Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back
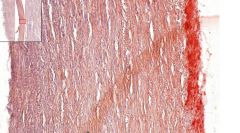
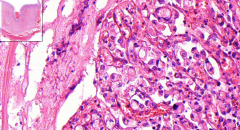
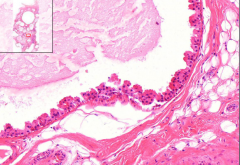
Foamy cells due to accumulation of fatty droplets
- Macrophages - Smooth muscle cells Etiology? |
Lipoid streak of aorta
Early stage of atherosclerosis |
|
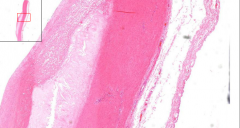
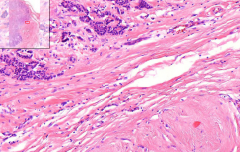
- Hyaline fibrotic tissue (fibroblasts, smooth muscle, foamy cells)
- Covered with fibrous layer (fibrous cap) - Centrally: Amorpheus necrotic tissue Etiology? Macro? Risk factors? Complications? |
Atherosclerotic plaque (atheroma) of aorta
Etiology - Lipoid streak --> Fibrotic plaque --> Atherosclerotic plaque --> Complicated plaque Macro - Yellow, soft consistency, sometime calcifications Risk factors - Hyperlipidemia - Hypertension - Smoking - DM Complications - Small & medium vessels: Ischemia due to obstruction - Large vessels: Aneurysm due to thin wall |
|
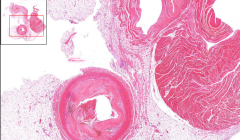
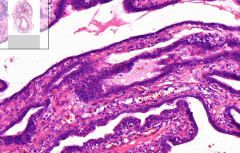
Thrombus
- Blood elements - Fibrin - Platelets Intimal layer thickened with fibrotic plaque - Central parts: Amorpheus material, lipophages - Basal parts: Vasa vasorum grow into plaque from adventitia - Siderophages, dystrophic calcifications |
Sclerosis and thrombosis of coronary artery
|
|
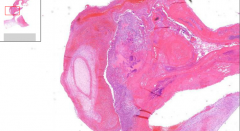
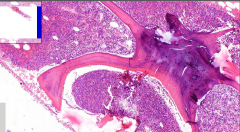
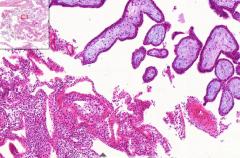
- Thrombus with fibrin
- Bacterial colonies - Adjacent valve with necrosis - Leukocytic infiltration - Organization (healing with granulation tissue) Etiology? Macro? Complications? Clinically |
Infectious endocarditis
Etiology - Bacteremia/septicemia of staphylococci, streptococci, G- bacilli, mycosis Macro - Irregular protuberances on endocardium, especially on valves of left heart Complications - Rupture of valve - valvular insufficiency - Embolization of thrombotic parts --> Infectious emboli --> Abscesses Clinically - Sepsis - Kidney / CNS symptoms |
|
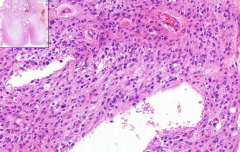
- Lymphoplasmocytic infiltration of myocardium
- Small necrosis - Death (heart failure) Etiology? Macro? Complications? |
Viral myocarditis
Etiology - Viral infection (Coxsackie, A,B, ECHO, influenza, rubella) Macro? - Heart enlargement - Dilatino of all heart spaces - Pericarditis Complications - Dilated cardiomyopathy |
|
- Small nodules in interstitial tissue = Rheumatic nodules, made of modified histiocytes:
-- Ashoff cells (large, basophilic, 1-3 nuclei) -- Anitschkov cells (small, 1 nuclei, chromatin center) Etiology Complications |
Rheumatic myocarditis
Part of pancarditis in rheumatic fever - Cross reaction (3 weeks after b hemolytic streptococci infection) - Autoantibodies against both streptococci and CT of host - Development starts with fibrinoid necrosis - accumulation of macrophages Complication - Death |
|
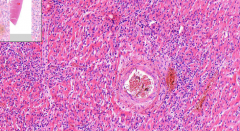
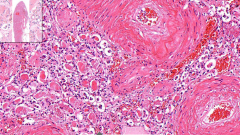
Kidney
- Thrombosis & infarction in affected part of artery - Inflammatory infiltration - Fibrinoid necrosis of vessel wall (&thickening) Etiology? |
Polyarteritis nodosa (PAN)
- Disease of small and median vessels - Unknown etiology - Affect all organs EXCEPT lungs |
|
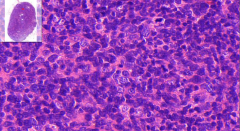
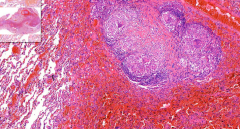
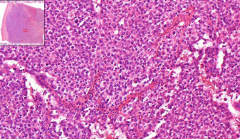
Lymph node
- Destroyed normal structure - Fibrotic binds - Peripheral eosinophilia - Reactive, infiltrative background - Pathognomonic cells - 2 types? Etiology? |
Hodgkins lymphoma
= Malignant tumor derived from lymphoid cells - of lymph node origin Pathognomonic cells: - Reed-Sternberg cells - large multinucleated, eosin nucleoli - Hodgkin cells - 1 nucleus Together = H/RS cells Infiltrate is: - Lymphocytes & eosinophilic granulocytes |
|
Lymph node
- Follicular pattern - Small - angulated cells are? - Large, vesicular nuclei cells are? - Germinal centers in medulla - cells are activated Etiology? |
