![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
151 Cards in this Set
- Front
- Back
|
Congenital Abnormalities of the esophagus present after birth with |
regurgitation during feeding |
|
|
Esophageal ____________ is associated with congenital heart defects, genitourinary malformations and neurological disorders |
Atresia |
|
|
Portion of the esophageal conduit is replaced by a thin, noncanalized cord with blind pouches above and below the segment |
esophageal atresia |
|
|
_________ is the most common form of congenital intestinal atresia caused by failure of the cloacal membrane to involute |
Imperforate anus |
|
|
Connection between the esophagus and trachea/mainstream bronchus that allows swallowed material or gastric fluids to enter the respiratory tract |
Fistula |
|
|
Incompletem of atresia |
Stenosis - lumen is reduced by a fibrous thickened wall - can be congenital or from inflammatory scarring (GERD) |
|
|
Cystic masses with redundant smooth muscle layers that can occur throughout the GI tract |
Congenital duplication cysts |
|
|
Occurs when incomplete formation of the diaphragm allows cephalad displacement of abdominal viscera |
Diaphragmatic hernia - when hernia is substantial, pulmonary hypoplasia incompatible with life |
|
|
Occurs when abdominal musculature is incomplete and the viscera herniate into the ventral membranous sac |
Omphalocele - 40% are associated with other birth defects |
|
|
Similar to omphalocele except that all layers of the abdominal wall from skin to peritoneum fail to develop |
Gastroschisis |
|
|
Most common site for gastric mucosa ectopia |
proximal esophagus (inlet patch) - dysphagia and esophagitis Can also occur in the small bowel or colon presenting with occult blood loss or peptic ulceration |
|
|
Pancreatic heterotropia occurs most commonly in the __________ |
stomach pylora and esophagus - inflammation, scarring, and obstruction |
|
|
Blind pouch leading off the alimentary tract, lined by mucosa and includes all three layers of the bowel wall (mucosa, submucosa, muscularis propria) |
True diverticulum |
|
|
Results from persistence of the vitelline duct (connecting yolk sac and gut lumen) leaving a solitary outpouching within 85cm of ileocecal valve |
Meckel Diverticulum
- male to female ratio 2:1 - heterotropic gastric/pancreatic tissue can be present causing ulceration (gastric tissue) |
|
|
Stenosis assoicated with Complex polygenic inheritance, Turners syndrome, and trisomy 18 |
Congenital hypertrophic pyloric stenosis - common, male 4x female - regurgitation and projectile vomiting within 3 weeks of birth - externally visible peristalsis and palpable firm ovoid mass Tx - full thickness muscle splitting (myotomy) |
|
|
___________ is a complication of chronic antral gastritis, peptic ulcers close to the pylorus, and malignancy |
acquired pyloric stenosis |
|
|
Results from arrested migration of neural crest cells into the gut, yielding an aganglionic segment lacking peristaltic contractions |
Hirschsprung disease or congenital aganglionic megacolon - functional obstruction and progressive dilation/hypertrophy of unaffected proximal colon - 1 in 5000 births - Rectum ALWAYS effected |
|
|
Heterozygous loss of ____________ accounts for 15% of sporadic cases and majority of familial cases of Hirschsprung disease |
RET tyrosine kinase receptor - penetrance is incomplete - influenced by sex linked factors (males 4x more common) - Genetic and environmental modifiers |
|
|
Hirschsprung disease manifestations |
- Neonatal failure to pass meconium - abdominal distention with severely distended megacolon - patient's risk perforation, sepsis, enterocolitis, sepsis, or enterocolitis with fluid derangement |
|
|
Difficulty swallowing |
dysphagia |
|
|
Short or long lived muscle contraction of esophagus |
spasm |
|
|
causes functional obstruction of esophagus and increased wall stress can cause diverticula to form |
diffuse esophageal spasm |
|
|
_____________ can contain one or more layers and if sufficiently large, they can accumulate enough food to present as a mass with food regurgitation |
Esophageal diverticula |
|
|
_______________ occurs immediately above the upper esophageal sphincter |
Zenker (pharyngoesophageal) diverticulum |
|
|
_____________ occurs at the esophageal midpoint |
Traction diverticulum |
|
|
________________ occurs immediately above the lower esophageal sphincter |
Epiphrenic diverticulum ZTE |
|
|
Ledgelike protrusions of fibrovascular tissue and overlying epithelium |
Mucosal webs - most common in upper esophagus - women over 40 |
|
|
A constellation of mucosal webs, iron deficiency anemia, glossitis, and cheilosis |
Plummer Vinson syndrome - Patterson brown kelly syndrome |
