|
|
17. A dopamine infusion of 3 mcg.kg-1.min-1 is likely to
A. increase myocardial contractility
B. increase renal blood flow
C. increase heart rate
D. increase systemic vascular resistance
E. all of the above
|
B
As classically described:
At low doses (1-3 mcg/kg/min) dopamine has predominantly D1 actions (increasing RBF)
At moderate doses (2-10 mcg/kg/min), it acts via B receptors to increase contractility and cardiac output
At high doses (> 10 mcg/kg/min), it acts via alpha-1 to increase SVR
|
|
|
26. Correct statements regarding trigeminal neuralgia include
A. associated sensory loss is common.
B. it most frequently occurs in the second or third division of the nerve (V2 or V3)
C. oedema of the trigeminal ganglion is usually seen on a cranial CAT scan
D. the pain is often bilateral
E. the pain is usually described as an intense deep ache
|
B
Emedicine article - http://emedicine.medscape.com/article/794402-overview
A – false. usually normal examination
B – true.
C – false.
D – false. unilateral
E – false. nature of pain – brief and paroxysmal, character of which is stabbing or shocklike and typically severe
|
|
|
33. A widened mediastinum after a chest injury is suggestive of a ruptured aorta especially if associated with
A. displacement of the mid-oesophagus to the right
B. right haemothorax
C. elevated left main bronchus
D. fractured left third rib
E. left pneumothorax
|
A
Oh’s ICU:
A widened mediastinum ALWAYS arouses suspicion of a ruptured aorta. In one series, mediastinal width greater than 8cm at the level of the aortic arch was present in all 10 patients with ruptured thoracic aorta.
Diagnosis is enhanced by ONE or more of the following radiological features:
* Left haemothorax
* Depressed left main bronchus
* Blurred outline of the arch or descending aorta
* Fractured first rib or left apical haematoma
* Displacement of the mid-oesophagus to the right (easily detectable with a nasogastric tube in situ)
|
|
|
40. Epidural analgesia in labour
A. typically increases uterine perfusion in healthy women
B. can result in lateral rectus muscle palsy if complicated by dural puncture
C. is particularly indicated for mothers with aortic stenosis
D. may cause hyperglycaemia in the presence of diabetes mellitus
E. may be lethal in the presence of maternal mitral stenosis if, following delivery, the block is prolonged
|
B
• A. False - "Continuous epidural analgesia with bupivacaine 0.075% increases the resistance of uterine artery and therefore possibly reduces the uterine blood flow" British Journal of Anaesthesia 2006 96(2):226-230
• B. True - We believe that a dural puncture during an attempted epidural anesthetic resulted in cerebrospinal fluid (CSF) leakage with a consequent headache. The CSF leak caused traction on the sixth cranial nerve resulting in lateral rectus muscle palsy. An epidural blood patch performed after the onset of symptoms did not acutely resolve the abducens nerve palsy." Szokol RAPM Volume 24, Issue 5, September-October 1999, Pages 470-472 wiki
o 'The complications of accidental dural puncture include headache, high or total spinal anaesthesia, 6th cranial nerve palsy and subdural haemorrhage.' from "Complications of obstetric anaesthesia" Amanda Pinder Current Anaesthesia & Critical Care (2006) 17, 151–162 wiki
• C. False. BUT traditionally contraindicated but now considered safe - epidural for labour indicated in AS. Epidural, CSE and spinal also been safely used in patients with AS for caesarian section http://books.google.com.au/booksid=lWcbqi14uDAC&pg=PA184&dq=epidural+and+aortic+stenosis#PPA185,M1
• D. False - Epidural reduces the stress in labour and enables better glucose control, therefore is indicated. http://books.google.com.au/books?id=5VsQJl6pBRUC&pg=PA206&dq=epidural+and+hyperglycaemia&ei=JEY0SpPuDoXWlQTaqdWrBQ
• E. ?False - epidural indicated for labour in MS. Epidural and CSE also used for C/S. No evidence found for mortality after prolonged block, not mention early removal.
|
|
|
41. Which of the following alternatives is correct regarding the range of values that odds ratios (OR) and relative risks (RR) can take?
A. OR (0 to positive infinity); RR (0 to positive infinity)
B. OR (negative infinity to positive infinity); RR (negative infinity to positive infinity)
C. OR (0 to 1); RR (0 to 1)
D. OR (0 to positive infinity); RR (negative infinity to positive infinity)
E. OR (negative 1 to positive 1); RR (negative 1 to positive 1)
|
|
|
|
42. A placebo should be used in a clinical trial when
A. observer bias is possible
B. a type one error is probable
C. an acceptable standard treatment is not known to exist
D. a placebo effect is anticipated
E. human patients are used as subjects
|
C
The Declaration of Helsinki : revising ethical research guidelines for the 21st century
Placebo use and risk
Article II. of the current Declaration states that "in any medical study, every patient - including those of a control group, if any - should be assured of the best proven diagnostic and therapeutic method. This does not exclude the use of inert placebo in studies where no proven diagnostic or therapeutic method exists."
Article 19 of the Proposed Revision states that "when the outcome measures are neither death nor disability, placebo or other no-treatment controls may be justified on the basis of their efficiency".
Benefit of the amendment
In certain circumstances, it permits placebo use even when a standard therapy already exists. This allows researchers to trial new and improved treatments in a more efficient, cost-effective manner.
Objection to the amendment
In freely allowing placebo use as long as participants do not die or become disabled, it fails to recognise other adverse health effects that could arise from placebo use, such as pain, discomfort or psychological stress.
|
|
|
59. In patients giving a history of penicillin allergy
A. cross-sensitvity to cephalosporins occurs in approximately 30% of patients
B. there is an increased liklihood of allergic reactions to neuromuscular blocking drugs
C. beta-lactamase resistant penicillins are less likely to provoke a response
D. a 'test dose' of one tenth the planned dose of penicillin should be given with a 5 minute delay before the main dose
|
B
o A – False
http://www.australianprescriber.com/magazine/17/3/62/5/
“Cephalosporins share a common beta-lactam ring with the penicillins but the degree of cross-reactivity is quite low. Around 3-7% of those with penicillin allergy, for example, may have allergic reactions to cephalosporins as well”
http://www.allergy.org.au/aer/infobulletins/hp_antibiotics.htm
o B – True
“A review of this subject found that patients with an allergy to penicillin were more likely (threefold) to experience an anaphylactic reaction to any other drug”
http://www.anesthesia-analgesia.org/cgi/content/full/97/5/1381
o C – false
Beta lacatamse resistant penicllins include flucloxacillin
“The major limiting factor for the use of penicillins is the high incidence of reported allergy (5%). ….Anaphylactic reactions occur in 1/10000 patients. Symptoms range from urticaria to anaphylactic shock. All other beta lactams should be avoided in these patients.”
http://www.utmb.edu/otoref/Grnds/Antibiotics-update-2005/Antibiotics-2005_0412.htm
o D – false - I wouldn’t give it IV
“skin prick testing is the gold standard for the diagnosis of penicillin allergy”
Essentials of allergy By Mamidipudi Thirumala Krishna, George Mavroleon, S. T. Holgate
|
|
|
70. A three-week-old infant presents with vomiting for 3 days and a diagnosis of pyloric stenosis. The most correct statement concerning resuscitation is that
A. alkalosis should be treated with dilute hydrochloric acid
B. 5% albumin is an appropriate fluid for initial treatment of
shock
C. fluid deficit should be completely replaced with 5% dextrose
D. hyponatraemia should be treated with 2N (twice normal) saline
E. potassium replacement should begin immediately
|
B
Whilst not specifically mentioned, the guidelines do refer to treating shock initially and I can’t see that 5% albumin would be an inappropriate fluid
RCH Clinical Practice guidelines:
• Fluid resuscitation may be necessary with 10-20ml/kg boluses of normal saline, for patients with moderate to severe dehydration
• Commence IV Fluids (0.45% Saline with 5% or 10% Dextrose + 10mmol KCl / 500mls) at 100mls/kg/day initially. Review after 4-6 hours (see below).
