Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
69 Cards in this Set
- Front
- Back
|
What are the 3 layers of normal Skin?
|
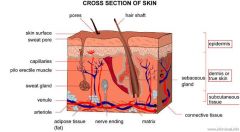
Epidermis
Dermis Subcutaneous tissue |
|
|
List the layer of Epidermis from inside-out & define each
|
Stratum Basale = proliferative basal layer of columnar-like cells; actively dividind stem cells along the BM
Stratum Spinosum = contains prominent Desomosome attachments of Keratinocytes Stratum Granulosum = cells contain Keratohyaline granules Stratum Corueum = flattened, anucleated cells containing keratin |
|
|
What are the 4 cells within the Epidermis & explain each
|
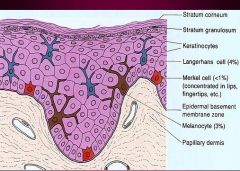
Keratinocytes = form the multilayered epidermis; produce keratin proteins
Melanocytes = provide color & protection from UV radiation; derived from Neural Crest ectoderm; located in Stratum Basalis; transfers Melanosomes by dendritic processes to Keratinocytes Langerhans cells = APC cells Merkel Cells = tactile function of the skin |
|
|
What 2 lamina does the Basement Membrane of the skin contain?
|
Lamina Lucida: with Bullous Pemphigoid antigens
Lamina Densa |
|
|
What are the 2 zones of the Dermis?
|
1. Papillary Dermis = upper, below the Epidermo-dermal jxn; contains loose CT
2. Reticular Dermis = deep, dense collagen, bordering on SubQ tissue |
|
|
What are the Primary Skin lesions that contain NO fluid?
|
Macule
Papule Plaque Nodule |
|
|
What are the Primary Skin lesions that contain fluid?
|
Vesicle
Bulla Blister Pustule |
|
|
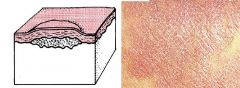
1. Macule
2. Patch |
Flat area of skin with discoloration
1. < 5 mm 2. > 5 mm |
|
|
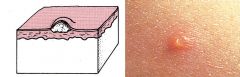
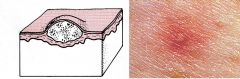
Papule
|
Elevated solid area 5 mm or less
|
|
|
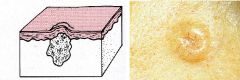
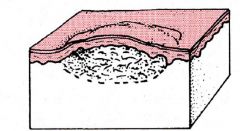
Plaque
|
Elevated flat-topped area, greater than 5 mm
|
|
|
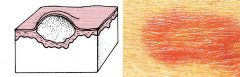
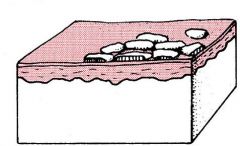
Nodule
|
Solid elevated area, greater than 5 mm
|
|
|
Vesicle
|
Fluid-filled raised area, less than 5 mm
|
|
|
Bulla
|
Fluid-filled raised area, greater than 5 mm
|
|
|
Common term used for Vesicle or Bulla
|
Blister
|
|
|
Pustule
|
Discrete, pus-filled, raised area
|
|
|
Wheal
|
Transient, irregular pink elevation with surrounding edema
|
|
|
Scale
|
Skin debris on the surface of the epidermis
|
|
|
Crust
|
Dried exudate over a damaged epithelium
|
|
|
Fissure
|
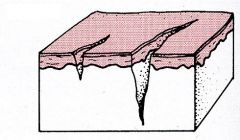
Crack in the epidermis, usually extending into the dermis
|
|
|
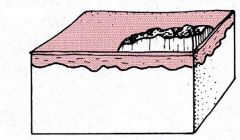
Ulcer
|
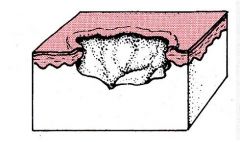
Loss of epidermis, extending into dermis or deeper
|
|
|
Hyperkeratosis
|
Stratum Corneum thickening = ?
|
|
|
1. Parakeratosis
2. Acanthosis |
1. nuclei retention in the keratinocytes of the Stratum Corneum = ?
2. Epidermal hyperplasia = ? |
|
|
Spongiosis
|
Intercellular Edema of the Epidermis = ?
|
|
|
Acantholysis
|
Separation of Epidermal cells from each other = ?
|
|
|
What is the pathogenesis of "disorders of Epidermal Maturation"? What disease is characterized by this?
|
Defect in the mechanism of desquamation; increased cohesiveness of the cells in the Stratum Corneum
Ichthyosis |
|
|
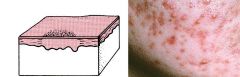
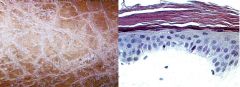
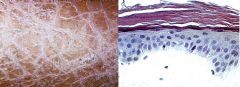
-Striking thickening of stratum corneum that is disproportionately thick in comparison with the nucleated epidermal layers
-Little or no inflammation |
Ichthyosis
|
|
|
Ichthyosis
-Striking thickening of stratum corneum that is disproportionately thick in comparison with the nucleated epidermal layers -little or no inflammation |
What is seen here?
|
|
|
What is the most common inherited skin disorder?
|
Ichthyosis Vulgaris
-Autosomal Dominant |
|
|
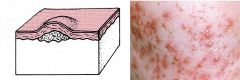
-Autosomal dominant or acquired
-Onset in childhood -Small white scales on extensor surfaces of the extremities and on the trunk and face (fish-like scales) |
Ichthyosis Vulgaris
|
|
|
-Usually mediated by local or systemic immunologic factors
-Last from days to weeks -Characterized by inflammation and edema |
Acute Inflammatory Dermatoses
-Urticaria & Angioedema -Acute Eczematous Dermatitis -Allergic Contact Dermatitis -Erythema Multiforme |
|
|
-Type I, IgE-dependent hypersensitivity
-Antigens include pollens, foods, drugs, insect venom -Degranulation of mast cells -> dermal microvascular permeability -> pruritic edematous plaques (wheals) |
Urticaria & Angioedema
|
|
|
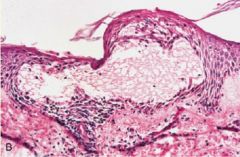
Pruritic papules and plaques that appear and disappear within a few hours
|
Urticaria & Angioedema
|
|
|
How is Angioedema different from Urticaria?
|
Deeper edema of both the dermis & subcutaneous fat
|
|
|
What is the treatment for Urticaria & Angioedema?
|
Avoid the offending agent
Prompt administration of Antihistamines = b/c its a Type I HS rxn |
|
|
Urticaria or Angioedema = Type I HS rxn
|