Non-Hogdkins lymphoma / follicular lymphoma
= Malignant tumor derived from lymphoid cells, with 3/4 arising in lymph nodes Small cells = Centrocytes Large cells = Centroblasts - No macrophages eating cells - B cells are immortal |
|
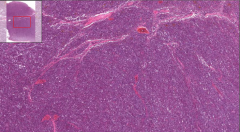
Lymph node
- Monotonous infiltration of small lymphocytes obliterate whole node, spleen, marrow - Destroyed nodal structure - No germinal centers Etiology? |
Chrnoic lymphocytic leukemia (CLL)
= Monoclonal proliferation of small lymphocytes, leukemic form of lympocytic lymphoma B-cell type 95% T-cell type 5% Middle aged --> Old patients |
|
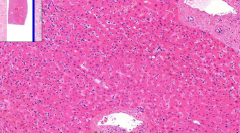
Liver
- Hypercellular liver - All maturation stages - Hepatocyte borders are lost |
Chronic myeloid leukemia (CML)
= Malignant transformation of stem cells - produce differentiated cells - especially neutrophils Symptom: - Acute leukemia |
|
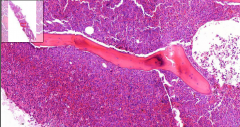
Bone marrow (see bone)
- Hypercellular: Granulocytes and megakaryocytes - May be fibrosis Etiology? Symptoms? |
Chronic myeloid leukemia (CML)
Megakaryocytes are pathological: Large with round nucleus. Usually nucleus is folded. Symptoms: - Pain due to pressure inside bones - Anemia - Thrombocytopenia NB! Marrow has almost no fat - so this SHOULD be a marrow of a 3 month old baby. So hypercellular |
|
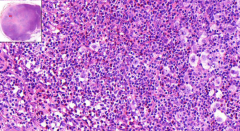
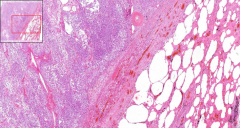
Bone marrow
- Hypercellular - Pathological plasma cells - what do they produce? with irregular, exentric cytoplasm - Tumor infiltration of bones (darker bones) Clinically? |
Plasmocytoma / multiple myeloma
Plasma cells are these large pink ones. Sometimes binucleated. Producing: - Paraprotein / Bence-Jones protein (urine), may produce tubular casts Clinical findings: - Plasma cell leukaemia - Increased calcemia - due to osteolysis - Paraprotein in blood - renal failure risk - Anemia + thrombocytopenia - Tumor lesion of bones on x-ray. |
|
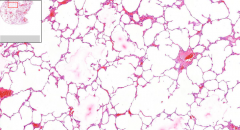
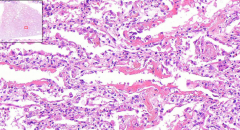
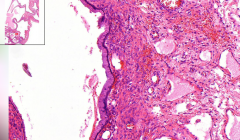
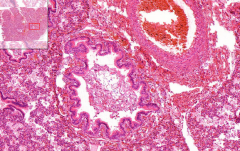
- Thin alveolar septa
- Rupture of septa --> Ends of capillaries protruding into free space Etiology? Complications? Macro? |
Pulmonary emphysema
= Permanent enlargement of airways distal to terminal bronchioli with destruction of airways Etiology: Centroacinar type - Smokers damage tissue with toxic compounds - Chronic bronchitis with protolytic enzymes Panacinar type - Alpha-1-antitrypsin defect --> Lack of protease inhibitor --> Lung damage - Affect whole parenchyma from beginning Complications - Pulmonary hypertension --> Cor pulmonale - Pneumothorax if rupture of bubbles Macro: - Honeycomb |
|
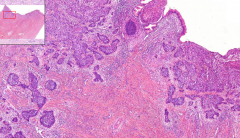
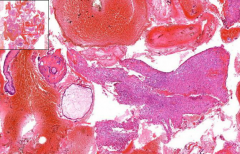
- Alveoli evenly filled with fibrin and leukocytes
Etiology? Complications? |
Lobar pneumonia
= Affecting one or two lobes of lung Etiology - Streptococcus pneumoniae Complications? - Pleuritis: Fibrinous --> Pyogenic --> Empyema - Pulmonary abscesses - Carnification/hepatization: Insufficient dissolution of fibrin - fibrous obliteration of alveoli + neutrophilic infiltration --> Lung fibrosis (grey and red carnification) Nb! Nowadays a very rare disease due to antibiotic treatment |
|
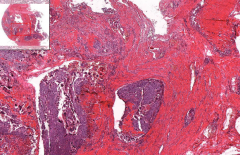
- Groups of alveoli filled with leukocytes - focal lesions, affected alveoli related from their respective inflammated terminal bronchioles
- Congested capillaries + neutrophil emigration Etiology? Sequels? |
Bronchopneumonia
- most common type - patchy consolidation Etiology Variety of bacteria - Staphylococci - Streptococci - Hemophilus Secondary process - Flu - Stroke - Immobility - Malignant tumors - Immunosuppressions |
|
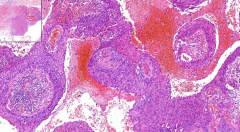
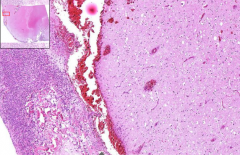
- Many granulomas - NO central necrosis / caseation (so not TB!)
