![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
73 Cards in this Set
- Front
- Back
|
List 4 components of normal hemostasis. |
1. primary hemostasis (platelets) 2. secondary hemostasis (coagulation cascade) 3. fibrinolysis 4. regulation of hemostasis |
|
|
List 3 general types of abnormal hemostasis. |
1. hemorrhage 2. thrombosis 3. DIC |
|
|
What does hemostasis accomplish, what are the 3 major components of hemostasis, and how are these components activated?
|
Prevents blood loss, while maintaining blood in fluid state. Platelets Endothelial cells Blood clotting proteins in plasma Activation, and subsequent coagulation, triggered by injury to the vessel (endothelium) |
|
|
What are the 5 steps of hemostasis? Which steps are involved in primary hemostasis and which steps are involved in secondary? |
1. vasoconstriction 2. platelet plug formation 3. coagulation to form fibrin mesh 4. fibrinolysis 5. repair at damaged site Steps 1 and 2 = primary hemostasis Step 3 = secondary hemostasis |
|
|
What occurs during primary hemostasis? |
-immediate vasoconstriction: reflex- and endothelin-induced -vessel injury exposes subendothelium (BM) -platelets activated when exposed to ECM: collagen, proteoglycans, fibronectin, glycoproteins -platelets adhere: directly (collagen) or via von Willebrand's factor -platelet shape change consolidates platelet plug -platelet degranulation: alpha and dense granules, thromboxane, ADP, Ca++ -platelet aggregation forms loose plug --> primary hemostatic plug |
|
|
What does thromboxane do during primary hemostasis?
|
Induces vasoconstriction. Necessary for platelet aggregation. |
|
|
What occurs during secondary hemostasis? |
Tissue factor produced by endothelial cells. Phospholipid complex (on platelet surface). Plasma clotting factors become activated. Fibrin formation Fibrin cements the platelet aggregate --> secondary hemostatic plug |
|
|
What is the end product of secondary hemostasis? |
Fibrin, which comprises the secondary hemostatic plug. |
|
|
What are the components of the coagulation cascade in secondary hemostasis? |
Enzymatic coagulation factors. Non-enzymatic coagulation factors. Ca++ Phospholipid membs |
|
|
Intrinsic, extrinsic, and common pathways work together to produce _____, AKA factor ____, with a final product of _____, AKA factor ____> |
thrombin II fibrin I |
|
|
What occurs/what is involved in the intrinsic pathway of secondary hemostasis?
|
-contact factors -vascular injury: pre-kallikrein-HMWK and factor XII bind to phospholipids of injured endothelial cells -catalytic cascade -IXa, VIIIa, phospholipid and Ca++ from TENASE -tenase activates factor X and initiates common pathway |
|
|
What occurs/what is involved in the extrinsic pathway of secondary hemostasis? |
Tissue factor: sub-endothelium, activated endothelium -endotoxin, TNF, IL-1, thrombin all stimulate TF production: sepsis -TF-VIIa activates X |
|
|
What occurs/what is involved in the common pathway of secondary hemostasis? |
-activated Xa: bound to endothelial or platelet memb, converts prothrombin (II) to thrombin (IIa) -thrombin has multiple functions FIBRIN FORMATION |
|
|
Fibrin is formed from _____ by _____. |
fibrinogen thrombi |
|
|
True or false? Fibrin self-polymerizes. |
True |
|
|
Fibrin self-plymerizes and is cross-linked by factor _____. |
XIIIa |
|
|
What is formed by cross-linking of fibrin, and platelet contraction? |
a strong, fibrin-platelet thrombus |
|
|
How is a thrombus retracted? |
By platelet retraction: allows blood flow around, and pulls damaged vessel edges closer together. |
|
|
True or false? Intrinsic and extrinsic cascades reflect in-vivo events. |
False |
|
|
What happens when tissue factor is exposed to plasma major activator? |
IX activation --> by-pass intrinsic pathway (Thrombin on its own cannot convert enough fibrinogen to fibrin.) |
|
|
Thrombin activates _____ and factor ____, ___ , ____, and ____. What is accomplished by activation of these factors? |
platelets V VIII XI XII Activation of large quantities of thrombin. |
|
|
True or false? The fibrin-platelet plug is normally permanent. |
False. Temporar |
|
|
What controls thrombus size? |
Fibrinolysis, which is dissolution of the fibrin-platelet plug. |
|
|
What does thrombomodulin do? |
Blocks coagulation cascade |
|
|
What is the key enzyme in fibrinolysis? |
Plasmin |
|
|
Plasminogen is activated into ____ by _____ and _____. |
plasmin coagulation factors plasminogen activators in endothelium and tissue |
|
|
Fibrin is degraded to ______, which are an important clinical measurement of ____. |
fibrin degradation products (FDP) uncontrolled coagulation |
|
|
What does the regulation of hemostasis achieve?