What type of Acute Inflammatory Dermatoses is this?
|
|
|
Urticaria
-dermal edema -scattered lymphocytes & mast cells |
What type of Acute Inflammatory Dermatoses is this?
|
|
|
-All are characterized by red, papulovesicular, oozing, and crusted lesions.
-Persistent lesions become less wet, and progressively scaly |
Acute Eczematous Dermatitis
|
|
|
Acute Eczematous Dermatitis
|
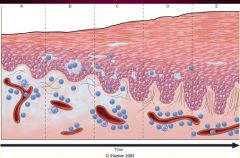
These are the stages of what Acute Inflammatory Dermatoses?
|
|
|
-T-cell mediated reaction to foreign antigens (Type IV HS)
-possible antigens: Poison ivy, rubber glove, dyes, cosmetic, minerals (gold ring, nickel) -intensely pruritic erythema & vesicles -Histology shows spongiosis, vesicles, & superficial perivascular lymphocytic infiltrate |
Allergic Contact Dermatitis
|
|
|
Allergic Contact Dermatitis
|

What is this picture illustrating?
|
|
|
Allergic Contact Dermatitis
|

What is this showing?
|
|
|
Allergic Contact Dermatitis
-T-cell mediated reaction to foreign antigens (type IV hypersensitivity) -spongiosis, vesicles and superficial perivascular lymphocytic infiltrate |
What is seen here?
|
|
|
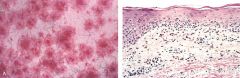
-Usually a reaction to a drug (sulfonamides), or an infectious agent (herpes simplex)
-A sparse infiltrate of lymphocytes in the upper dermis and small individually necrotic keratinocytes -Both humoral and delayed type hypersensitivity contribute to the pathogenesis of EM -> epithelial cells killed by CD8+ cytotoxic T lymphocytes |
Erythema Multiforme
|
|
|
Macules, papules, vesicles, & bullae,characteristic "target lesion"
Symmetric involvement of the extremeties |
Erythema Multiforme
|
|
|
An extensive & life-threatening form of this disease is called Stevens-Johnson Syndrome
-often in children -erosions & hemorrhagic crusts involve the lips & oral mucosa |
Erythema Multiforme
|
|
|
Erythema Multiforme = target lesions
|