- Granulomas are made up by? - Peripheral lymphocytic infiltration (purple) - Large multinucleated giant cells or - Schaumanns bodies (calcifications) - Asteroid inclusions Etiology? Complications? |
Sarcoidosis (lung)
= multisystemic granulomatous disease Granulomas - Epithelioid histiocytes - Multinucleated Giant cells of Langhans - Schaumann´s bodies - Asteroid inclusions Etiology? - Unknown Complications? - Lung fibrosis - Pulmonary hypertension - c. pulmonale |
|
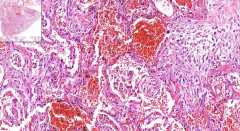
LUNG
- Dilated capillaries in alveolar septa - May see fibrin thrombi - Desquamation of alveolar epithelium - Alveoli filled with oedematic fluid - Fibrin --> Hyaline membranes Etiology? Consequences? |
Diffuse alveolar damage (DAD) - acute phase
= Morphological like ARDS Etiology Diffuse alveolar / endothelial damage by: *Exogenous - Inhalation of toxic gas - Aspiration of stomach juice *Endogenous - Uremia - Sepsis - Large burns - Crush syndrome - Idiopathic: Acute interstitial pneumonia (AIP) / Hamman-Rich syndrome Complications - 50% death acute phase - 50% interstitial fibrosis |
|
LUNG
- Hyperemic spots - Dilated capilaries - Fibrotic thickness of alveolar septa with lymphocytic infiltration - Septa covered with pneumocytes II type - Hyaline membranes with organized granulation tissue Etiology? Complications? |
Chronic phase of DAD
Etiology - Late phase of DAD Complications - Honey comb lung - Fibrosis --> Pulm. hypertension --> C. pulmonale Damage to capillaries and epithelium --> Fibrin leaks from capillaries leading to hyaline membranes ----> Type II pneumocytes replace damaged type I cells |
|
LUNG / BRONCHIOLI
- Cells of same type through whole depth of epithelium - Tumor spread in bronchial wall - growing into glands - Cellular and nuclear pleomorphism - Keratin pearls Etiology? Complications? |
Squamous cell carcinoma of lung
= Malignant bronchogenic tumor, originates in superficial bronchial epithelium as squamous metaplasia Etiology? - Smoking cancer agents - Genetic risks Complications - Metastasing - Obliteration of bronchi - pneumonia or collapse Keratin pearls - Different intra- and extracellular keratin production |
|
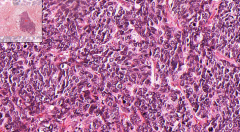
LUNG / BRONCHIOLI
- Big purple lesion in the middle of the slide - Small lymphocyte like cells, sometimes "oat" elongated - Mitotic activity (darker) in clusters of hyperchromatic cells Etiology? Complications? |
Small cell carcinoma of lungs
= Highly malignant bronchogenic carcinoma (most agressive lung cancer) - Highly invasive, rapid, aggressive growth - Arise from neuroendocrine cells Etiology - Cigarette smoking Complications - Early metastasing - Hormone production (ACTH) ---> "Paraneoplasitc syndrome" |
|
LUNG
- High, columnar cells with mucous production - Growth of tumor spread along alveolar wall (thus its name) Etiology? |
Bronchioalveolar carcinoma of lungs
= Lung adenocarcinoma Porogenic spread 2 forms: Multifocal - Several focuses - may resemble pneumonia Solitar - Tumor in upper lobar peripheral parts of lung Etiology - Cigarette smoking - Industrial and atmospheric pollution So these are 3 of the 4 histological types of lung cancers: 1. Small cell 2. Squamous carcinoma 3. Adenocarcinoma 4. Large cell carcinoma |
|
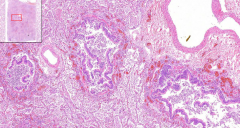
Kidney
- Elongated cysts w/flat ep. - Interspace with remnants of fetal tissue - Small glomeruli Etiology? |
Fetal type polycystic kidney disease / polycystosis
=Microcystosis - Oligohydramnion --> Potter face - Lungs compressed --> Death Etiology - Inborn AD developmental defect: 2 tubes in renal development does not fuse - ALL nephrons affected --> Filtrate is captured in cysts |
|
Kidney
- HUGE cysts with low epithelium (pressure atrophy) - Some kidney remnants in septa among cysts - Inflammatory infiltrate - Nephro & arteriosclerosis (increased BP) Etiology? |
Adult polycystic kidney disease / polycystosis
= Macrocystosis - Cysts may rupture & cause hematuria / retroperitoneal bleeding - Cysts grow slowly - destroy glomeruli - so filtrate is captured Etiology - AD hereditary disease, pathogenesis not known - 50% of nephrons affected |
|
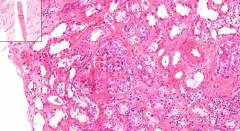
Kidney
- Proximal tubular cells destroyed & missing nuclei (dystrophic changes of different levels) - Granular cylinder casts in lumina of proximal tubules - Interstitial edema - Medullary hyperemia - Glomeruli intact Etiology? Pathogenesis? |
Acute tubular necrosis (ischemia)
= "shock kidney" Etiology - Hypovolemia Pathogenesis - Strong vasoconstriction - Ischemic necrosis of proximal tubule epithelium - Desquamation with Hb & myoglobin - Block distal & collecting tubules - Olig-/anuria Regeneration - 2-3 months - First polyuria due to nonfunctioning tubular cells - If BM damaged - no recovery |
|
Kidney
- Tubuli filled by leukocytes --> Destruction of tubules -----> Spread of inflammation to parenchyma - Small abscesses found, both medulla and cortex - Glomeruli intact, no abscess in them (contrary to hematogenous spread) Etiology? |
Acute pyelonephritis (pyelitis + nephritis)
Etiology - G- germs (e.coli) - Urine retention, VUR, DM (germs like glucose) |
|
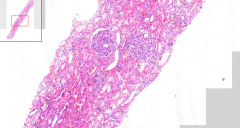
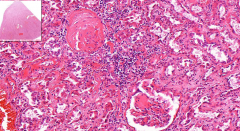