• Stop oral feeds
• Insert a nasogastric tube if vomiting continues despite stopping feeds. Replace nasogastric losses with IV normal saline
• Repeat U&E, Acid-Base 4-6 hourly initially and adjust fluid accordingly. The aim for most infants should be to fully correct fluid and electrolyte deficits within 48 hours.
• Initial KCl may be required if significant hypokalaemia
• Replace deficit, in addition to maintenance, in those infants who are clinically dehydrated (weight is a good marker of the degree of dehydration)
|
|
|
76. When magnesium sulphate is used in the treatment of pre-eclampsia
A. its tocolytic action commonly delays the progress of labour
B. it potentiates neuromuscular blockade by depolarising muscle relaxants
C. therapeutic blood levels are 6 - 8 mmol.l-1
D. when given as an infusion it frequently produces hypotension
E. none of the above
|
E
• A - False.
• B - True from older quotes, BUT "The interaction of magnesium with succinylcholine is controversial. Initial studies suggested potentiation of depolarizing blockade or no significant effect. However, one study suggests that magnesium may antagonize the block produced by succinylcholine." Miller, 6th ed. p.516-7 and Stoelting (Pharm) pg. 550 . Potentiation of suxamethonium by Mg therapy is not a consistent observation. Patients treated with Mg do not exhibit fasciculations after administration of suxamethonium
o Old evidence: Magnesium and the Anaesthetist. CEACCP.
• C - False.
• D - False.
• E – True.
|
|
|
84. In an acute malignant hyperthermia episode
A. the serum creatinine kinase level peaks within one hour
B. the peak serum creatinine kinase level is a good indicator of
the amount of muscle involved
C. elevated creatinine kinase levels contribute to acute renal
failure
D. the serum myoglobin level does not peak for at least 24 hours
E. muscle rigidity occurs in 75% of cases
|
E
In an acute malignant hyperthermia episode
A. the serum creatinine kinase level peaks within one hour - false: "Additional features that increase the likelihood of underlying MH are signs of metabolic stimulation and grossly elevated plasma creatine kinase (CK) and myoglobin concentrations. There may also be evidence of myoglobinuria; this occurs earlier than CK increases. CK reaches a peak approximately 24 h after the insult and, even in patients with no muscle disorder, can reach 50 times the upper limit of normal." (Malignant hyperthermia BJA CEPD Reviews 2003 Feb 01, 3: 5-9.)
B. the peak serum creatinine kinase level is a good indicator of the amount of muscle involved - false: "The CK increase resulting from surgery is similar to that seen after these acute MH episodes because of coincident muscle damage, but it also may be a result of CK release from other tissues. CK is found in brain and intestinal tissue; CK may increase substantially after a bowel infarction (6). Maternal labor appears to increase CK, possibly in relation to physical exertion (e.g., pushing) during the second stage of labor (14,15). Other conditions associated with increased CK include myocardial infarction (6), fever (16), stroke (17), and tubal pregnancy" (A & A November 1995 vol. 81 no. 5 1039-1042)
C. elevated creatinine kinase levels contribute to acute renal failure - false: "Plasma myoglobin concentrations are sufficient to cause renal tubular damage and acute renal failure." (Malignant hyperthermia BJA CEPD Reviews 2003 Feb 01, 3: 5-9.)
D. the serum myoglobin level does NOT peak for at LEAST 24 hours - false: "Increases in serum myoglobin occur earlier after muscle injury than increases in CK. Peak levels of CK may not be observed until 12 to 24 hours after muscle injury." (Malignant hyperthermia and myotonic disorders, Anesthesiology Clinics of North America - Volume 20, Issue 3 (September 2002))
muscle rigidity occurs in 75% of cases - true: "The occurrence of generalized muscle rigidity is the most specific sign of MH [11] [12]" (Malignant hyperthermia and myotonic disorders, Anesthesiology Clinics of North America - Volume 20, Issue 3 (September 2002))
|
|
|
88. The optimal patient position for anaesthetising a woman at term with an umbilical cord presenting externally is
A. knee-chest (i.e. on hands and knees)
B. left lateral (i.e. on side with left side down)
C. supine with head down (and lateral tilt)
D. supine with head elevated (and lateral tilt)
E. supine and level (with lateral tilt)
|
|
|
|
90. In chronic obstructive pulmonary disease (COPD), the variable most closely associated with prognosis is
A. arterial carbon dioxide partial pressure (PaCO2)
B. arterial oxygen partial pressure (PaO2)
C. forced expiratory volume in one second (FEV1)
D. forced vital capacity (FVC)
E. response to bronchodilators
|
C
REPEAT
Australian and New Zealand COPD site:
'Spirometry is the most reproducible, standardised and objective way of measuring airflow limitation, and FEV1 is the variable most closely associated with prognosis.”
|
|
|
96. A 46 year old brewery worker has cirrhosis of the liver with oesophageal varices and has bled from these varices on one occasion. A portacaval shunt is being considered as definitive treatment for his portal hypertension. The operation would be contraindicated if he had
A. a serum bilirubin greater than 50 micromol.litre-1
B. a serum albumin less than 30 gram.litre-1
C. ascites
D. all of the above are true
E. none of the above are true
|
|
|
|
97. Features of perfluorocarbon emulsions when used as blood substitutes include
A. a dose dependent half-life
B. a sigmoidal oxygen dissociation curve
C. liver dysfunction, which is a common side-effect
D. metabolism by the liver
E. prolongation of the the bleeding time
|
A
Artif Cells Blood Substit Immobil Biotechnol. 1994;22(4):1043-54.
