Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
52 Cards in this Set
- Front
- Back
|
Background - differculty with perception
|
Cons,pa,on means different things to different people
Arises when the pa,ent experiences a reduc,on in their normal bowel habit accompanied with more difficult defeca,on and/or hard stools Many people believe that anything other than 1 bowel movement per day is abnormal |
|
|
rome criteria for constipation
|

|
|
|
Prevalence & Epidemiology
|
Common symptom affec,ng between 2‐27% of the Western popula,on
Occurs in all age groups, especially the elderly: 25‐40% of people > 65 years have cons,pa,on May have normal bowel frequency but strain at stool Probably a result of a sedentary lifestyle, decreased fluid intake, poor nutri,on, avoidance of fibrous foods and chronic illness Women are 3 ,mes more likely to suffer from constipation as men |
|
|
Aetiology
|
Intes,nal transit ,me is increased, allowing greater water absorp,on from
the large intes,ne leading to harder stools that are more difficult to pass Frequently caused by a deficiency in dietary fibre, a change in lifestyle and/or environment and medica,on Patients may also ignore the defecatory reflex due to inconvenience |
|
|
History Taking - need to know
|
Details of bowel habit:
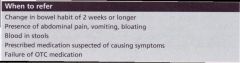
Normal bowel func,on may result in 3 movements per day to 3 per week Any change in bowel habit is important, par,cularly if prolonged Associated symptoms: OYen associated with abdominal discomfort, bloa,ng and nausea May be severe enough to obstruct the bowel Results in abdominal pain, disten,on and vomi,ng Urgent referral Other causes may include bowel tumour or twisted bowel |
|
|
History Taking need to know 2
|
Presence of blood in stool:
Not necessarily serious May arise from haemorrhoids or anal fissure OYen caused by cons,pa,on Characteris,cally noted on toilet paper aYer defeca,on May also cause discomfort of defeca,on Medical referral is required if blood is mixed in with the stool or if it appears par,ally digested (black, coffee ground appearance) |
|
|
history taking need to know 3
|
Bowel cancer:
May also present with a persistent change in bowel habit Early diagnosis and interven,on can drama,cally improve the prognosis Incidence rises steeply with age; uncommon < 50 years Average age at diagnosis is 60‐65 year |
|
|
History Taking - need to know 4
|
Diet:
Insufficient dietary fibre is a common cause of cons,pa,on An impression of fibre content of the diet can be obtained by asking what would normally be eaten during the day: Presence of wholemeal cereals, bread, fresh fruit and vegetables Changes in diet and lifestyle may result in cons,pa,on An inadequate intake of food and fluids, e.g. during illness, may be responsible |
|
|
history taking - need to know 5
|
Medica,on:
One or more laxa,ves may have already been tried Refer if treatment failure Previous history of laxa,ve use: Con,nuous use may result in diarrhoea, followed by cessa,on of bowel ac,ons for 1‐2 days More laxa,ves taken etc Overuse of s,mulant laxa,ves can result in loss of muscular ac,vity in the bowel wall (atonic bowel) Many medica,ons may cause constipation |
|
|
history taking need to know 6
|
IBS:
Lower abdominal pain, alterna,ng cons,pa,on and diarrhoea is likely to indicate IBS Pregnancy: Cons,pa,on very common, especially in the 3rd trimester Displacement of the uterus against the colon, decreased mobility and iron supplementa,on all contribute Hard stools, rather than a decrease in bowel movements in the common complaint |
|
|
history taking need to know 7
|
Func,onal causes:
Common in children Not normally a result of organic disease, but stems from a trauma,c experience associated with defeca,on (e.g. unwillingness to defecate due to prior pain) Depression: Many pa,ents present with physical rather than emo,on symptoms Up to a third of pa,ents suffering from depression present with GI complaints |
|
|
history taking - need to know 8
|
Hypothyroidism:
10‐fold more common in women than men Onset of symptoms is oYen subtle May experience weight gain, lethargy, course hair, dry skin, cons,pa,on Cons,pa,on may be the main presen,ng complaint in these women |
|
|
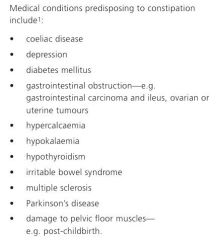
what medical condictions can cause constipation
|
|
|
|
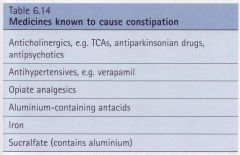
what medications can cause contipation
|
|
|
|
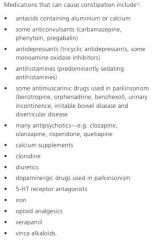
medications that can cause constipation
|
|
|
|
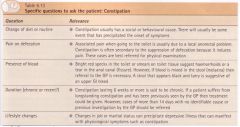
what are the main things to find out and why
|
|
|
|
when to referr
|
|
|
|
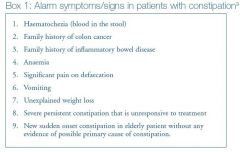
alarm symptoms of constipation
|
|
|
|
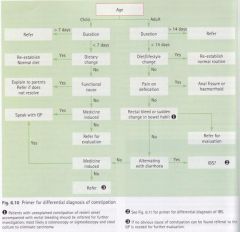
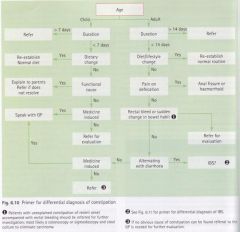
flow chart for dealing with constipation
|
|
|
|
Treatment Options
Dietary and lifestyle changes |
Usually the first step in cons,pa,on management although evidence is
limited. Should be con,nued even if laxa,ves are used: Ensure adequate dietary fibre intake (25–30 g daily is recommended in adults; increase intake gradually to avoid bloa,ng and flatulence; may be less beneficial in slow transit cons,pa,on) Ensure adequate fluid intake Increase exercise Use toilet after meals as gastrocolic reflex is maximal |
|
|
examples of fibre levels
|
|
|
|
Treatment Goals
|
Restore normal frequency
Achieve regular, comfortable bowel movements with the least number of drugs for the shortest possible time Avoid laxative dependence Relieve discomfort |
|
|
Treatment Options
Four major treatment classes:laxatives |
Bulk‐forming agents
Stimulants Osmotic laxatives Stool soYeners and lubricants Few well‐designed clinical trials Laxa,ves increase bowel movement and perform significantly better than placebo Lack of comparative efficacy |
|
|
Treatment Options
Bulking agents (unscheduled; ispaghula husk, psyllium and sterculia): |
Exert their effect by mimicking increased fibre intake, swelling in the bowel and
increasing faecal mass Insoluble (e.g. vegetables, legumes, fruits, nuts, wholegrain wheats and oats, rye meal, brown rices, seeds) and soluble (e.g. oats, barley, ispaghula, rye, vegetables, fruits) Commonly causes flatulence and abdominal disten,on Well tolerated in pregnancy Appear to have no drug interactions of note Bulking agents are useful for mild cons,pa,on, small hard stools and long term control Do not use for acute relief of cons,pa,on as they can take several days to develop their full effect Ensure adequate fluid intake (2 L per day unless unable to tolerate) to avoid intestinal obstruction |
|
|
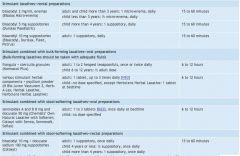
onset of bulk laxatives
|

|
|
|
Treatment Options
Stool softeners |
(unscheduled; docusate, liquid paraffin, poloxamer):
These agents soften the stool and ease its passage Liquid paraffin: Safer and more effec,ve agents are available Case reports of death caused by aspira,on of liquid paraffin leading to lipid pneumonia May also cause anal leakage and poor absorp,on of fat‐soluble vitamins Docusate: Safe for all age groups and pregnant women Free of side‐effects Docusate and poloxamer are detergents; liquid paraffin is a lubricant They are used to treat cons,pa,on (usually with a s,mulant or osmo,c laxa,ve) and to prevent straining aYer rectal surgery and in acute perianal disease They have ligle value as single agents in chronic cons,pa,on or cons,pa,on from major causes, e.g. opioid use. Stool softeners are generally given orally but can be used rectally |