Kidney
- Enlarged glomeruli, filling up Bowman´s capsule - Feel like glomerular vessels are pushed through it, ooh - Edematous mesangium - RBC in tubuli Etiology? |
Acute postinfectious glomerulonephritis
= Poststreptococcal glomerulonephritis 1. Nephrotic syndrome 2. Nephritic syndrome Etiology - Part of RHEUMATIC FEVER - 7-14 days after b-hemolytic streptococcal infection - Immunity cross reaction - so NO bacteria! (autoimmune) - Immunecomplex deposition in glomerulus => Expansion of mesangium and endothelium EM/IHC must be done to see depositions |
|
Kidney
- Collapsed capillaries of glomeruli - Rounded fibroepithelial crescents in bowman´s space (pink, homogenous material) Etiology? What is a crescent? |
Rapidly progressive glomerulonephritis
= Crescentic glomerulonephritis Etiology - Antibodies against glomerular BM - Agressive enzymes from leukocytes & macrophages cause capillary holes and leakage of fibrin and blood cells - Renal failure in 1-3 months Fibroepithelial crescents = 'Half-moon' - Fibrin - Monocytes - Bowman´s capsule epithelial ells |
|
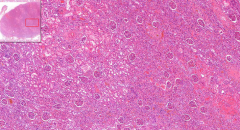
Kidney
- Most glomeruli sclerotic with hyaline targets - Those glomeruli has atrophic adjacent tubules - Healthy ones are compensatory hypertrophic = Macroscopic granulation - Scattered lymphocytes in interstitial tissue Etiology? |
Chronic sclerotic glomerulonephritis
= Group of inflammatory diseases ending with "end-stage" kidney Etiology - Usually starts with acute glomerulonephritis or some discrete changes |
|
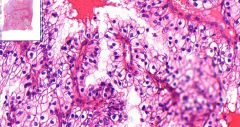
Kidney
- Hyaline nodules in mesangium (glomerulosclerosis) - Capillaries pushed out to bowman´s space - Some glomeruli are 100% hyalinized - Hyaline changes on vessels (arteriosclerosis) Etiology? What is sclerosis? Complications? |
Diabetic glomerulosclerosis
There are 4 forms of renal damage from diabetes: 1. Glomerular affection (glomerulosclerosis) - our slide 2. Renal vascular lesions (nephroslerosis) 3. Pyelonephritis with necrotizing papilitis 4. Glycogen and lipid accumulation in tubular epithelial cells (Armani cells) This is one of Prof. Steiner´s favorite topics These nodules are called Kimmelstein Wilson nodules Sclerosis = Hardening. - Increased amount of fibrillary material in interstitial tissue - Calcifications are results of these dystrophic changes NB! Slide is similar to amyloidosis. But amyloidosis does not form globules / nodules - and you can use different stain Complications - Podocytes are destroyed due to high glucose (they´re uptake is not insulin dependent) - So filtering holes are greatly enlarged => Nephrotic syndrome ==> Renal failure |
|
Kidney
- Solid growth pattern of tumor - Clear cells (cytoplasm w/ glycogen & lipids) - Low mitotic activity - 'Sarcomatoid transformation' = Small enlarged spindle cells - looking like sarcoma - Find focuses of bleeding & necrosis Etiology? What decides grading? Metastasis? |
Renal clear cell adenocarcinoma
= 'Grawitz carcinoma' Etiology - Malignant transformation of tubular epithelial cells - Elder patients - Male - Smoker Grading - Nuclei size & shape Metastasis? - Lymphatic / hematogenous - solitary - Brain & thyroid gland |
|
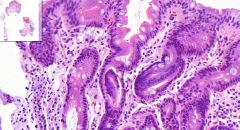
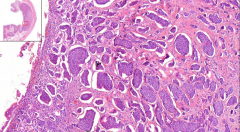
Stomach
- Lymphocytic infiltration - Intestinal metaplasia (goblet & paneth cells) - Atrophic glands - H.pylori on surface Etiology? Complications? |
Chronic gastritis
Etiology - H.pylori infection - Long term irritation - Autoimmune Intestinal metaplasia due to adaption of the chronic irritation Complications - Anemia - Stomach ulcer - MALT lymphoma |
|

Stomach
- Definite ulcer - Fibrolymphocytic membrane Etiology? Components of fibrolymphocytic membrane? Complications? Difference ulcer vs. erosion? |
Chronic peptic ulcer
Etiology - More or less same as gastritis - only chronic Fibrinolymphocytic membrane - Lymphocytes (chr) - Fibrin (fibrinoid necrosis) - Necrotic cells => Therefore it looks yellow macroscopically - Granulation tissue as a regeneration attempt Complications - Penetration to other organs - Perforation => Acute abdomen (death by peritoneal infection) Erosion = Eroded mucosa Ulcer = Eroded through muscularis mucosae |
|
Stomach
- THICK stomach submucosa (usually very thin) - A lot of fibrous tissue produced, no architecture - Among fibrous tissue we see 'signet ring cells' => Called 'desmophilic reaction' - High mitosis, nucleoli Etiology? Other names? Complications? 2 types of stomach cancers? |
Scirrhotic carcinoma of stomach
Etiology - Dietary realation, higher in Japan, spicy food Other name - Linitis plastica (due to leather-like wall) Complications - Metastasis - Krukenberg tumor - Virchov's node Stomach cancers 1. Intestinal type - cribriform pattern with glands 2. Poorly cohesive type (this type, diffuse, scirrhotic) |
|
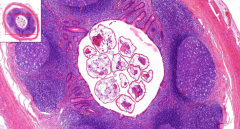
Appendix
- Parasites in lumen - No inflammation - Eosinophils in wall Etiology? |
Exyoriasis of appendix
= 'Oxyuris vermicularis' - pinworm Etiology - This worm. Often kids in kindergarden. - Anal itching - itch - eat - circle |
|
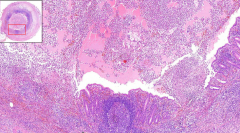
Appendix