|
|
Similar to mucosal webs but are circumferential and thicker that include the mucosa, submucosa, and occasionally hypertrophic muscularis mucosa |
Esophageal rings |
|
|
Esophageal rings located above the gastroesophageal junction |
A rings - squamous epithelium |
|
|
Esophageal rings located at the squamocolumnar junction |
B rings - gastric cardia type mucosa |
|
|
Triad of incomplete relaxation of the LES, increased LES tone, and esophageal peristalsis |
Achalasia |
|
|
_________ achalasia is idiopathic and results from failure of distal esophageal neurons to induce LES relaxation during swallowing (NOS and VIP signaling) |
Primary achalasia |
|
|
Acquired megalocolon can occur in |
Chagas disease, bowel obstruction, inflammatory bowel disease, psychosomatic disorders Only in CHAGAS are ganglia actually lost |
|
|
Secondary achalasia causes |
T cruzi - Chagas disease Disorders of the vagal dorsal motor nuclei (polio) Diabetic autonomic neuropathy Infiltrative disorders Tx - myotomy, balloon dilation, and or botulinum toxin injection to inhibit LES cholinergic neurons |
|
|
Longitudinal laceration of the Gastroesophageal junction associated with excessive vomiting, often in the setting of alcohol intoxication |
Mallory-Weis tears - reflex relaxation of LES fails in prolonged vomiting resulting in esophageal stretching and tearing - hemoptysis |
|
|
Agents that cause damage to esophageal squamous epithelium |
Alcohol, corrosive acids/alkalis, excessively hot fluids, and heavy smoking Pills that lodge in the throat and dissolve can cause esophagitis Irradiation, chemotherapy or GVHD |
|
|
Esophagus can also be involved in systemic desquamative disorders such as |
pemphigoid epidermolysis bullosa Crohns disease |
|
|
Esophageal infections of immunocompromised patients |
HSV, CMV, candida - pain and dysphagia are the chief symptoms in severe and/or chronic cases, hemorrhagic, stricture, or perforation can result |
|
|
What is the most common inflammatory response in the esophagus? |
Dense neutrophilic infiltrate - may not occur in chemical necrosis w/o inflammation |
|
|
Any epithelial ulceration is accompanied by ____________ and eventual fibrosis |
granulation tissue |
|
|
_________, when severe, is associated with adherent grey-white pseudomembranes composed of densely matted fungal hyphae and inflammatory cells |
Candidiasis |
|
|
Infection that causes punched out ulcers |
Herpes viruses |
|
|
Shallow ulcerations with viral inclusions |
CMV |
|
|
Lesions associated with esophageal GVHD or blistering disorders resemble ______________ |
counterparts for skin |
|
|
___________ is the most common cause of GERD |
Reflux of gastric contents - major source of mucosal injury - duodenal bile reflux can exacerbate injury |
|
|
What causes Gastric reflux? |
decreased LES tone - exacerbated by alcohol, tobacco, obesity, CNS depressants, pregnancy, delayed gastric emptying, increased gastric volume |
|
|
___________ is also a cause of GERD and occurs when the diaphragmatic crura are separated and the stomach protrudes into the thorax |
Hiatal hernia |
|
|
Morphology of GERD |
Hyperemia and edema Basal zone hyperplasia and thinning of superficial layers Neutrophil and/or eosinophil infiltration |
|
|
GERD is common in adults over age ________ |
40 |
|
|
Symptoms of GERD |
dysphagia, heartburn, regurgitation of gastric contents into mouth Relief with proton pump inhibitors or H2 histamine receptor antagonists |
|
|
Complications of chronic GERD |
Ulceration, hematemesis, melena, stricutre or Barretts esophagus |
|
|
Adults present with food impaction and dysphagia while children present with feeding intolerance and GERD like symptoms |
Eosinophilic esophagitis - Cardinal histological feature is large numbers of intraepithelial eosinophils - Patients have one or more atopic disorders (atopic dermatitis, asthma) - Tx = dietary restriction, steroids |
|
|
Complication of GERD characterized by intestinal metaplasia within the esophageal squamous mucosa |
Barrett's esophagus - white male between 40-60 with chronic GERD - increased risk of esophageal adenocarcinoma - pre-invasive dysplasia |
|
|
Grossly, Barrett's esophagus presents as |
patches of red, velvety mucosa extending up from the gastroesophageal junction |
|
|
Microscopically, Barrett's esophagus looks like |
Intestinal columnar epithelium, particularly mucin secreting goblet cells Dysplasia is classified as low or high grade Intramucosal adenocarcinoma is characterized by neoplastic cell invasion into lamina propria |
|
|
Dx of Barretts |
Both gross and microscopic findings - periodic endoscopy done for surveillance - Multifocal high grade dysplasia or carcinoma typically requires esophagectomy but laser ablation may be used |