|
Restriction of clot to site of vessel injury |
|
|
What is antithrombin III (ATIII) and what does it do? |
The most potent anticoagulant. Binds to heparan sulfate on endothelium and degrades all activated coagulation factors, except VIIa. |
|
|
What 3 compounds inhibit thrombosis? |
ATIII Protein C TFPI (tissue factor pathway inhibitor) |
|
|
What are the 2 types of fibrinolytic inhibitors? |
Plasminogen activator inhibitor-1 (PAI-1): inhibits tiss plasminogen activator, and therefore plasmin formation; inactivates protein C, plasmin, and thrombin Antiplasmins: co-operatively prevent excess plasmin activity (slows thrombus dissolution |
|
|
What are the 2 broad categories of hemostatic disorders? |
Too little coagulation --> hemorrhage Too much coagulation --> thrombosis |
|
|
List 4 things that can cause hemorrhage. |
Abnormal func/integrity of major factors that influence hemostasis: 1. blood vessel 2. endothelium 3. platelets 4. coagulation factors |
|
|
What can compromise a blood vessel that might cause hemorrhage?
|
Trauma (rhexis) Vascular erosion: inflammatory, invasive tumors, fungi (eg Aspergillus) Diapedesis (small defects in otherwise intact vessels allow some RBC to escape) Blood vessel wall malformation: Ehlers-Danlos syndrome, vit C deficiency |
|
|
What can cause endothelial injury that leads to hemorrhage? |
Endotoxemia Vasculitis: virus (eg canine adenovirus-1), tick-bourne diseases Uremic toxins Immune complexes (Type III hypersensitivity rxn) |
|
|
What can cause platelet dysfunction/depletion that leads to hemorrhage? |
Thrombocytopenia (decreased platelet #): decreased production in bone marrow, increased destruction (immune-mediated, some viruses), increased use (DIC) Abnormal platelet function: inherited, drug-induced (Aspirin), uremia (renal failure) Secondary platelet dysfunction: von Willebrand's disease (esp in Doberman's) |
|
|
What can go wrong with coagulation factors, which may lead to hemorrhage? |
Congenital defects (hemophilia): decreased conc, functional deficiency Acquired defects: decreased production - liver disease (most factors), vit K deficiency (affects II, VII, IX, X), eg that caused by Warfarin; increased consumption - DIC |
|
|
True or false?
Cardiac tamponade can be expected in dogs with Warfarin toxicity. |
True |
|
|
List 6 types of hemorrhage. |
Petechiae Purpura Ecchymosis Suffusive Hematoma Hemorrhage within body cavity |
|
|
What are petechiae? |
Very small (1-2mm) areas of hemorrhage on serosal surfaces, caused by diapedesis, indicating minor vascular damage |
|
|
What is purpura? |
Small (3mm-2cm) areas of hemorrhage. |
|
|
What is ecchymosis?
|
Larger (2-cm) areas of hemorrhage that indicate more extensive vascular damage. Includes subcutaneous hematomas (bruises). |
|
|
Explain the colouration of a bruise. |
Macs degrade and phagocytose RBCs --> release of red-blue Hb, blue-green bilirubin, and gold-brown hemosiderin |
|
|
What is suffusive hemorrhage? What can cause it? |
Hemorrhage that affects a large contiguous area. eg. caused by vit C deficiency in GPs |
|
|
What is hematoma? |
Hemorrhage within a confined space. eg aural hematoma |
|
|
List 3 types of hemorrhage within a body cavity.
