![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
45 Cards in this Set
- Front
- Back
|
Cardinal Signs of Inflammation |
Rubor Calor Dolor Tumor (functio laeso) |
|
|
Cardinal Signs with causes |
Rubor -- Vasodilation of Arterioles (erythromatous) Calor -- Vasodilation of arterioles -Caused by prostoglandins and NO Tumor -- Edema via vascular permeability in venules (edematous) -Bradykinin, histamine, C3a, C5a ... Dolor -- mainly via bradykinin
|
|
|
Five steps to inflammation, the "5 Rs" |
1. Recognition of agent 2. Recruitment of leukocytes 3. Removal of agent 4. Regulation of response 5. Resolution/repair |
|
|
Leukocyte response to agent |
1. Marginization -Via stasis and ^ blood viscosity 2. Rolling -Weak binding of Lewis-X to E,P-selectins 3. Adhesion -Strong binding of integrins to ICAMs -B2 integrin (CD18) exclusive to leukocyte 4. Diapedesis -Mainly in postcapillary venules -Involves PECAM-1 (CD-31)
|
|
|
Weibel-Palade Bodies |
Storage of P-selectin in endothelial cells -Also vWF |
|
|
Cell surface receptors |
1. GPCR -- Seven transmembrane regions -Recognize N-Forylmethionyl 2. TLRs -- LPS on bacteria, others 3. Cytokine receptors -Ex- IFNy 4. Phagocytosis receptors |
|
|
The Inflammosome |
Protein oligomer: -Caspase 1, PYCARD, NALP -Pormotes maturation of IL-B1, IL-18 -Pyroptosis --> Cell death with inflammatory response |
|
|
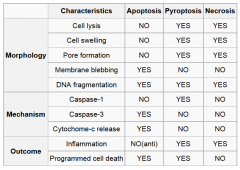
Comparison of apoptosis, necrosis, and pyroptosis |
|
|
|
The Respiratory burst reaction (withing the 2` lysosome) |
1. NADPH oxidase (membrane bound) yields oxygen radiacl 2. Superoxide dismutatse / sponatneous yields H202 3. Fetton reaction (w/ iron) gives hydroxyl radical 4. Myeloperoxidase (w/ Cl-) gives hypoclorous acid 5. Catalase yields H2O ad O2 |
|
|
LAD type 1 |
"Leykocyte Adhesion Deficiency"
-Decreased Expression of B2 integrin (CD18) -Neutrophils present in bloodd near site of infection, but NOT in tissue -Decreased wound healing -Delayed separation of umbilical cord
|
|
|
Chediak-Higashi Syndrome |
LYST mutation --> failure of fusion of phagosome and lysosome --> giant granules in all leukocytes -Also: albanism, pyogenic infections, "accelerated phase" (lymphoproliferative disease) |
|
|
Chronic Granulomatous Disease |
-NADPH Oxidase malfunction -->Decreased H202 Production -Pathogens that produce catalase NOT killed -Ex. Staph Aureas -Diagnosed with Nitroblue Tetrazoleum (NBT) -Normal: ROS cause NBT to become purple -CGD: No ROS, NBT remains blue
|
|
|
Stain -- NitroBlue Tetrazoleum |
-Stains yellow within neutrophils -Turns purple in presence of ROS -Negative test (no change) is POSITIVE for Chronic Granulomatous Disease |
|
|
Morphologies of Inflammation |
1. Serous Inflammation -Flluid with no fibrin or fibrinogen -Ex. Skin blister 2. Fibrinous Inflammation -Presence of fibrin -"Bread and Butter pericarditis" -Seen in percardial friction rub -Fibrin is RED on H&E 3. Suppurative Inflammation -Purulent = "with pus" -Many neutrophils (sign of accute inflammation) diffuse into tissue -Pyogenic bacteria --> pus forming 4. Abcess -- Neutrophils and necrotic debris -Seen with liquefactive necrosis 5. Pseudomembranous Inflammation -- Exudate of neutrophils AND fibrin will form membrane-like inflammation -Pseudomembranous colitis --> Note mushroom shaped pseudomembrane 6. Ulcer -- Degradation of epithelium due to inflammation -Distinguish from erosion, which will not completely destroy epithelium |