|
|
_____________ are caused by severe portal hypertension inducing collateral bypass channels between portal and caval circulations |
Esophageal varices - dilated subepithelial and submucal veins in distal esophagus - alcoholic cirrhosis is number one cause - hepatic schistosomiasis is second most common |
|
|
Esophageal varices morphology |
tortuous dilated veins in distal esophagus/proximal gastric submucosa irregular luminal protrusion of overlying mucosa with superficial ulceration, inflammation, or adherent blood clots |
|
|
Clinical features of Esophageal varices |
Clinically silent til rupture caused by - inflammatory erosion - increased venous pressure - increased hydrostatic pressure/vomiting Tx - sclerotherapy/balloon tamponade/ligation 50% die during first bleed, survivors usually die within a year |
|
|
______________ evolve from dysplastic changes in Barrett's esophagus |
Esophageal adenocarcinoma - white men - half of all esophageal cancers |
|
|
Oncogensis from Barrett's esophagus to esophageal adenocarcinoma |
Chromosomal and p53 abnormalities Amplification of c-ERB-B2 and cyclin D1/E Mutations in Rb and p16/INK4a cyclin dependent kinase inhibitor |
|
|
Esophageal adenocarcinoma Gross |
Exophytic nodules to excavated infiltrative masses in distal third of esophagus |
|
|
Esophageal adenocarcinoma micro |
Produce mucin and form glands (Adeno) Intestinal type morphology Diffusely infiltrative signet ring tumors LESS common and rarely adenosquamous or poorly differentiated cells |
|
|
Esophageal adenocarcinomas typically present with |
dysphagia, weight loss, hematemesis, chest pain, or vomiting Detected late, 5 year survival is poor |
|
|
Esophageal Squamous cell carcinoma epidemiology |
Older than 45, black male alcohol, tobacco, caustic esophageal injury, achalasia, Plummer Vinson syndrome, scalding hot beverages |
|
|
Most common causes of esophageal squamous cell carcinoma in US |
alcohol and tobacco Contributing factors - nutritional deficiencies and diet of PC hydrocarbons, nitrosamines - HPV |
|
|
Half of all esophageal squamous cell cancers occur in the _____________ of the esophagus |
middle third
|
|
|
Morphologic progression of Esophageal SCC |
In situ gray white, plaque like mucosal thickenings Expand as exophytic lesions, ulcerate, or become diffusely infiltrative with wall thickening/luminal stenosis Rich submucosal lymphatic network promotes circumferential longitudinal spread into adjacent mediatstinal structures Moderately to well differentiated |
|
|
Clinical features of ESCC |
Onset of symptoms late - dysphagia, obstruction, weight loss, hemorrhage, sepsis secondary to ulceration, or respiratory fistula with ulceration |
|
|
Benign tumors of the esophagus are usually __________ in origin with leiomyomas being most common |
Mesenchymal Followed by fibromas, lipomas, hemangiomas, neurofibromas, lymphangiomas |
|
|
Benign tumors can also take the form of mucosal polyps due to |
- Fibrovascular polyps - Pedunculated lipomas - Squamous papillomas - HPV associated condylomas |
|
|
Masses of granulation tissue in the esophagus can grow as ____________ or ____________ |
inflammatory polyps invasive inflammatory pseudotumors |
|
|
Transient mucosal inflammatory process that can be asymptomatic or cause varying degrees of pain, nausea, vomiting |
Acute gastritis - severe cases exhibit ulceration with hemorrhage presenting as hematemesis or melena - occurs when one or more mechanisms that protect gastric mucosa from acidic environment are overwhelmed |
|
|
Pathogenesis of acute gastritis |
- increased acid production w/ back diffusion - decreased bicarbonate - mucin production - direct mucosal damage - NSAIDs reduce bicarb and interferes with the cytoprotective actions of prostaglandins |
|
|
What are the protective effects of prostaglandins? |
Inhibit acid production promote mucin synthesis increase vascular perfusion |
|
|
Acute Gastritis morphology |
Gross - edema/hyperemia (hemorrhage) Micro - neutrophils invade gastric epithelium with superficial erosion and fibrous luminal exudate |
|
|
Focal, acute gastric mucosal defects that occur as a complication of NSAID use or as a consequence of severe stress |
Acute gastric ulceration - systemic acidosis, hypoxia, and reduced splanchnic flow |
|
|
________ ulcers occur after shock, sepsis, and severe trauma |
stress ulcers |
|
|
__________ ulcers occur in the proximal duodenum and are associated with burns or trauma |
Curling ulcers **burning that midnight oil, curling iron dude** |
|
|
__________ ulcers are gastric, duodenal, and esophageal ulcers arising in patients with intracranial disease that have a high risk of perforation |
Cushing ulcers Cushing disease results from INTARCRANIAL problems same as cushing ulcers |