Pharmacokinetics and side effects of perfluorocarbon-based blood substitutes
Perfluorochemicals are fluorine-saturated carbon-based molecules which demonstrate utility in the areas of imaging and oxygen delivery. In general, these molecules are biologically inert and, therefore, do not pose toxicologic risk from metabolic degradation. Intravenous (i.v.) perfluorocarbon (PFC) emulsions are cleared from the blood through a process involving phagocytosis of emulsion particles by reticuloendothelial macrophages (RES) and ultimate elimination through the lung in expired air. RES phagocytosis of PFC emulsion particles leads to characteristic, predictable, and reversible biological effects that are a consequence of a normal host-defense mechanism. This mechanism is characterized by dose-related stimulation of macrophages and subsequent release of intracellular products (particularly metabolites of the arachidonic acid cascade and cytokines) which are responsible for most of the biological effects associated with i.v. PFC emulsions (i.e., cutaneous flushing and fever at lower doses, and macrophage hypertrophy and recruitment at higher doses). These biological effects are reversible, and do not result in any permanent tissue alteration, even with prolonged exposure at relatively high doses. The rate of PFC elimination from the RES is proportional to the vapor pressure of the PFC, inversely proportional to molecular weight and positively influenced by lipophilicity. This dose-dependent respiratory excretion occurs with no evidence of metabolic products. Repeated administration of high doses of PFC emulsion may lead to a saturation of the RES-mediated clearance capacity, resulting in a redistribution of PFC to non-RES tissues and ingestion by resident or mobile macrophages. This condition is benign with respect to the integrity of the surrounding parenchyma, as well as to the macrophages themselves. Increased pulmonary residual volume (IPRV) due to pulmonary gas (air) trapping, a reversible side effect, has been observed with i.v. doses of PFC emulsion in some animal species. The gross morphological change associated with IPRV is not accompanied by any histological alteration other than the appearance of vacuolated macrophages (characteristic of the normal clearance mechanism) and some minor, increased interalveolar cellularity. Animal lungs affected by IPRV have a normal, pale pink appearance with no visible lesions or signs of edema. The degree of IPRV is dependent on species, PFC dose, and type of PFC administered; PFCs with higher vapor pressures produce the most severe cases of IPRV in sensitive species. Species sensitivity depends upon physiological and morphological characteristics. There is no evidence indicating that IPRV occurs in humans. Although i.v. PFC emulsions may elicit minor untoward effects, these effects are reversible and, at clinically relevant doses, do not pose a toxicologic risk.
|
|
|
98. Each of the following is effective in the treatment of pain from acute herpes zoster EXCEPT
A. acyclovir
B. amitriptyline
C. carbamazepine
D. corticsteroids
E. topical aspirin
|
C
• A – False. (I.e. is effective.)
o From APMSE 2010:
• B – False. (I.e is effective.)
o From Priciples and Practice of Pain Medicine 2nd edition by Warfield & Bajwah: “There is a strong consensus among clinical investigators that centrally active antidepressants should be tried in any patient who is not obtaining pain relief, whether or not he or she appears depressed. Tricyclics and anxiolytics frequently are given together because, although depression is not common in acute herpes zoster, many patients experience anxiety along with the severe pain. The most widely used combination is amitriptyline and fluphenazine. Amitriptyline alone has been shown to significantly reduce pain in older patients by more than one half, making a strong argument for its use with an antiviral in this group of patients. In addition to their antidepressant and analgesic properties, tricyclics are also sedatives (for sleep regulation).”
o From APMSE 2010:
• C – True – I.e. not effective – first line therapy in trigeminal neuralgia though.
• D – False. (I.e. is effective.)
o From APMSE ‘10:
• Thus corticosteroids do not prevent nor reduce the duration of post-herpetic neuralgia BUT is of benefit symptomatically
• Regarding TOPICAL corticosteroids - From APMSE ’10:
• E – False. (I.e. is effective.)
|
|
|
99. Cerebral palsy is associated with each of the following EXCEPT
A. gastro-oesophageal reflux
B. increased sensitivity to non-depolarising muscle relaxants
C. malnutrition
D. recurrent aspiration
E. scoliosis
|
B
"Non-depolarizing neuromuscular blocking agents are less potent and have a shorter duration of action in patients with CP owing to the up-regulation of ACh receptor."
-CEACCP Vol 10 (3) 2010
|
|
|
100. True statements about phantom limb pain include each of the following EXCEPT
A. phantom limb pain commonly occurs within the first few days after surgery
B. phantom limb pain occurs in up to 85% of patients
C. the risk of phantom pain is increased after chemotherapy
D. the risk of phantom pain is influenced by preoperative pain intensity
E. the risk of phantom pain is influenced by the degree of preoperative depression
|
E
A. True "75% of patients will report phantom pain within the first few days after amputation" (APMSE 2005 2nd Ed. No change in update)
B. True "The incidence of PLP is estimated to be 30-85%" (APMSE 2005 2nd Ed. No change in update)
C. True (APMSE 2005 2nd Ed. No change in update)
D. True (APMSE 2005 2nd Ed. No change in update)
E. False. POSTOPERATIVE Depression is a risk factor for chronic postsurgical pain (APMSE 2005 2nd Ed. p11 No change in update)
|
|
|
101. In relation to obstetric haemorrhage
A. amniotic fluid embolism is unlikely to present as unexplained haemorrhage
B. coagulopathy is uncommon after severe maternal abruption
C. the risk of placenta accreta only increases after a second caesarean section
D. treatment of an atonic uterus with injectable prostaglandin rarely causes adverse maternal effects
E. intravenous magnesium may facilitate replacement of an inverted uterus
|
E
Miller:
"Uterine relaxation may be necessary to replace the uterus; â-sympathomimetic agents, magnesium, and nitroglycerin all have been used to achieve this goal."
|
|
|
102. Appropriate practice when performing central neuro-axial block should include all of the following EXCEPT
A. application of an alcohol based antiseptic at least twice
B. application of an alcohol based antiseptic that is allowed to dry
C. a surgical hand wash
D. disinfection of the neck of ampoules being cracked open by an assistant
E. wearing a new facemask
|
C
Wiki votes between A and D, However:
Benhamou D. Hospital policy for prevention of infection after neuraxial blocks in obstetrics. Int J Obstet Anesth 2002;11:265-269
A – “The patient's back should be disinfected at least twice (alcohol–iodine, alcoholic solution of chlorhexidine or of povidone–iodine)”
B – Certainly true
C – Not exactly a surgical hand wash: “must wash his hands with an antiseptic soap solution, dry them on a sterile towel and wear sterile gloves”
D – “Drugs must be prepared contemporaneously and in a sterile manner (collar of non-sterilized ampoules cleaned with alcohol)”
E – “Any person involved with the procedure must wear a cap and a new face mask”
|
|
|
103. Best evidence in obstetric anaesthesia supports each of the following assertions EXCEPT
A. colloid effectively prevents hypotension from regional anaesthesia, but crystalloid does not
B. fentanyl added to spinal bupivacaine for caesarean section has no influence on the incidence of intraoperative nausea
C. high doses of ephedrine (>15 mg) are more likely to cause hypertension than prevent hypotension
D. in labour, combined spinal-epidural analgesia is associated with faster onset and greater maternal satisfaction than epidural analgesia
E. in nulliparous women, epidural analgesia in labour, compared with intravenous opioid analgesia, does not increase caesarean section rate
|
B & D
Whilst onset is faster there is no difference in satisfaction.
ANZCA pain book:
“Combined spinal epidural (CSE) analgesia provided faster onset of analgesia compared with epidural analgesia. However, as CSE did not improve satisfaction or mobilisation, and increased the risk of pruritus, clinical advantages over epidural analgesia (either traditional or low dose) are limited (Simmons et al, 2007 Level I)”
B also true – reduces visceral stimulus for N&V
|
|
|
104. Each of the following statements concerning surgery for correction of scoliosis is true EXCEPT
A. one third of the blood loss occurs postoperatively
B. major blood loss is frequently accompanied by a consumptive coagulopathy
C. surgery will halt progression of the restrictive lung deficit
D. the major neurological deficits that occur are usually due to damage to the posterior columns of the spinal cord
E. the use of aprotinin reduces blood loss
|
D
Anaesthesia for Correction of Scoliosis in Children. Anaesthesia and Intensive Care, Vol. 32, No. 4, August 2004
• A : “Scoliosis correction may be associated with major blood loss (>50% of blood volume) and the development of coagulopathy. Blood loss is related to length of procedure and number of segments fused. About a third of the blood loss occurs in the postoperative period. The 24 hour blood loss has been calculated at about 200 ml/segment fused".
