad mitochondria from an egg and use good mitochondria from an egg donor. |