|
|
Brain injuries can lead to increased __________ stimulation causing gastric acid hypersecretion
|
vagal stimulation |
|
|
Ulcer morphology |
shallow, less than 1 cm in diameter ulcer base brown w/ adjacent mucosa normal |
|
|
Defensive forces of stomach mucosa |
- Surface mucous secretion - Bicarb secretion - Mucosal blood flow - Apical surface membrane transport - Epithelial regenerative capacity - Elaboration of prostaglandins |
|
|
Injury to gastric epithelium includes |
- H pylori - NSAID - Aspirin - Cigarettes - Alcohol - Gastric hyperactivity - Duodenal gastric reflux |
|
|
Critical ill patients with gastric mucosal injury |
bleeding, blood loss requiring transfusion, perforation After removing of injurious stimulus, healing with complete re-epithelialization is the norm |
|
|
Single most important determinant of outcome is the ability to ___________________ |
correct the underlying conditions |
|
|
_____________ is characterized by ongoing mucosal inflammation with mucosal atrophy |
Chronic gastritis - substrate in which dysplasia and carcinoma can arise |
|
|
Most common cause of chronic gastritis |
H pylori - fecal-oral, oral-oral, environmental routes - lower SES |
|
|
H pylori induce predominantly _________ gastritis |
antral - increased acid production and disruption of normal mucosal protection mechanisms |
|
|
H Pylori virulence factors |
Motility via flagella Urease production buffering gastric acid Bacterial adhesins to bind surface epithelial cells Toxins - cagA and vacA |
|
|
Initial antral gastritis progresses to __________ |
multifocal atrophic gastritis & intestinal metaplasia - mucosal atrophy with reduced acid production - polymorphisms in IL-B and TNF genes correlate with the development of chronic disease |
|
|
H pylori infected mucosa is _________ |
erythematous to coarse/nodular H pylori organisms are found in the antrum in the superficial mucus and overlying surface and neck epithelium Luminal/epithelial neutrophil - pit abscesses Lamina propria contains plasma cells, macrophages, and lymphocytes |
|
|
Long standing gastritis is associated with |
diffuse mucosal atrophy prominent lymphoid aggregates |
|
|
H pylori Dx |
Serologic test, urea breath test, bacterial culture, direct bacterial visualization in gastric biopsy, DNA based tests |
|
|
_________ gastritis typically spares the antrum and is associated with hypergastrinemia |
Autoimmune gastritis - CD4 T cell mediated autoimmune destruction of parietal cells - gastric secreted antibodies to parietal cells and intrinsic factor - Parietal cell cytotoxicity leads to defective gastric acid secretion that triggers hypergastrinemia and antral G cell hyperplasia - Reduced intrinsic factor leads to B12 deficiency causing pernicious anemia - Damage to chief cells causes pepsinogen loss |
|
|
Immune gastritis morphology |
Rugal folds are lost diffuse mucosal damage leading to damage of parietal cells in body/fundus Lymphocytic infiltrates with macrophages and plasma cells |
|
|
Classical picture of autoimmune gastritis |
Antibodies, gastric atrophy, Pernicious anemia b12 deficiency can also lead to - atrophic glossitis, malabsorption, and peripheral neuropathy/CNS lesions associated with other autoimmune disorders |
|
|
Group of disorders marked by edema, glandular hyperplasia, and regenerative changes due to an injury via NSAID use or bile reflux |
Reactive gastropathy |
|
|
Characterized by heavy eosinophlic infiltration of the mucosa or submucosa via allergies, infection, or systemic collagen vascular disorder |
Eosinophilic gastritis |
|
|
Idiopathic disorder predominantly affecting women with 40% marked by celiac disease and an accumulation of intraepithelial CD8 T cells |
Lymphocytic gastritis |
|
|
Diverse group of diseases sharing the presence of granulomas, sarcoid, crohn disease, and other causes |
Granulomatous gastritis |
|
|
What typically occurs in the first portion of the duodenum or antrum? |
Peptic ulcer disease - most commonly due to H pylor induced hyperchloridic chronic gastritis and NSAID use |
|
|
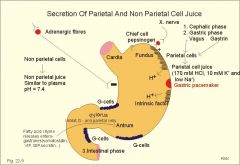
MOA of how H pylori induced acid secretion |
The inflammatory response caused by bacteria colonizing near the pyloric antrum induces G cells in the antrum to secrete the hormone gastrin, which travels through the bloodstream to parietal cells in the fundus. Gastrin stimulates the parietal cells to secrete more acid into the stomach lumen, and over time increases the number of parietal cells, as well.[40] The increased acid load damages the duodenum, which may eventually result in ulcers forming in the duodenum.