- Discontinuous mucosa with ulcers - Thick submucosa - Leukocytic infiltration = cellulitis / phlegmone - Lumen filled by pus / fibrin = empyema Etiology? Complications? |
Acute / ulcerophlegmonous appendicitis
Etiology - Stagnation of stool etc. Complications - Perforation - Spread to other tissues = Periappendicitis |
|
Ileum
- Islands of trabecules of uniform cells - Normal nuclei with chromatin, low mitosis Etiology? Immunohistochemistry? Complications? Classification of neuroendocrine tumors? |
Carcinoid of small bowel
= A neuroendocrine tumor Etiology - Neuroendocrine argentaffin (?) cells Immunohistochemistry - Confirm diagnosis via argentaphinity and argentaphilia Complications - Fibroelastic changes of RA, since hormones go there Neuroendocrine tumor classification NET G1 - typical carcinoid = Benign NET G2 - atypical carcinoid = Intermediate NEC - large cell = Malignant NEC - small cell = Highly malignant (oat cell) |
|
Ileum
- Giant cell granulomas with no central necrosis - Ulcers & hyperemia of mucosa - Transmural mixed inflammatory infiltrate (ly, plasm) - Areas of scarring - Dysplastic changes = precancerous! Etiology? Complications? |
Chrohn disease
- Chronic discontinuous inflammation of GIT Etiology - Autoimmune reaction to something? ParaTB infection with genetic predisposition? (dark petra) Complications - Dysplastic, precancerous changes - Potential to develop amyloidosis |
|
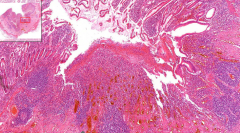
Liver biopsy
- Bluish areas of inflammation = portobiliar spaces - Small necrosis of hepatocytes = Piece-meal necrosis - Ground glass cells Diagnosis? Etiology? What is ground glass cells? What is piece-meal necrosis? What is portobiliar space? 2 types of chronic hepatitis? |
Chronic hepatitis
Etiology - HBV, HCV Ground glass cells: - Viruses infected with HBV Piece meal necrosis: - Isolated necrosis of 1 hepatocyte with lymphatic infiltrate around - and when many - large fibrosis and then liver cirrhosis occur Portobiliary space: - Portal triad + fibrous tissues 2 types chronic hepatitis 1. Minimal necrosis --> Healed 2. Active, chronic: More necrosis --> Goes to cirrhosis Gross liver is nodular due to fibrosis, and maybe brownish |
|
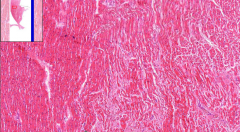
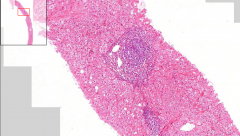
- Nice nodular liver parenchyma
- Remnant of septum in portobiliary space - Lots of vessels and fibrous strands with chronic inflammation - Architecture lost with fibrosis in spaces around ducts - Pseudo-ducts proliferation Diagnosis? Etiology? Complications? |
Liver cirrhosis
Etiology - many: Necrosis of hepatocytes - Toxic - Alcohol - Metabolic disorders (Wilson's disease) - Infections - Immune / unknown Complications - Portal hypertension - Liver failure - Malignancy --> Hepatocellular carcinoma May see the cause of liver cirrhosis in slide as well, this is shown here by ground glass cells I think, so it's a post-hepatic cirrhosis |
|
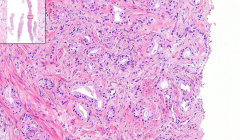
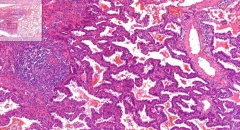
Prostate
- Fibromuscular stroma - Cribriform growth of glands - Invade prostatic capsule - Perineural spread Diagnosis? Etiology? Location? Gleason score? |
Prostatic carcinoma
Etiology - Malignancy of epithelial glands (adenocarcinoma) Location - Peripherally on the gland, unlike prostatic hyperplasia which is in central part Gleason score: - 1 to 5. Depends on type of growth of adenocarcinoma. Typical cribriform is 4, so 4+3 = 7 for example |
|
Supposed to look at testis:)
- No normal spermatic tubules - Germinal cells with clear cytoplasm, and this tumor you see fibrovascular septa with lymphocytes - Low mitotic activity Diagnosis? Tumor of which cells? Called what in females? |
Seminoma
Tumor of testicular germinal cells Called dysgerminoma in females |
|
Cervix of uterus
- Look at squamo-columnar junction - Tumor grows endophytic - High mitotic activity, hyperchromatic nuclei Diagnosis? Etiology? Macroscopically growth patterns? Complications? |
Squamous cell cervical carcinoma
Etiology - HPV 16,18,31,33 Macroscopically - Exophytic (cauliflower) - Ulcerative - Endophytic (this) Complications - Infiltrate deep cervix & uterus, and parametrial tissues around! 5% of HPV etiology also become adenocarcinoma |
|
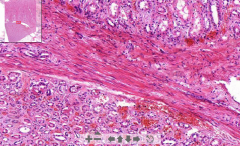
Intestine
- Endometrial tissue inside intestinal wall - Wall distended with fibrosis - Endometrial glands within muscular layer, but when you look closer you see they are normal, so no adenocarcinoma - Stroma around glands look like endometrial stroma! Diagnosis? Etiology? What is adenomyosis? What is chocolate cyst? |
Endometriosis of intestinal wall
= Presence of functional endometriual glands in abnormal location Etiology - Retrograde flow in menstruation - can occur anywhere in peritoneal cavity! - Trauma in sezarian section Adenomyosis - Nonfunctional endometrium in myometrium Chocolate cyst - Cyst filled with blood, which decompose to hemosiderin |
|

Ovary
- Very thick band of fibrous tissue on surface - Primordial follicles seen (normal) - Enlarged follicular cysts - NOT normal Diagnosis? Etiology? Complications? |
Polycystic ovaries
Etiology - Usually Stein-Leventhein syndrome Complications - Polycystosis, hirsutism, oligo/amenorrhea, infertility (thick tunica albuginea), no progesterone -> Obese & risk for endometrial hyperplasia due to too much estrogen --> So cause hormonal imbalances |