• B – “The coagulopathy is both dilutional and consumptive"
• C – “Surgical correction does not reverse the restrictive lung deficit but will halt its progression”
• D – “more vulnerable anterior cord”
• E – “aprotinin is the most studied and the most effective, halving blood loss in high-risk patients”
|
|
|
105. In the elderly patient
A. renal dysfunction can be excluded if the serum urea and creatinine concentration are within normal limits
B. sedation does not negate the benefits of regional anaesthesia with respect to postoperative cognitive dysfunction
C. shivering may be less effective in restoring body temperature, than in younger adults
D. the effect of ephedrine in treating hypotension is similar to younger adults
E. the uptake of sevoflurane is similar to younger adults, because of its low blood gas solubility
|
C
" Perioperative hypothermia in the high-risk surgical patient. Best Practice & Research Clinical Anaesthesiology, Volume 17, Issue 4, Pages 485-498 K. Leslie, D. Sessler
"elderly or debilitated patients shiver less effectively than younger patients
|
|
|
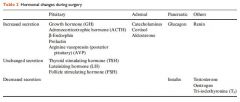
106. During surgery there is increased secretion of each of the following hormones EXCEPT
A. aldosterone
B. glucagon
C. growth hormone
D. thyroid stimulating hormone
E. vasopressin
|
|
|
|
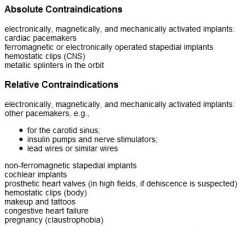
107. Which of the following is NOT an absolute contraindication to magnetic resonance imaging?
A. cardiac pacemaker
B. cerebral aneurysm clips
C. cochlear implant
D. implanted defibrillator
E. prosthetic heart valve
|
|
|
|
108. According to the AHA (American Heart Association) Guidelines intermediate clinical predictors of increased perioperative cardiovascular risk include each of the following EXCEPT
A. prior heart failure
B. diabetes mellitus
C. previous myocardial infarct
D. renal insufficiency
E. uncontrolled systemic hypertension
|
E
Active cardiac conditions require investigation and likely intervention unless the surgery is an emergency.
• Unstable coronary Sx
• Decompensated heart failure
• Significant arrythmias
• Severe valvular disease
Clinical Risk Factors to stratify other patients
• Hx of heart disease
• Prior heart failure
• Cerebrovascular disease
• Diabetes mellitus
• Chronic renal impairment
Procedure related risk
• Vascular (>5% risk of MI and/or death). Includes all vascular surgery except carotid endarterectomy
• Intermediate (Less than 5%, more than 1%). Carotid endarterectomy, abdominal, thoracic, neuro, head and neck, major orthopaedic, prostatic, etc.
• Low risk (less than 1%). Ambulatory, eyes, superficial, endoscopy, breast
|
|
|
109. The MAC (Minimum Alveolar Concentration) of inhalational anaesthetics is DECREASED by
A. hypercarbia (pCO2 of 55 mmHg)
B. hypernatraemia
C. hyperthermia
D. lithium
E. tricyclic antidepressants
|
D
A – false, no change
B – false, increased
C – false, increased
D – true, decreased (Stoelting)
E – trueish, not much on TCA but could increase catecholamines thus inc MAC
|
|
|
110. Immediate life threatening complications following pneumonectomy include all of the following EXCEPT
A. acute right heart failure
B. broncho-pleural fistula
C. cardiac herniation
D. pulmonary oedema
E. right to left shunt
|
B
Note difference in wording comparing to similar questions from previous paper. "Immediate life threatening" vs "early complication". I think broncho-pleural fistula is not immediately life threatening whereas the other options are
|
|
|
111. During controlled ventilation of a neonate prior to repair of a truncus arteriosus which of the following is MOST likely to be deleterious?
A. controlled hypoventilation
B. ventilation with air
C. ventilation with an FiO2 of 0.18
D. ventilation with nitric oxide
E. ventilation with PEEP of 3 cmH2O
|
D
Truncus arteriosus occurs when the single great vessel fails to separate completely, leaving a connection between the aorta and pulmonary artery. High PVR ensures that blood is directed systemically. Ultimately high PVR results in obstructive pulm vasc disease and right heart failure (eisenmengers). Occasionally this reduces pulm flow to the extent that longer survival is possible. Similarly pulm stenosis may allow same effect.
However the important thing in mananging these infants is to preserve systemic flow and minimise further pulm shunting. Avoid hyperventilation and high FiO2. Medical mx includes usual failure medication. NO likely to cause decrease in PVR thus bad
|
|
|
112. What percentage of the total greenhouse gas effect is due to the use of volatile anaesthetic agents?
A. 0%
B. less than 1%
C. 2%
D. 5%
E. 10%
|
|
|
|
113. In the diagnosis of postoperative myocardial infarction
A. echocardiography has little role to play
B. infarct size can be judged from cumulative enzyme release
C. new left bundle branch block on ECG confirms acute infarction
D. serum troponins have high sensitivity and are detectable for
up to 5 days
E. ST segment elevation is extremely common
|
B
CEACCP:
Serial CK-MB can be best employed in clarification of the timing of an infarct or the size of the infarct, on the basis of cumulative enzyme release.
|
|
|
114. In patients undergoing thoracotomy, techniques which reduce the incidence of intraoperative atrial fibrillation include
A. hyperventilation
B. pre-operative loading with digoxin
C. rocuronium, rather than pancuronium
D. thoracic epidural bupivacaine
E. thoracic epidural morphine
|
D
Thoracic Epidural Bupivacaine Attenuates Supraventricular Tachyarrhythmias After Pulmonary Resection (Anesth Analg 2001;93:253–9) This reference only compares epidural bupivacaine and epidural morphine, no mention of any of the other options however
|
|
|
115. The signs of exposure to a nerve agent such as Sarin or VX include
A. bronchodilation
B. dry skin
C. muscle fasciculation
D. pupillary dilatation
E. tetany
|
C
eMedicine:
Sarin & VX– potent irreversible AChE inhibitor
Both organophosphates
ACh accumulates throughout the nervous system, resulting in overstimulation of muscarinic and nicotinic receptors. Clinical effects are manifested via activation of the autonomic and central nervous systems and at nicotinic receptors on skeletal muscle.