|
|
|
Causes of hyperacidity in PUD |
Infections parietal cell hyperplasia excessive secretory response increased gastrin production NSAIDs and steroids block the normal prostaglandin cytoprotective effects and cigarette smoking impairs mucosal blood flow and healing |
|
|
Most ulcers are __________ |
solitary - sharply punched out defect - clean ulcer bases - thin layers fibrinoid tissue merging with granulomatous tissue - surrounding mucosa exhibits chronic gastritis |
|
|
PUD presents with |
epigastric gnawing, burning or aching pain worse at night Nausea, vomiting, bloating belching and weight loss Complications - anemia, hemorrhage, perforation, and obstruction |
|
|
Long standing chronic gastritis exposes epithelium to inflammation related free radical damage and proliferative stimuli leading to _____________ |
in situ lesions as dysplasia
|
|
|
Excessive growth factor in rugal fold epithelial cells that leads to |
giant enlargement of rugal folds - hypertrophic gastropathies - excessive growth factor production |
|
|
Diffuse foveolar cell hyperplasia, with a protein losing enteropathy that causes hypoproteinemia due to an overexpression of TGF-alpha |
Menetrier disease - risk of gastric adenocarcinoma is increased |
|
|
Gastrin secreting tumors typically in the small bowel or pancreas |
Zollinger Ellison syndrome - multiple duodenal ulcers and chronic diarrhea - elevated gastrin levels - increased parietal cells - 60-90% of gastrinomas are malignant |
|
|
Nodules or masses that project above the level of the surrounding mucosa resulting from epithelial hyperplasia, inflammation, ectopia, or neoplasia |
Polyps |
|
|
_________ constitute 75% of gastric polyps |
Hyperplastic/inflammatory polyps - ages 50-60 - chronic gastritis - less than 1 cm and multiple - irregular, cystically dilated and elongated glands with variable inflammation |
|
|
__________ polyps occur sporadically in women over 50 or in familial adematous polyposis |
Fundic gland polyps - increased by PPI and increased gastrin - smooth, well circumscribed lesions with little inflammation |
|
|
Gastric adenomas comprise ______ of gastric polyps |
10% - FAP or chronic gastritis w/ atrophy - usually solitary and less than 2 cm - over 2 cm resect, could have carcinoma |
|
|
_______________ constitute more than 90% of gastric malignancies and are divided into intestinal and diffuse forms |
Adenocarcinomas - H pylori increases risk - increased consumption of N-nitroso compounds, benzopyrene in food preservation - reduced risk with increased fruits and leefy green veggies Partial gastrectomy increases the risk by permitting bile reflux and devleopment of chronic gastritis |
|
|
Loss of ____________ is a key step in oncogenesis |
intercellular adhesion - especially diffuse gastric cancer - |
|
|
Mutation of ________ encoding E selectins is a key factor in diffuse gastric adenocarcinomas |
CDH1 |
|
|
Intestinal type gastric cancers are associated with |
FAP, mutations in B catenin, microsatellite instability Hypermethylation of TGFBRII, BAX, IGFRII, and p16/INK4a p53 mutations |
|
|
Gastric cancers are most commonly found in the ____________ |
antrum - lesser curvature more than greater |
|
|
Intestinal sporadic type cancers are associated with aberrations in ________ pathway |
WNT signaling pathway |
|
|
tumors with ___________ morphology tend to form bulky exophytic tumors composed of glandular structures developing from flat dysplasia or adenomas |
Gastric tumors of intestinal morphology |
|
|
Tumors with diffuse infiltrative pattern tend to be composed of _____________________ |
signet ring cells - intracellular mucin vacuoles push the nucleus to the periphery - fibrous desmoplastic response - no identified precursor lesions - loss of E selectin key via CDH1 - LINITUS PLASTICA |