|
|
Systemic Effects of inflammation |
1. Fever (PGE2 from ant. hypothalimus) 2. Leukocytemia 3. Production of accute phase proteins -CRP, a1-antitrypsin, etc... 4. Increased ESR -Due to increased fibrinogen |
|
|
Serotonin |
-In platelet cells -Contraction of smooth muscle -Will produce 5-HIAA
-Carcinoid tumor --> Serotonin ^ -HIAA in urine |
|
|
Factor XII -- Hageman Factor |
Activates four systems: 1.Kinin -Kallikrein yeilds bradykinin from HMWK 2.Clotting 3.Complement 4.Fibrinolytic |
|
|
lComplement Deficencies & diseases |
1. C2,C4 -SLE-like symptoms -Due to build-up of immune complexes 2. C3 -recurrent infections by pyogenic bacteria like SA 3. C6,7,8 -neisseria -No MHC 4. Decay Accelerating Factor -Usu. inhibits complement activation via decaying C3 convertase -hemoglobinuria -pancytopenia 5. C1 inhibitor --> herediatary angioedema (swollen lips/face) -Excess c2b and bradykinin 6. Factor H -Usu. regulates alternative complement pathway -->increased vascular permeability w/ macular degeneration -->atypical hemolytic uremic syndrome |
|
|
Eicosanoids: |
Prostaglandin Prostacyclin Thromboxane Leukotrienes
-PG hydrolysis is rate limiting step |
|
|
Prostaglandins |
Prostaglandin G2 via COX1,2 -Inibited by steroids, aspirin, indomethacin PGI2 = prostacyclin -From endothelial cells -Vasodilation, Inhibits platelet aggregation -cAMP^ TXA2 = Thromboxane -From platelets -Vasoconstrict, promote platelet agg -IP3 ^ PGE2 -Fever production -From ant. Hypothalamus -Patent Ductus Arteriosus -Osteoid Osteoma PGF2 -Uterine contraction, broncoconstriction |
|
|
Leukotrienes |
LOX converts arachidonic acid to 5-HPETE 12 lipoxygenase yields Lipoxin A4 and B4
-Slow reacting substance of anaphylaxis -Bronchoconstriction = "Aspirin induced asthma"
Lipoxin: -Inhibit neutrophil chemtaxis and adhereance to endothelium - |
|
|
Drugs for COX |
-COX 1 is constituative -COX 2 is inducible
Aspirin will inhibit BOTH prostaglandins and thromboxanes, but prostaglandins can recover due to their nucleated cell source -Thus aspirin will inhibit blood clots |
|
|
Neutrophils |
>5 Lobes = Hypersegmented nucleus -Megaloblastic Anemia -Band cell is immature neutrophil -Indicative of bacterial infection, accute inflammation
White area on brain surface = Acute bacterial meningitis
|
|
|
Lymphocytes |
-B cells, T cells NK cells -Stain darkly, very little cytoplasm -B cells = "clock face", plasma cells have eccentric nucleus (abundant RER) -Indicate viral infection -Present in chronic inflammation - |
|
|
Monocytes |
-Kidney-bean nucleus, "ropey" chromatin -Cytoplasmic vacules -Activated monocyte = epitheliod cell -Abundant cytoplasm -Activated by IFNy, Th2
|
|
|
Eosinophils |
-Nucleus is bi-lobed -Many eosiniphilic granules -Contain Major Basic Protein (MPB), histaminase -On EM these granules have a dark center
-Role in allergic reactions and parasites |
|
|
Basophils, Mast Cells |
-Bind IgE, have dark (basophilic) granules with histamine, leukotriene, etc... |
|
|
Granuloma |
Aggregation of epitheliod cells (note abundant pink cytoplasm) -Lymphocytes or giant cells may be present