• Mnemonic devices used to remember the muscarinic effects of organophosphates are SLUDGE (salivation, lacrimation, urination, diarrhea, GI upset, emesis) and DUMBELS (diaphoresis and diarrhea; urination; miosis; bradycardia, bronchospasm, bronchorrhea; emesis; excess lacrimation; and salivation). Muscarinic effects by organ systems include the following:
• Cardiovascular - Bradycardia, hypotension
• Respiratory - Rhinorrhea, bronchorrhea, bronchospasm, cough, severe respiratory distress
• Gastrointestinal - Hypersalivation, nausea and vomiting, abdominal pain, diarrhea, fecal incontinence
• Genitourinary - Incontinence
• Ocular - Blurred vision, miosis (constrict)
• Glands - Increased lacrimation, diaphoresis
• Nicotinic signs and symptoms include muscle fasciculations(cause depolarizing blockade in overdose Yentis p4), cramping, weakness, and diaphragmatic failure. Autonomic nicotinic effects include hypertension, tachycardia, mydriasis, and pallor.
|
|
|
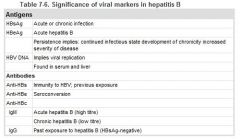
116. Immunological evidence of immunity to hepatitis B is the presence of
A. hepatitis B core antibodies
B. hepatitis B core antigen
C. hepatitis B surface antibodies
D. hepatitis B surface antigen
E. any of the above
|
|
|
|
117. The patient most likely to sustain blunt cardiac trauma (cardiac contusion) is a
A. back seat passenger in a motor vehicle which crashes at a speed of 60 km.hr-1
B. motor bike rider who falls from his bike on a bend travelling at 50 km.hr-1
C. painter who falls 10 metres on to grass
D. seventy-year-old patient who had cardiopulmonary rescusitation (CPR) performed by a passerby in the street
E. water skier who falls from his skis travelling at a speed of 40 km.hr-1
|
C
Whilst MVA’s are most common cause, not sure if back seat passenger in MVA wold still be most likely (I.e. need something to make inpact with). As per 2nd reference this would leave fall as most likely
Blunt Cardiac Trauma: The Journal of Emergency Medicine, Vol. 35, No. 2, pp. 127–133, 2008:
"Motor vehicle accidents are the major cause of blunt trauma, accounting for 81% of cases, followed by crush injuries (5.7%). Chest compressions during cardiopulmonary resuscitation efforts may also lead to cardiac injury."
European Journal of Emergency Medicine: Cardiac contusion following blunt chest trauma. December 2006 - Volume 13 - Issue 6 - pp 373-376:
"Cardiac contusion following blunt chest trauma is not rare, and the works in the literature report incidence rates between 5 and 50%. Traffic accidents are the most frequent cause of cardiac contusion followed by violent fall impacts, aggressions and the practice of risky sports."
Trauma. By William C. Wilson, Christopher M. Grande, David B. Hoyt. p. 367-8. CRC Press, 2007
"Myocardial contusion refers to damage occurring to the myocardium from blunt trauma. The classic setting is a decelerational injury where an individual is moving forward, the chest strikes an immobile or slower object, and the heart is compressed within the thorax. Motor vehicle accidents or falls from a significant height are common causes of decelerational injuries. However, any mechanical motion that generates stress on the heart or any direct transfer of energy to the heart can result in tissue damage and contusion"
|
|
|
118. A three-week old infant presents with pyloric stenosis and 3 days of vomiting. A typical electrolyte profile would be
A. Na+ 130 mmol.l-1 K+ 5.8 mmol.l-1 Cl- 98 mmol.l-1 HCO3-
17 mmol.l-1
B. Na+ 148 mmol.l-1 K+ 4.1 mmol.l-1 Cl- 108 mmol.l-1 HCO3
13 mmol.l-1
C. Na+ 135 mmol.l-1 K+ 4.5 mmol.l-1 Cl- 90 mmol.l-1 HCO3-
30 mmol.l-1
D. Na+ 130 mmol.l-1 K+ 2.8 mmol.l-1 Cl- 90 mmol.l-1 HCO3-
28 mmol.l-1
E. Na+ 130 mmol.l-1 K+ 3.9 mmol.l-1 Cl- 98 mmol.l-1 HCO3-
17 mmol.l-1
|
D
CEACCP 2001
“the metabolic picture is a chloride-responsive hypochloraemic, hypokalaemic, hyponatraemic metabolic alkalosis”
|
|
|
119. When placing a patient in the lithotomy position
A. the femoral nerve is NOT at risk of injury
B. the common peroneal nerve is NOT at risk of injury
C. flexion at the hips of greater than 90 degrees will protect the obturator nerve
D. damage to the sciatic nerve may be prevented by exaggerated external rotation of the hips
E. damage to peripheral nerves is more commonly due to compression of blood supply, rather than direct pressure
|
E
• A - False. "The following from Warner Neuropathies, Blindness & Positioning Problems in ASA Refresher Course 2005, Ch 127 p3: "A 1994 retrspective review of patients in the lithotomy position found that the most common lower extremity neuropaties were the common peroneal (81%) sciatic (15%) and femoral (4%)" Wiki.
• B - False. "The common peroneal nerve is particularly vulnerable and must be protected when the patient is placed in the lithotomy position." Miller, 6th ed., p. 2293.
• C - False. "Extreme flexion of the hip joints can cause neural damage by stretch (sciatic and obturator nerves) or by direct pressure (compression of the femoral nerve as it is passes under the inguinal ligament). Distally, the common peroneal nerve and saphenous nerve are particularly at risk of compression injury as they wind round the neck of the fibula and medial tibial condyle, respectively." Patient Positioning in Anaesthesia. Knight D, Mahajan R, CEACCP Volume 4 October 2004 and "The obturator nerve passes through the pelvis and is occasionally injured by surgical retractors placed deep below the pelvic brim. Excessive flexion can also injure the obturator nerve." Miller, 6th ed., p. 1153-1158.
• D - False. See quote at C.
• E - True. "The mechanism of injury to superficial nerves is usually compression of the vasa vasorum and subsequent ischaemia....Superficial nerves (e.g. ulnar and common peroneal) are especially vulnerable in thin patients." Injury during anaesthesia. S Contractor, JG Hardman. BJA CEACCP Volume 6 Number 2 2006
|
|
|
120. Transfusion related acute lung injury (TRALI)
A. can be caused by all homologous blood components, but particularly FFP (fresh frozen plasma)
B. is associated with significantly elevated pulmonary artery pressure
C. is the commonest cause of morbidity associated with blood transfusion
D. should be treated with high dose steroids
E. typically presents 24 hours following transfusion
|
A
CEACCP 2006
A. True. “The 2004, SHOT report describes 13 reactions as follows: 6 to FFP, 4 to platelets, 2 to packed cells and 1 to whole blood. The preponderance of reactions with FFP and platelets is thought to result from their ‘high plasma component’, in comparison with packed cells and cryoprecipitate, which have a ‘low plasma component”.
B. False. “Invasive monitoring in TRALI demonstrates normal intracardiac pressures”
C. False. “TRALI is the most common cause of major morbidity and death after transfusion”. Incorrect blood component transfused (IBCT) was the commonest reported morbidity in 2004-05 SHOT report.
D. False. No evidence for steroids, management involves PEEP and ventilatory support.
E. False. “It presents as an acute respiratory distress syndrome (ARDS) either during or within 6 h of transfusion”
|
|
|
121. A six-week-old baby is booked for elective right inguinal hernia repair. An appropriate fasting time is
A. 2 hours for formula milk
B. 2 hours for clear fluids
C. 5 hours for breast and formula milk
D. 6 hours for solids
E. 6 hours for solids and 3 hours for all fluids
|
B
RCH Guidelines
Solids 6 hours
Formula/Cow’s milk 4 hours
Breast milk 3 hours
Clear fluids 2 hours
Baby is 6 weeks, therefore not on solids!
|
|
|
122. Clopidogrel
A. acts via the glycoprotein IIb/IIIa receptors on platelets
B. binds reversibly to its receptor on the platelet
C. blocks thrombin mediated platelet activation
D. inhibits ADP induced platelet activation
E. is inhibited by concurrent aspirin usage
|
|
|
|
123. Correct statements regarding fondaparinux include each of the following EXCEPT
A. it has a structure unrelated to heparin
B. it is administered once daily
C. it is a synthetic, selective Factor Xa inhibitor
D. it is recommended for DVT prophylaxis in major orthopaedic surgery
E. the dosage does NOT need to be adjusted for age and sex
|
A
A. false 'Apart from the O-methyl group at the reducing end of the molecule, the identity and sequence of the five monomeric sugar units contained in fondaparinux is identical to a sequence of five monomeric sugar units that can be isolated after either chemical or enzymatic cleavage of the polymeric glycosaminoglycans heparin and heparan sulfate (HS).'