|
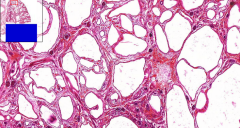
Ovary
- Loads of cysts - But look closer: There are tall columnar epithelium (coelomic) on base with mucin production Diagnosis? Etiology? What is coelomic epithelium? 2 types of epithelioid stromal tumors? (most common of ovaries) |
Mucinous cystadenoma of ovary - very frequent
Etiology - Intraction of this endocervical ep to ovaries Coelomic ep - Epithelium that lines the inner body cavities Epitheloid stromal tumors 1. Serous - cylindrical with cilia 2. Mucinous - cylindrical/cuboidal with pale cytoplasm, nuclei in base |
|
Breast
- Massive fibrosis - Large and small cysts (of ducts) - Apocrine metaplasia: Inner lining of cyst (snouts) - Secretion of some proteinaceous material (milk) but low amount - the gland is not lactating - May see scarring, cysts and calcifications Etiology? Age groups? Dangers of epithelial changes? |
Fibrocystic changes of breast
Etiology - Hormonal imbalance, of increased estrogen and lower or no counteracting progesterone Occurs in young women Ductal epithelial changes: - Typical hyperplasia = benign - Atypical hyperplasia = precancerous |
|
Breast
- Violet area = tumor - Form ducts with cribriform pattern - May form islands (solid type) - cohesive Risk factors? Macro? Micro types of this? Metastasis? Treatment? Carcinoma in situ lesions? |
Ductal adenocarcinoma of breast
- most ocmmon female tumor (100:1 F:M) Risk factors - Family history (BRCA) - Precancerous breast changes (atypical lobular / ductal hyperplasia) - Cancer in contralateral breast - Duration of hormonal activity - Obesity (since hormonal activity last longer when it's stored in fat) Macro - Uneaven, stone hard nodule - May retract nipple & peau d'orange Micro-types 1. Ductal carcinoma (80%) 2. Lobular carcinoma (8%) Metastasis - Sentinel lymph node (check with technesium (drained by lymph) to see which is sentinel Treatment - It is hormone dependent, so can block hormones - Biological therapy for HER 2 receptors Carcinoma in situ lesions 1. Ductal CIS (our slide) - Monoclonal proliferation (solid or cribriform) - Comedo necrosis in middle - Cohesive 2. Lobular CIS - Smaller, non-cohesive (loss of E-cadherin) - Line up in 'indian files' or 'duck-lines' - Desmophilic stroma like ad.ca of stomach |
|
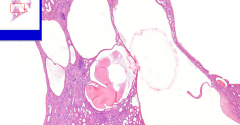
- A tube with an embryo inside
- Blood coagulum with chorionic vili = Myxoid stroma, cytotrophoblasts, syncytiotrophoblast - Tubular epithelium should have decidual change (not sure if our slide has) = Large cells with eosinophilic cytoplasm Etiology? Complications? |
Ectopic pregnancy - here of uterine tube
Etiology - Chronic inflammation (any) lead to scarring of tube and thus ectopic pregnancy Complications - Trophoblasts grow into tube to create "placenta" - will lead to massive bleeding and rupture (abort child) - HCG hormone increase - Very rarely it may reimplant in abdominal cavity…. |
|
- See a whole mess of hemorrhagic material
1. Blood with chorionic villi of the 2 types of trophoblasts (upper right) = decidual change 2. Larger endometrial glans + stroma arranged in fascicular pattern Etiology? Complications? |
Miniinterruption of pregnancy
1. Own wish 2. Miscarriage (curretage cleans the uterine cavity and this is the result) We (pathologists) need to check it since if there is decidua but NOT trophoblasts - this means it is ectopic pregnancy, and clinician must go hunting. - HCG should go down to normal within 14 days, if not it may be ectopic or some HCG producing tumor Complications - Source of endometriosis (rare) - Ectopic pregnancy |
|
- Collapsed lung (see:bronchioles & no air in alveoli)
- Stellate bronchioles - Squamous scale material in bronchi Etiology? What is content of amniotic fluid? |
Aspiration of amniotic fluid by fetus
Etiology - Squeezing of umbilical cord - leading to hypoxy of baby. This irritates breathing center, which activates respiratory reflex, and aspiration of fluid is done. Content - Desquamated skin - Hair - Metabolic derivatives (pee) This is all the time drunken by baby and peed out. - May also see meconium, since - like in any hypoxia/strangulation - one of the reflexes is defecation |
|
- Large chorionic villi with extreme stromal edema
- Avascular - Lined by proliferating trophoblasts - Some fjor-like invaginations - Circumferential proliferation of syncytiotrophoblasts Etiology? Grossly? 2 types of moles? Complications? |
Hydatidose mole
Etiology - Part of gestational trophoblastic diseases Macro - Huge grape-like chorionic villi, filling up the whole uterine cavity - Increased HCG and size of uterus compared to normal gestational age! Types of moles 1. Complete - No fetus (empty egg fertilized by 1diploid or 2 haploid sperms) - So chromosomal material is 46 XX / XY - No fetus persent 2. Partial - Normal haploid egg, fertilized by 1 diploid or 2 haploid sperms - So chromosomal material is 69 XXX / XXY - May see parts of fetus Complications - Always ends with miscarriage - Increased risk of choriocarcinoma |
|
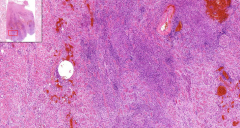
- Very hemorrhagic (red)