|
hemoabdomen hemothorax hemopericardium |
|
|
True or false? Rapid loss of up to 20% of blood V can be tolerated by the body. |
Tru |
|
|
True or false? Slow rate of blood loss can be tolerated. |
Tru |
|
|
Rapid loss of >20% blood V usu results in _____. |
hypovolemic shoc |
|
|
What are the possible clinical consequences of hemorrhage? |
hypovolemic shock cardiac tamponade loss of iron and subsequent iron deficiency anemia: predominantly external hemorrhage (from GIT); internal hemorrhage - iron is preserved and recycled |
|
|
What are 3 possible resolutions of hemorrhage? |
1. resorption: small amount 2. organization: larger amounts, phagocytosis and digestion of Hb 3. organizing hematom |
|
|
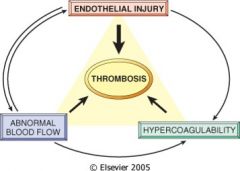
Define thrombosis. |
Formation of inappropriate (excessive) thrombus in the wall of a blood or lymphatic vessel, or heart, or free in lumen (thromboembolism) |
|
|
Draw Virchow's triad. |
|
|
|
What can cause endothelial injury, leading to thrombosis? |
vasculitis (viral, bacterial, fungal) immune-mediated toxic DIC |
|
|
Endothelial injury exposes ____, _____, and _____. Why do exposure of these things cause thrombosis? |
TF (affecting extrinsic coagulation) collagen fibronectin All are potent stimuli for platelet adhesion, and trigger the coagulation cascade. |
|
|
What usually prevents thrombus formation in the heart or arterial circulation?
|
High rate of flo |
|
|
List 2 ways that blood flow can be altered, and how these can lead to thrombosis. |
Reduced blood flow: systemic heart failure, local congestion Turbulent blood flow: aneurysm, narrowing vessels Alteration in flow can lead to increased contact of platelets and endothelial cells, and the accumulation of activated coagulation factors. |
|
|
What can cause hypercoagulability, leading to thrombosis?
|
1. Increased conc of activated clotting factors: increased activation (inflammation, stress, pregnancy, surgery, renal disease), or decreased degradation (liver disease). 2. Decreased conc of anti-coagulation factors: decreased ATIII w renal disease in dogs |
|
|
Cardiac and arterial thrombi are usually due to ____. |
endothelial damage |
|
|
Cardiac and arterial thrombi are made up of predominantly ____ and _____ and are therefore ____ in colour. |
platelets fibrin pale |
|
|
Venous thrombi are usu due to ____. |
blood stasi |
|
|
Which cells are commonly incorporated into venous thrombi, and how does this affect the colour of the thrombi? |
RBCs red |
|
|
When performing a PM, it important to distinguish cardiac/arterial thrombi and venous thrombi from _______ coagulation. |
post-mortem |
|
|
What prevents the incorporation of RBCs in cardiac and arterial thrombi?
|
fast flow of bloo |
|
|
What are 4 possible fates of the thrombus? |
Propagation: accumulate more platelets and fibrin, eventully leading to vessel obstruction. Dissolution: removal by fibrinolytic activity. Organization and recanalization: fibrosis. Embolism: dislodge and travel to other sites. |
|
|
What are thromboemboli? |
Dislodged fragments of thrombus. |
|
|
What 3 things may occur if a thromboembolism lodges in a smaller vessel? |
1. venous thromboembolism: typically lodge in pulmonary cir 2. arterial thromboembolism: lodge downstream, typically at a vascular bifurcation 3. cardiac thromboembolism: often lodge at iliac bifurcation |
|
|
What kind of thromboembolism is a saddle thrombus? |
cardiac thromboembolism bc lodging at iliac bifurcation |
|
|
Besides thromboemboli, what other types of emboli are there? |
bacterial emboli: abscesses or valvular endocarditis fat emboli: fracture (releasing bone marrow), usu lodge in pulmonary circ fibrocartilaginous emboli: ruptured intervertebral disc, localized spinal cord infarction intravascular parasites: heartworm malignant neoplasms |
|
|
What does DIC stand for? |
Disseminated intravascular coagulation. |
|
|
What is DIC? |
Sever malfunction of hemostasis, often resulting in death, that is characterized by excessive (systemic) generation of thrombin/TF. |
|
|
What causes DIC? |
-diffuse vascular damage (trauma, vasculitis, burns): exposure of endothelial TF -bacteremia and systemic infections: intravascular generation of TF by endothelial cells and monocytes. |
|
|
Explain the pathogenesis of DIC. |
Excessive generation of TF --> TF-induced activation of extrinsic cascade --> Thrombin production, platelet aggregation, and fibrin formation --> widespread intravascular clots, widespread consumption of clotting factors and platelets, and thrombin-stimulated fibrinolysis. Widespread intravascular clots lead to thrombosis. |