B. true
C. true
D. true, this is what it is licensed for
E. true standard dose for all
|
|
|
124. Complications of severe anorexia nervosa (body weight < 40% ideal) include all of the following EXCEPT
A. cardiomyopathy
B. delayed gastric emptying
C. hypokalaemia
D. hypercalcaemia
E. prolonged QT interval
|
D
Hypo not hypercalcaeima
MEDSCAPE
In anorexia nervosa:
CVS
• Sinus brady usually
• AV block, St depression, T wave inversion, Qt prolongation
• Beware of arryhtmias under GA – 16-62%
• Higher rate of MVP
Resp
• Metabolic acidosis - laxative abuse & vomiting
• Asp pneumonia
• Decreased compliance from starvation
Renal
• Proteinuria in >50%
• Dec GFR
• Hyponatraemia, hypokalaemia, hypochloraemia, hypomagnesaemia, and loss of hydrogen ions.
• Hypocalcaemia due to decreased dietary intake may also occur
Gastrointestinal
• Salivary gland hyperplasia, dental caries, periodontis, oesophageal strictures, Mallory-Weiss tears, gastritis, and oesophagitis
• Binge-eating patients may develop gastric dilatation and, in acute circumstances, gastric infarction or perforation
• Strict dieting appears to prolong gastric emptying times
• Abnormal LFT
• 'Refeeding syndrome'
Endocrine
• Amenorrhoea - diagnostic criterion for anorexia nervosa
• Menstruation ceases BMI< 15
• May sometimes display features of panhypopituitarism
• Decreased T3/T4
Immunological and Haematological
• Normal immune till weight < 50% of normal
• anaemia is unusual
• Anorexic patients also demonstrate raised cholesterol levels and hypercarotenaemia.
Neurological
• white (revesible) and grey (non-reversible) matter changes in the brain
• coma and seizures may occur as a result of hypoglycaemia and electrolyte disturbances,
• Mild neuropathies, fatigue, and generalized weakness common
• Pain threshold may be raised in anorexics
• loss of insulating adipose tissue, hypothermia
• body temperatures of commonly < 36.3°C.
Musculoskeletal
• Generalized myalgia - hyponatraemia, hypokalaemia, and hypophosphataemia
• muscle weakness
• osteopenia and osteoporosis
Investigations
• FBE, U&E, CMP, LFT, BSL
• Urinalysis – proteinuria
• ECG
• TTE
Anaesthetic
• weigh
• NG for delayed emptying prior to induction
• sodium citrate, ranitidine
• RSI
• Beware of positioning / pressure care
• Avoid hypothermia
• Neuromuscular blocking (hypokalaemia / hypocalcemia prolong effect)
|
|
|
125. Each of the following are causes of right axis deviation on the ECG (electrocardiogram) EXCEPT
A. chronic lung disease
B. lateral myocardial infarction
C. left anterior hemiblock
D. left posterior hemiblock
E. right ventricular hypertrophy
|
C
Causes of right axis deviation
• normal finding in children and tall thin adults
• right ventricular hypertrophy
• chronic lung disease even without pulmonary hypertension
• anterolateral myocardial infarction
• lateral infarction
• left posterior hemiblock
• pulmonary embolus
• Wolff-Parkinson-White syndrome - left sided accessory pathway
• atrial septal defect
• ventricular septal defect
|
|
|
126. Which of the following herbal treatments is most likely to cause central serotonin syndrome when combined with a serotonin reuptake inhibitor?
A. echinacea
B. ginko
C. ginseng
D. St John’s Wort
E. valerian
|
D
http://www.anesthesia.wisc.edu/Clinic/providerinfo/herbals.html
A – Echinacea - hepatotoxicity, decreased effectiveness of steroids
B – Ginko – Used for cognitive disorders. Causes bleeding & reduced efficacy of antiepileptic drugs
C – Gensing – Boosts energy. Mild sympathomimetic. Interacts with MAOI. May cause bleeding, hypoglycaemia
D – St Johns Wart - Used for Anxiety, depression and sleep disorders = Slow recovery, induces P450, Serotinergic Syndrome
E – Valerian – Used for sleep disorders. Potentiates sedative effects of anaesthesia. Withdrawal may cause seizures
|
|
|
127. The operative procedure most frequently associated with post-operative visual loss due to ischaemic optic neuropathy is
A. coronary artery bypass surgery
B. sitting position craniotomy
C. spinal surgery in the prone position
D. urgent caesarean surgery
E. urgent trauma surgery
|
A
Anesthesiology 2006; 105:652–9 The American Society of Anesthesiologists Postoperative
Visual Loss Registry. Analysis of 93 Spine Surgery Cases with Postoperative Visual Loss:
• Spine 0.2%
• Cardiac 4.5%
The Prevalence of Perioperative Visual Loss in the United States: A 10-Year Study from 1996 to 2005 of Spinal, Orthopedic, Cardiac, and General Surgery. Anesthesia & Analgesia Issue: Volume 109(5), November 2009, pp 1534-1545
Cardiac and spinal fusion surgery had the highest rates of POVL. The national estimate in cardiac surgery was 8.64/10,000 and 3.09/10,000 in spinal fusion
|
|
|
128. In patients with renal failure each of the following drugs has prolonged clearance or has active metabolites with prolonged clearance EXCEPT
A. aspirin
B. buprenorphine
C. codeine
D. pethidine
E. tramadol
|
B
ANZCA Pain management guidelines:
In liver impairment:
Safest - sufentanil
OK - fentanyl, alfentanil, morphine
Reduce dose - tramadol, LA, panadol (use with caution)
NEVER - carbamezepine, valproate, methadone, pethidine
In renal impairment:
Safest - fentanyl, alfentanil, buprenorphine, panadol, ketamine, sufentanil
OK - oxycodone (because metabolite oxymorphone has minimal known clinical effects)
Reduce dose - all others including: clonidine, morphine, gabapentin, LA, tramadol
NEVER - pethidine, dextropropoxyphene
|
|
|
129. The adverse outcomes resulting in the most frequent medicolegal claims against anaesthetists are
A. dental damages from airway instrumentation
B. eye injuries
C. non-obstetric epidural complications
D. obstetric epidural complications
E. peripheral nerve injuries
|
A
Cass NM. Medicolegal claims against anaesthetists: a 20 year study. Anaesth Intensive Care. 2004 Feb;32(1):47-58
|
|
|
130. The most correct statement describing the effect of the antithrombotic agents on the coagulation cascade is that
A. low molecular weight heparin directly inhibits activated
factor X
B. low molecular weight heparin directly inhibits thrombin
C. unfractionated heparin directly inhibits activated factor X
D. unfractionated heparin directly inhibits thrombin
E. ximelagatran directly inhibits thrombin
|
E
All the others act via antithrombin III
CEACCP Volume 6 Number 4 [p156–159] 2006 Anticoagulants and the perioperative period:
• “Ximelagatran is a new, oral, directly acting thrombin inhibitor that has been shown to be more effective than placebo in prevention of thromboembolism with little increase in risk of haemorrhage”
|
|
|
131. Prior to surgical stimulation, which of the following drugs, when added to propofol or volatile anaesthesia, will decrease the bispectral index (BIS)?