- Tumor (blue) inside = large cytoplasm cells = decidual change - Pleomorphic cells (look closer) - Areas of necrosis - See smooth muscle cells of myometrium of uterus! This may be a difficult slide from our slide box.. Look for tumors around in smooth muscle… Necrosis and pleomorphic cells Etiology? Risk factors? Complications? Treatment? |
Choriocarcinoma of uterus
= malignant tumor of trophoblasts, with tendency to necrotize and metastasize hematogenously early (since it's tries to make placenta = lots of vessels) Risk factors - Complete (invasive) hydatiform mole Complications - early metastasis - Local destruction of uterus and parametria Treatment - Very sensitive to chemotherapy, even with distant spreads like to the brain! Woho :D |
|
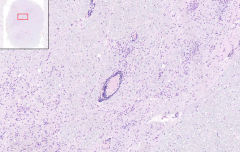
Brain
- Dilated spaces between meninges (normally very narrow) (Pia mater <--> arachnoid) - Dilated vessels + neutrophils around - Sharp edge from inflamm --> No brain parenchyma infiltrate Etiology? Ways of spread of bacteria? Grossly? |
Acute purulent meningitis of leptomeninges
Etiology - Bacteria o Meningococcus (Neisseria meningitidis) o Pneumococcus (Streptococcus pneumoniae) o H. Influenzae in children o E.coli Nb! H.Influenza vaccination was earlier the cause of the kid meningitis!! Just 5 years ago they got new vaccine. Ways of spread: - Hematogenous (sepsis) - Otogenic (chr. mid.ear. inflamm) - Open trauma of head (any small connection) - Retrograde in veins (facial, jugular) Grossly - Swollen brain - Hyperemic, non-glossy surface - Pus accumulates in sulci of brain ! Possible with spread along brain vessels --> Meningoencephalitis |
|

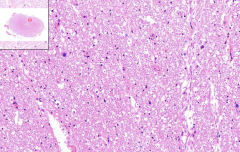
Brain
- See ducts of sylvius (on bottom) - Pinkish color is fibrinous exudation (with fibers!) - See lymphocytes & histiocytes = Orth cells - See Langhans cells => TBC! - Maybe we see caseous necrosis, maybe not Etiology? Grossly? Synonym? What can it be misdiagnosed with in CSF LM? |
TBC purulent leptomeningitis
Etiology - Hematogenous spread from primary TBC focus Grossly - Exudative - white/green gelatinous layer of base - Thick, white nodules on base Synonym = Basal meningitis CSF microscopy - may be misdiagnosed with treponema pallidum and neurosyphilis - So today we use more commonly PCR - takes hours - while culturing takes 6-8 weeks. |
|
Brain
- Spine cross section - Grey horn of anterior root: o Hypercellular (triangular bluish cells) o Lymphocytes around vessels o Loss of Nissl substance in motor neuron (Tigrolysis) o Necrosis of ganglial cells => Perivascular lympchocytic infiltrate o Accumulation of microglial cells Etiology? Macro? What is tigrolysis? What is the function of microglial cells here? |
Poliomyelitis / tick-bite encephalitis of SC
=> Both have similar LM picture Etiology - Viral brain inflammation (polio is transferred by water) Macro - Brain and spine edema Tigrolysis - That first of all dissapears the Nissl substance (ER) of cells - so all the cellular organelles that require energy dies off first. Later - the nuclei - since somehow the cell can preserve the most important part (nucleus) Microglial cells - Work like inflammatory-like cells for: o Phagocytosis o Walling-off the area |
|
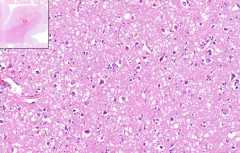
Brain
- Whitish spots - is the loss of myelin sheaths - Myelin is pinkish - since they are proteins Macro? Etiology? What can you stain myelin with? Where is the highest loss of myelin? What is the typical course? What is the cause of death? |
Multiple sclerosis
=> A autoimmune (maybe viral cross reaction) demyelination disorder Macro: seen as white plaques Myelin stain - Luxol blue Highest loss - Below ependymal layer of brain ventricles Typical course - Worsening -- bettering -- worsening and gradually worse and worse Cause of death - Stop of breathing due to failure of respiratory muscles leading to aspiration or pneumonia - or just stop of breathing |
|
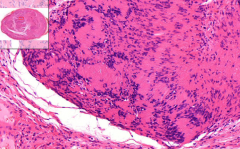
Some oval, demarcated round lesion with capsule
- Hypo- and hypercellular areas (what are they called?) - Hypercellular areas arranged in palicading / radial structure - Spindle cells with light eosinophilic cytoplasm - No neurons What is it? What is the areas called? What are the special bodies in hypercellular areas called? |
Neurinoma / Schwannoma
- origins from Schwann cells - Grow from peripheral nerve sheaths - but grow as a nodule and not into the nerve - so easy to excise. Areas - Antoni A = Hypercellular (palicading structure) - Antoni B = Hypocellular They are called "Verocay bodies" NO other tumor has this organization! It is a biopsy - nerve is not here. |
|
- Just see a whole bunch of random stuff
- Small cells with spindle shaped nuclei - Whirlpool organization - or in rounded onion globules… - Central of onion is often necrosis - and there may be secondary calcifications = What is this called? What is it? Where does it usually affect? Grossly? Complications? What are the calcified onions called? |
Meningeoma
- A benign tumor of the leptomeninges Usually affect - Frontal skull areas - maybe because there are progesterone receptors? More women than men have this tumor Grossly: - Hyperkeratosis of the adjacent bone (may grow inwards in a wavy fashion) - If it is flat (meningioma en plaque) it's a big problem with surgical removal & recurrence Complications - Pressure of adjacent brain tissue => Epilepsy Calcified onions = Psammoma bodies |