What skin lesion is this?
|
|
|
Erythema Multiforme
-A sparse infiltrate of lymphocytes in the upper dermis and small individually necrotic keratinocytes |
What skin condition is this?
|
|
|
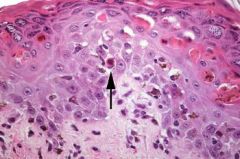
Erythema Multiforme
-vacuolization and necrosis of basal keratinocytes that are being attacked by T-lymphocytes with some necrotic keratinocytes (colloid bodies) in the epidermis |
What Acute Inflammatory Dermatoses is this?
|
|
|
What are 3 examples of Chronic Inflammatory Dermatoses?
|
1. Psoriasis
2. Lichen Planus 3. Lupus Erythematosus |
|
|
Psoriasis:
1. how common? 2. where more common? 3. Etiology? 4. Macroscopic appearance? 5. Where do new lesions occur? |
1. common = 1-2% of all people
2. Scandanavia, less common in Africa & China, nonexistent in Native American Indians 3. Genetic predisposition, multifactorial 4. Large, erythematous, scaly, plaques on the extensor dorsal surfaces 5. At the site of minor skin trauma = Koebner's Phenomenon |
|
|
What are 3 examples of Chronic Inflammatory Dermatoses?
|
1. Psoriasis
2. Lichen Planus 3. Lupus Erythematosus |
|
|
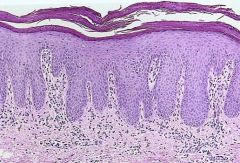
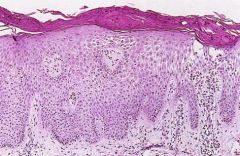
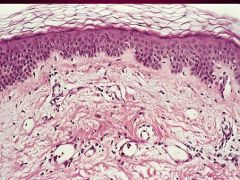
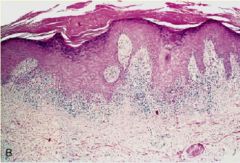
Psoriasis
-large plaque with scales -Acanthosis = epidermal hyperplasia -Parakeratosis = nuclei retention in Stratum Corneum -elongation of Rete Ridges |
What is seen here?
|
|
|
Psoriasis
-Acanthosis = epidermal hyperplasia -elongation of Rete ridges -Parakeratosis = nuclei retention in Stratum Corneum -extension of the Papillary Dermis close to the surface epithelium = blood vessels in the dermis rupture when scales are picked off = Auspitz sign |

What is this?
|
|
|
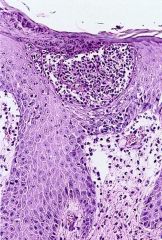
Psoriasis
-Munro Microabscess |
What is this picture showing?
|
|
|
-Marked acanthosis with regular downward elongation of the rete ridges
-Extensive overlying parakeratotic scale with thinned or absent stratum granulosum -Supra-papillary thinning with dilated and tortuous blood vessels within these papillae |
Psoriasis
|
|
|
Auspitz sign: multiple minute bleeding points when the scale is lifted from the plaque. Dx?
|
Psoriasis
|
|
|
Munro’s microabscesses: collections of neutrophils within the parakeratotic stratum corneum . Dx?
|
Psoriasis
|
|
|
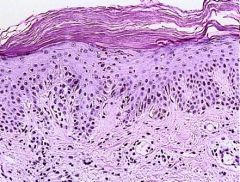
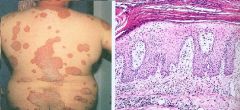
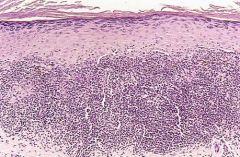
-“Pruritic, purple, polygonal papules”
-Self-limiting and resolves within 1-2 years Flexor surfaces of the wrists |
Lichen Planus
|
|
|
Lichen Planus
-Pruritic, purple, polygonal papules -usually on wrists |

What is seen here?
|
|
|
Lichen Planus
-band-like epidermal lymphocytic infiltrate -Hypergranulosis = Stratum Granulosa is thickened |
What is seen here?
|
|
What is seen here?
|
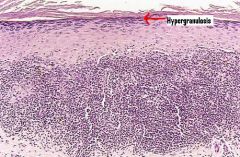
Lichen Planus
-Band-like dense infiltrate of lymphocytes at the dermo-epidermal junction -Hypergranulosis, angulated zig-zag contour of dermoepidermal interface (saw-toothing) |
|
|
Band-like dense infiltrate of lymphocytes at the dermoepidermal junction
Hypergranulosis, angulated zig-zag contour of dermoepidermal interface (saw-toothing) |
Lichen planus
|
|
|
Autoimmune disease mediated by deposition of circulating immune complexes along the dermoepidermal junction
|
Lupus Erythematous
|
|
|
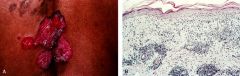
T or F: Discoid Lupus Erythematous usually develops into systemic disease
|
False
|
|
|
Where does Discoid Lupus Erythematosus usually occur?
|
Above the neck, sun exposed areas, including face (in the malar area), scalp, ears
|
|
|
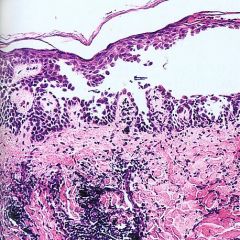
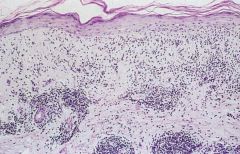
Discoid Lupus Erythematosus
-Epidermal atrophy, band-like lymphocytic infiltrate, vacuolated basal keratinocytes, apoptotic bodies, thickened and reduplicated lamina densa |
What is seen here?
|
|
|
Granular deposits of IgG and C3 along the dermoepidermal junction
|
Discoid Lupus Erythematosus
|
|
|
Discoid Lupus Erythematosus
-atrophy of the epidermis with an interface type of inflammation (affecting the basal layer of the epidermis causing vacuolization of the basal keratinocytes) with a superficial and deep inflammatory infiltrate |
What is seen here?
|
|
|
Discoid Lupus Erythematosus
-DIF: Granular deposits of IgG and C3 along the dermoepidermal junction (lupus band) |

What is this?
|