-May become fribrotic, hyalinize, or become calcified (apparent on X-ray)
|
|
|
Granulomatous Diseases |
1. TB (caseating granuloma / tubercle) 2. Leprosy -- Acid-fast Bacilli 3. 4. Cat-scratch disease 5. Sarcoidosis 6. Chron's Disease -- Autoimmune like reaction to normal flora |
|
|
Ceseating granuloma |
EX: TB Causes caseating necrosis in lung NOTE: that center is different from periphery -Due to ischemia and necrosis of granuloma center -Langhan's giant cells |
|
|
Non-caseating granuloma |
EX: Sarcoidosis -Unknown etiology -Non-caseating granuloma in many tissues -Presents with Hypercalcemia, Increased ACE -This presentation is diagnostic for sarcoidosis |
|
|
Epidermal Growth Factor (EGF) |
-TGFa is similar -Mitogenic for epithelial cells and fibroblasts |
|
|
Hepatocyte Growth Factor (HGF) |
"Scatter factor" Mitogenic for most epithelia Role in cancer: -Activates oncogenic pathway -Angiogeneis -Scatter (cell dissociation) --> metastasis |
|
|
Vascular Endothelial Growth Factor |
-Promote angiogenesis -Avastin blocks activity |
|
|
Platelet Derived Growth Factor |
Role in fibrosis of bone marrow |
|
|
Fibroblast Growth Factor |
Both acidic and basic form -Acidic from activated Macrophages -Basic from neural tissue -Role in: -Angiogenesis -Wound repair -Hematopoesis
|
|
|
Transforming Growth Factor B |
Can inhibit OR stimulate growth -Anti-inflammatory -Fribrogenic |
|
|
Tyrosine Kinase Activity |
-EGF,FGF,TGF,HGF |
|
|
GPCR Reactions |
1. Gs - ATP --> cAMP -Cholera toxin inhibits breakdown of active complex (Gs-GTP) 2. Gi -Inhibits adenylene cyclase --> cAMP \/ -Pertussis toxin inibits formation of active complex (Gi-GTP). This leads to an increase in cAMP 3. Gq Simulstes PLC, --> IP3 ^, DAG ^ --> Intracellular Ca++ ^ -->Arachidonic acid ^ 4. Gt -GTP --> cGMP -Ex. Rhodopsin in retina 5. G12,13 -Actin cytoskeletal remodeling |
|
|
Composition of the interstitial matrix and the basement membrane |
Interstital Matrix: -Fibrilar collagens -Elastin -Proteoglycan and hyaluronan Basement Membrane: -Type IV collagen -Laminin -Proteoglycan |
|
|
Collagen |
Secreted from fibroblasts Stains RED in H&E Stains BLUE in trichrome stain Excess proliferation --> keloids
Types: I -- Skin, bone, tendons, mature scars -Disease associate: OI II -- Cartilage III -- Embryonic tissue, blood vessels, pliable organs -Is first type deposited in wound healing (followed by type I) IV -- Basement membranes -Disease Associate: Alport syndrome -Disease Associate: Goodpasture disease (autoantibodies vs. Type IV) |
|
|
Stain -- Tricrome |
Red: Muscle and keratin Blue: Collagen and bone |
|
|
Elastin |
Surrounded by fibrilin -Fibrilin abnormal with Marfan syndrome Stains black upon special staining |
|
|
Angiogenesis |
VEGF is most important factor -Tip cells ONLY proliferate -Via DLL4 from VEGF -Not stalk cells -Tip cells express notch-1, which blocks effect of DLL4 on stalk cells |
|
|
Diseases of repair / wound healing |
1. Keloids -- Overgrowth of collagen -Common in African Americans 2.Pyomatuos Granuloma -Excess granulation tissue forms small mass -Lobular hemangioma 3. Contracture / Fibromatosis -Due to secondary union / intention -Large ,open wound -Example: Duputyren's Contracture -4th, 5th fingers |