|
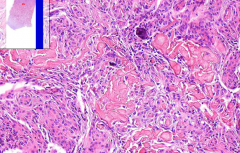
Brain
- Pleomorphism, mitotic activity, nucleoli - See some necrotic areas - Loads of vessels! - high cellularity - Maybe hemosiderin deposits - after bleeding What is it? Complications & prognosis? What is normally mitotic index of brain tissue? What are the CNS tumors of the astroglial cells - and which develop to this? |
Multiform glioblastoma - malignant
- Affect older people supratentorial (frontoparietal) Complications - Highly invasive - it has no capsule - So more or less impossible to resect without recurrences - 20% live 2 years Normal mitotic index should be 5% of glial tissue - Here it is maybe 50% (and hematology = 90%) CNS glial tumors cells: - Astroglioma o Low grade o High grade ==> Glioblastoma! |
|
Brain
- Lots of vesicles and spaces = Spongiform architecture - Loss of brain matter - Loss of neurons - but no inflammatory reaction Etiology? Grossly? Clinically? Other diseases caused by same problem? |
Creutzfeldt-Jacob disease
= Subacute spongiform encephalopathy The brain looks exactly the same in autopsy - due to autolysis and reaction with water Etiology - Small abnormal proteins (prions) cause CNS damage and also damage other proteins Grossly - You don't see nada, maybe brain atrophy Clinically - Progressive dementia Other diseases by prions: - Kuro - Scrapie?? - Mad cow They are all in the prion-disease group! |
|
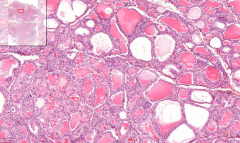
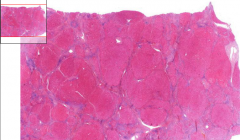
Thyroid gland
- High columnar epithelium - Light thin colloid with marginal 'usuration' - Interstitial lymphoplasmocytar infiltration Etiology? Predispositions? TSI / TGI? Clinically? |
Graves-Basedows disease (toxic goiter)
Etiology - Autoimmune process with Ab against TSH receptors - with STIMULATING activity: o TSI = Thyroid stimulating immunoglobulins - hyperfunction of follicular cells o TGI = Thyroid growth stimulating immunoglobulins - hyperplasia of follicular cells Predispositions - Female (10:1) - Familiar: HLA-DR3 antigen association Clinically - Exopthalmus - Struma vibrans - Pulsans et fremens |
|
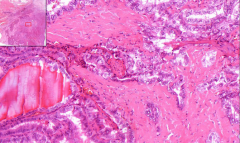
Thyroid gland
- Ground glass nuclei - with deep intranuclear grooves - True papilles seen (with fibrovascular stroma - like in papilloma) - Small calcifications --> Psammomatous bodies Etiology? Risk factors? Radio-imaging? Diagnosis? Prognosis? |
Papillary carcinoma of thyroid gland
- Most common thyroid malignant tumor Etiology - Ionizing radiation (Hiroshima, Nagasaki, Cernobyl) Risk factors - Young female Radio imaging - Cold nodule Diagnosis - FNAC Prognosis - Good |
|
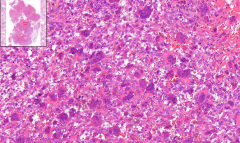
Don't really see which tissue we're at - but 2 main components:
1) Giant multinucleated cells of osteoclast character 2) Mononuclear round or spindle shaped cells Etiology? Location? Macro? X-ray picture? What are the mononuclear round cells? |
Giant cell tumor of bone = osteoclastoma = brown tumor of bone
Location - Epiphyseal areas of long bones Macro - Excentrically localized lytic lesion of bone - Highly vascularized with hemorrhagic focuses (brown) and cystic degeneration X-ray - Cluster of soap bubbles, it looks like |
|
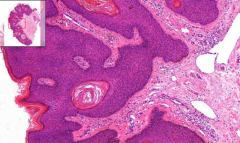
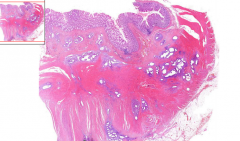
Some exophytic skin growth
- Hyperplasia of dermis: o Acanthosis o Papillomatosis o Hyperkeratosis o Parakeratosis - Horny globules (or horny balls as Prof. Steiner said…) trapped in hyperplastic epidermis - Hyperpigmentation of epidermal basal layer Grossly? Malignancy? |
Seborrhoic keratosis
= Senile keratosis Grossly - Exophytic verrucous growth / protuberance - Waxy appearance - Hyperkeratosis & hyperpigmentation Malignancy - Borderline lesion between hyperplasia & benign tumor (squamous papilloma) |
|
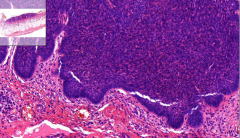
Looking at skin
- Nests of dark cells in base of epidermal layer - Irregular organization - Central parts maybe necrosis & cystic change Etiology? Grossly? Ulcus rodens? Complications? |
Basalioma
= Epidermal basal cell carcinoma Etiology - Elderly patients at areas with long lasting sun exposure Grossly - Slow growing papule with central ulcer / excavation - Edges are elevated (looks rolled) => Ulcus rodens Complications - No metastasis, but aggressive growth |
|
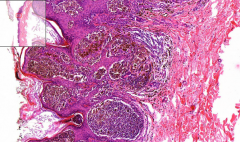
Looking at skin
- Nests of tumoral cells growing in nodular pattern - Variant amounts of melanin - High nuclear pleomorphism and mitotic activity - Chronic lymphocytic infiltration in adjacent tissue Etiology? Grossly? How does tumor cells migrate? Complications? |
Malignant melanoma
= Tumor of melanocytes - Skin, pigmented mucosal tissues, eye, meninges… Etiology - Transformation of pigmented nevus - UV radiation Grossly - Unevenly pigmented macule - No sharp margine - Ulceration and bleeding Migration of tumor cells 1. Start in epidermis 2. Invade deep dermis, subcutaneous fat (always) 3. In FOCUS EPIDERMOTROPISM (pagetoid spread) - there is also cellular penetration into epidermis Complications - late metastasis (>10 years after primary tumor) |