A. 70% nitrous oxide
B. ketamine (0.5mg. kg-1)
C. midazolam (0.2 mg.kg-1)
D. remifentanyl infusion (0.25 microg.kg-1.min-1)
E. all of the above
|
C
Monitoring depth of anaesthesia by EEG – Whyte - British Journal of Anaesthesia | CEPD Reviews | Volume 3 Number 4 2003
• Nitrous oxide, at inspired concentrations of up to 50%, does not reduce baseline BIS values
• Ketamine causes EEG activation, complicating BIS interpretation
Update on Bispectral Index monitoring – Johansen - Best Practice & Research Clinical Anaesthesiology Vol. 20, No. 1, pp. 81–99, 2006
• Preliminary evidence demonstrates that remifentanil, even at large doses, produced no modification of BIS obtained during a constant propofol infusion
|
|
|
132. In patients who have sustained a dural puncture headache following a dural puncture during epidural catheter placement (18G or greater), the percentage of patients achieving persistent relief of headache with blood patching (performed after 24 hours) is
A. less than 30%
B. 30 - 45 %
C. 45 - 60 %
D. 60 - 75%
E. more than 75%
|
E
ANZCA Pain book:
• Significant relief of PDPH was obtained in 93% of patients who received a mean EBP volume of 23 (+/-5) mL
Post-dural puncture headache: pathogenesis, prevention, and treatment - BJA 91 (5): 718-29 (2003)
• “The technique has a success rate of 70–98% if carried out more than 24 h after the dural puncture."
|
|
|
133. Pneumoperitoneum to pressure greater than 10 mmHg for laparoscopic surgery usually results in
A. a decreased arterial to end-tidal CO2 difference
B. a decrease in airway resistance
C. an increase in pulmonary compliance
D. an increase in physiological dead space
E. an increase in functional residual capacity (FRC)
|
|
|
|
134. During laparoscopic surgery, pneumoperitoneum usually results in a fall in systemic blood pressure when intra-abdominal pressure exceeds
A. 5 mmHg
B. 10 mmHg
C. 20 mmHg
D. 30 mmHg
E. 40 mmHg
|
C
From CEACCP Volume 4 Number 4 2004 - Laparoscopic abdominal surgery:
|
|
|
135. A number of drugs may reduce the incidence of perioperative cardiac complications in high risk patients when initiated preoperatively and used in the perioperative period. Evidence for this is strongest for
A. alpha-2 adrenoreceptor antagonists
B. aspirin
C. calcium channel antagonists
D. nitrates
E. statins
|
E
Stevens et al. Pharmacological myocardial protection in patients undergoing noncardiac surgery: a quantitative systematic review Anesthesia and Analgesia, 2003; 97:623-33
• “Current evidence supports the use of aspirin, statin, and angiotensin converting enzyme inhibitor therapy. There is also compelling evidence to support the use of beta-blockers, especially in patients who have recently sustained a myocardial infarction, or have heart failure”
• “Recently, it has been suggested that statins may have a role in preventing perioperative events. In a case control study, the perioperative mortality of patients undergoing vascular surgery was reduced in those receiving statin therapy. This benefit was substantial with an adjusted odds ratio for perioperative mortality among statin users as compared with non-users of 0.22 (95% confidence interval 0.10±0.47). This intriguing finding needs to be assessed in a prospective randomized controlled trial. However, all patients with vascular disease should be established on a statin, given the powerful evidence provided by the Heart Protection Study, and statin therapy may be even more critical in the perioperative period."
|
|
|
136. Regarding sampling blood for elevated histamine and mast cell tryptase (−tryptaselevels to confirm a possible anaphylactic reaction, which of the following statements is INCORRECT?
A. a sample for histamine can be taken up to two hours after the event
B. a sample for tryptase can be taken up to six hours after the event
C. a sample for tryptase can be taken up to two days after fatal anaphylaxis
D. tryptase levels can be elevated after amniotic fluid embolism
E. tryptase levels can be normal after clinical anaphylaxis
|
A
Mast cell tryptase: a review of its physiology and clinical significance. Anaesthesia, Volume 59, Issue 7 (p 695-703):
• “b-Tryptase levels peak at 15–120 min and with a half-life of 1.5–2.5 h, whereas histamine levels peak at 5 min and decrease to baseline within 15–30 min”
• “b-Tryptase testing can be performed on blood samples obtained 1–6 h after the onset of the reaction, compared with 15 min for histamine.
• “ High tryptase concentrations can be found in serum obtained from patients up to 3 days after death from suspected anaphylaxis”
|
|
|
138. Muscles which abduct the vocal cords include the
A. aryepiglottic
B. cricothyroid
C. lateral cricoarytenoid
D. posterior cricoarytenoid
E. thyroarytenoid
|
D
From Anatomy for Anaesthetists:
"The posterior cricoarytenoid muscle arises from the posterior surface of the lamina of the cricoid and is inserted into the posterior aspect of the muscular process of the arytenoid. It abducts the cord by external rotation of the arytenoid and thus opens the glottis; it is the only muscle to do so."
|
|
|
139. Phosphate-containing bowel preparations for colonoscopy are contra-indicated in frail, elderly patients because of the
A. frequent nausea, bloating and abdominal pain
B. risk of hypercalcaemia
C. risk of hypokalaemia
D. risk of hypomagnesaemia
E. risk of large fluid shifts
|
E
Australian Prescriber. 2005;28:16-7
"Phosphate preparations have the potential to cause electrolyte disturbances including serious hyperphosphataemia and hypocalcaemia; deaths have been reported. Sodium phosphate must therefore be avoided in patients with impaired renal function and used with great care in the presence of congestive cardiac failure because of the potential large fluid shifts. The frail, elderly and the very young are particularly at risk of fluid and electrolyte complications and alternative preparations should be used."
|
|
|
140. Intravenous paracetamol
A. has a volume of distribution of 10 l.kg-1
B. is excreted 20% unchanged
C. is highly protein bound
D. is mainly excreted in the gut
E. results in similar late plasma concentrations as oral paracetamol
|
E
A – false. Vd reported as 1 l/kg
B – false. 3-5% unchanged.
C – false. Not extensively bound to plasma proteins.
D – false. Hepatic metabolism with mainly renal excretion of metabolites.
E – true. Only evidence was in MIMS but they compared 500 mg oral paracetamol with 1 g IV paracetamol with similar plasma levels at 24 hours, and only in 12 adult subjects
|
|
|
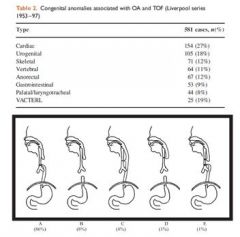
141. Tracheo-oesophageal Fistula (TOF)
A. is associated with cardiac anomalies in approximately 60% of cases
B. is associated with oesophageal atresia in approximately 20% of cases
C. is more common in males than females
D. is usually left sided
E. does not usually require contrast studies for diagnosis
|
E
• A - False. From Stoelting AACD: "Approximately 20% of neonates with EA have major co-existing cardiovascular anomalies (ventricular septal defect, tetralogy of Fallot, coarctation of the aorta, atrial septal defect), and 30% to 40% are born before term." and from CEACCP- 27%:
• B - False. Much higher. From CEACCP: "Approximately 4% of patients with TOF do not have OA."