|
|
Prognosis of gastric cancer depends on ______________ and extent of ______________ |
depth of invasion and extent of nodal/distant metastases |
|
|
Extranodal lymphomas are most common in the GI tract, especially the |
stomach - dyspesia and epigastric pain |
|
|
GI lymphomas are also called |
MALTomas - marginal B cell lymphomas - smaller fraction are large B cell lymphoma |
|
|
Extranodal marginal B cell lymphomas arise at site of __________ |
chronic inflammation, H pylori - antibiotic treatment can reduce tumor size |
|
|
Antibiotic resistant tumors |
11;18 tranlocation (most common) - links apoptosis inhibitor 2 gene (11) with the mutated MALT lymphoma gene (18) (14;18) translocation - MLT expression (1;14) BCL expression |
|
|
Common activity of these translocations is the constitutive activity of ________________ |
NFkB promoting cell survival Later, mutations of p53 and p16/INK4a tumor suppressors (Large B cell lymphoma) |
|
|
Morphological characteristics of MALT lymphomas |
dense infiltrate of atypical lymphocytes in lamina propria lymphoepithelial lesions |
|
|
Carcinoid tumors arise from diffusely distributed _______________ |
endocrine cells - arise in gut (small intestine) - over produce hormones |
|
|
Carcinoid tumor morphology |
yellow intramural/submucal masses forming polyps, firm, cause bowel obstruction Sheets of cohesive cells with scant granular cytoplasm and oval stippled nuclei |
|
|
Carcinoid tumor cells are typically positive for the neuroendocrine markers _______________ |
chromogranin A and synaptophysin |
|
|
Carcinoid clinical features |
- slow growing, effects due to hormones produced - gastrin = zollinger ellison - ileal = vasoactive products that result in cutaneous flushing, bronchospasm, increased bowl motility |
|
|
Cutaneous flushing, bronchospasm, increased bowel motility, and right sided cardiac valve thickening |
Carcinoid syndrome due to vasoactive peptide secretion from ileum - rarely occurs due to liver metabolizing peptides |
|
|
Most important prognostic factor of GI carcinoids tumors is ____________ |
primary site of the tumor |
|
|
Foregute carcinoid tumors _____________ |
rarely metastasize and are cured by resection |
|
|
Midgut carcinoid tumors (jejunum and ileum) are usually _______________ |
multiple and aggressive |
|
|
Hindgut tumors (appendix and colon) are usually |
found incidentally |
|
|
Appendiceal carcinoids are usually found at the tip and ___________ |
benign |
|
|
Colonic carcinoid tumors are large and ___________ |
metastasize |
|
|
Rectal carcinoids can secrete ___________ and/or cause pain but do not metastatsize |
Secrete polypeptide hormones |
|
|
___________________ is the most common GI mesenchymal tumor |
GI stromal tumor (GIST) - more than half in stomach - age 60 - increased NF-I |
|
|
Non-hereditary syndrome with GIST, paragangliomas, and pulmonary chondromas |
Carney triad |
|
|
GIST arise from the _______________ |
interstitial cells of Cajal (gut pacemakers) |
|
|
Major mutation in GIST |
Gain of function mutation in tyrosine kinase C-KIT (stem cell factor receptor) Constitutive activity of C-KIT leads to downstream activation of RAS, PI3K/AKT promoting tumor cell proliferation and survival |
|
|
GIST morphology |
solitary, well circumscribed fleshy masses, LARGE Epitheloid - plump and cohesive cells Spindle cell type |
|
|
Diagnostic marker for GIST |
c-KIT |
|
|
GIST symptoms are due to ___________ |
mass effects and blood loss |
|
|
Metastases of GIST occurs most often to __________ |
Peritoneal serosal nodes/liver |
|
|
GIST tx |
surgical resection Imatinib - tyrosine kinase inhibitor that inhibits c-KIT and PDGFRA |