• C - False. 1:1
• D - False. Oesophagus is on the right
• E - True. Emedicine: "Contrast studies are seldom required to confirm the diagnosis. These studies have the risk of aspiration pneumonitis and pulmonary injury, and they add minimal information to the diagnostic workup."
|
|
|
142. With regard to accidental electrocution, which of the following statements is true?
A. all electrical equipment in the operating room should be earthed
B. risk of ventricular fibrillation increases with increasing current frequency
C. risk of ventricular fibrillation is greater with alternating current (cf. direct)
D. risk of electrocution is reduced by earthing the patient
E. use of battery operated equipment avoids the risk of ventricular fibrillation
|
C
Electrical safety in the operating theatre. British Journal of Anaesthesia | CEPD Reviews | Volume 3 Number 1 [p10–14] 2003
A – false – attempt to not earth with isolated power supply
B – False – decreases eg diathermy 200kHz – 6Mhz has virtually no chance of VF (50hz dangerous)
C – true – hence use battery packs (also SELV specifies <25V AC and <60V DC)
D – false – see A (if earth patient then allows alternate passage of current through patient to ground)
E – false – “Class III equipment provides protection against electric shock by using voltages no higher than safety extra low voltage (SELV). SELV is defined as a voltage not > 25 V AC or 60 V DC. In practice, such equipment is either battery operated or supplied by a SELV transformer.It is unlikely that these voltages will cause electrocution. However, the danger of microshock persists and the latest standards relating to medical electrical equipment do not recognise Class III, since limitation of voltage alone is not sufficient to ensure the safety of patients.”
|
|
|
143. Pneumonia in children
A. if staphylococcal, is commonly associated with a pleural effusion
B. is commonly caused by mycoplasma pneumoniae in young children
C. is most commonly caused by streptococcus pneumoniae
D. is rarely caused by chlamydia trachomatis in neonates
E. often presents as lethargy without fever or cough
|
C
RCH Paediatric handbook 8th edition published 2009
Aetiology
• Respiratory viruses are the most common cause of pneumonia in young infants in developed countries. There is generally only mild to moderate constitutional disturbance. There may be scattered inspiratory crackles on auscultation.
• Mycoplasma pneumoniae is the most common pathogen in children >5 years old and is an under-recognised cause of pneumonia in younger children. Typically symptoms develop over several days before the cough, often with a systemic illness. Cough is prominent and crackles may be focal or widespread. Children are usually unwell, may have headache and focal signs are present in the chest.
• Streptococcus pneumoniae is the most common bacterial pathogen in all age groups, followed by non-typeable Haemophilus influenzae and Staphylococcus aureus. Group A β-haemolytic streptococcus is less common but may cause severe pneumonia. Many older children can be managed at home, but most <24 months should be admitted to hospital.
|
|
|
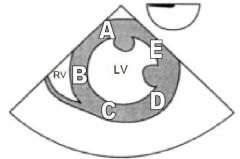
144. The diagram below is of a transgastric short axis view obtained during a transoesophageal echocardiography examination. Which letter corresponds to the area supplied by the right coronary artery?
A. A
B. B
C. C
D. D
E. E
|
|
|
|
145. With regards to obstructive sleep apnoea (OSA), which of the following statements is INCORRECT?
A. hypoxaemia is the main stimulus to arousal
B. the main method of treating this syndrome is with Continuous Positive Airway Pressure (CPAP)
C. this syndrome is the most likely diagnosis in patients presenting with excessive daytime sleepiness
D. this syndrome occurs in up to 5% of adults
E. this syndrome rarely has an obstructive component
|
E
85% have an obstructive component; 10% have a central component; 5% have mixed
|
|
|
146. Regarding postoperative nausea and vomiting (PONV), it has been demonstrated that
A. a repeat dose of a 5HT3 antagonist is useful if an initial prophylactic dose was not successful
B. dexamethasone is best given at the end of surgery
C. metoclopramide is effective for PONV prophylaxis
D. 5HT3 antagonists are best given at the beginning of surgery
E. the efficacy of droperidol is equivalent to ondansetron for PONV prophylaxis
|
E
Prevention of PONV – Annals of Pharmacotherapy Jan 2007 p 68-78
A – false. ‘Patients who have already received 5-HT3 receptor antagonists for prophylaxis should receive an agent from another class for treatment’
B – false. given at start of surgery
C – false. as efficacious as ondansetron in prevention of nausea, but not vomiting. Less effective than droperidol in prevention of both nausea and vomiting
D – false. best given towards end of surgery
E – true.
|
|
|
147. Serotonin syndrome may be appropriately managed with each of the following EXCEPT
A. bromocryptine
B. chlorpromazine
C. cyproheptadine
D. diazepam
E. non-depolarizing neuromuscular blockers
|
A
Anaesth Intensive Care 2005; 33: 181-187 - Serotonin Syndrome and the Anaesthetist
A. False. Bromocriptine is a DA agonist, therefore will worsen serotonergic syndrome.
B. Chlorpromazine has anti-DA and anti-5HT effects, therefore is helpful.
C. Cyproheptadine has anti-H and anti-5HT effects, therefore also helpful.
D. Diazepam and
E. NMB's are useful for symptomatic relief.
|
|
|
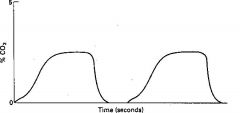
148. The capnograph below was recorded from a 70 kg anaesthetised patient , being ventilated via a circle system. The fresh gas flow into the circuit was 6 l.min-1. The tracing is consistent with each of the following EXCEPT
A. bronchospasm
B. decreased carbon dioxide production
C. high minute volume ventilation
D. hypotension
E. leaks in the side arm sampling tube
|
E
Leak in sidearm = characteristic double plateau for this –
Others are vaguely right
Good list of various capnography situations:
http://www.capnography.com/find.htm
|
|
|
149. Cauda equina syndrome
A. involves large sensory fibres initially
B. is not associated with back pain
C. results from compression of nerve roots
D. results in loss of sensation confined to the foot
E. results predominantly in an upper motor neuron lesion
|
C
A - False: Usually affects small nerve fibres first, ie autonomic nerves
B - False: Is characteristically associated with low back pain.
C - True: Spinal cord finishes at L1-2
D - False: Nerve root distribution, mostly saddle/perineal anaesthesia
E - False: LMN Lesion.
|
|
|
150. The most correct statement concerning the respiratory changes of morbid obesity is that
A. alveolar hypoventilation is characteristic of Pickwickian obesity
B. the functional residual capacity (FRC) is unchanged
C. the residual volume (RV) is decreased
D. the weight of the torso is responsible for increased chest wall compliance
E. the work of breathing is unchanged
|
A
Pickwickian syndrome = obesity hypoventilation
Characterised by obesity, hypersomnolence, hypoxia, hypercapnia, RV failure and polycythaemia
|