|
|
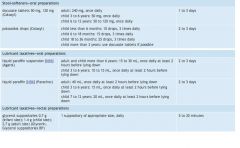
onset and summary of stool softeners
|
|
|
|
onset and summary of stool softeners
|
|
|
|
Treatment Options
Stimulant laxatives |
S,mulant laxa,ves (unscheduled; bisacodyl, senna):
Act by direct s,mula,on of nerve endings in colonic mucosa to increase intes,nal mo,lity and also cause accumula,on of water and electrolytes in the colonic lumen S,mulant laxa,ves tend to be reserved for severe cons,pa,on unresponsive to bulking agents or osmo,c laxa,ves They are usually given at night to help produce a bowel ac,on the following morning Short term use is preferred although they may be used long term in spinal damage, chronic neuromuscular disease and in people taking opioids |
|
|
summary of rectal and combo stimulant laxatives
|
|
|
|
Treatment Options
Osmotic laxatives: |
Act by retaining fluid in the bowel by osmosis or by changing the pattern of
water distribution in the faeces Glycerol can be used for rapid relief of cons,pa,on when stool is present in the lower rectum Lactulose and sorbitol need to be taken regularly They are not suitable for acute relief of constipation as they can take several days to have an effect Flatulence, abdominal pain and colic are frequently reported They can be taken by all pa,ent groups, have no drug interactions and can be taken in pregnancy |
|
|
Treatment Options
Osmotic laxatives (cont): Saline laxatives |
Saline laxatives contain poorly absorbed ions such as magnesium, phosphate,
sulphate and citrate They have a fast onset of ac,on and are suitable for occasional use when rapid bowel evacua,on is required There is a risk of electrolyte disturbance par,cularly in the elderly, children and patients with renal impairment or cardiovascular disease |
|
|
Bowel Prepara7on
Bowel preparation for surgery (S3): |
Contain polyethylene glycol (ColonLYTELY®, Glycoprep®, Glycoprep‐C®)
Saline laxa,ves (Fleet Phospho‐Soda Buffered Saline Laxa,ve Mixture®, Picolax®, PicoPrep®) Complete bowel clearance prior to surgery Risk of electrolyte disturbance and dehydra,on with all saline laxa,ves Fluid and electrolyte disturbances are less of a risk with PEG laxa,ves than with other osmo,c laxa,ves (e.g. saline laxa,ves) Counselling: Do not eat from 1–2 hours before star,ng prepara,on un,l aYer procedure performed; clear fluids are permiged; expect diarrhoea usually after about 1 hour and a clear water‐like discharge by 4 hours |
|
|
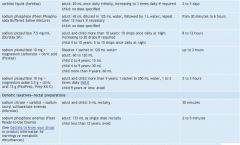
summary of osmotic laxatives
|

|
|
|
summary of osmotic laxatives 2
|
|
|
|
Management Strategies - what aprroach to treatment, evidence
|
There is insufficient evidence to assess the rela,ve effec,veness or
tolerability of laxa,ves Drug choice may be based on symptoms, required onset of ac,on, pa,ent preference, adverse effects, effec,veness of previous treatments and cost A stepped approach can also be used If lifestyle and dietary changes are ineffec,ve, a bulking agent or osmo,c laxative may be tried first with stimulant laxatives reserved as a second line option |
|
|
Pregnancy
|
Dietary and lifestyle changes are preferred
Bulking agents may be given to supplement fibre intake Docusate, lactulose and sorbitol are also safe to use Avoid stimulant laxatives (except for occasional doses) and polyethylene glycol laxatives |
|
|
Opioid Treatment
|
Cons,pa,on is the most troublesome adverse effect of opioid analgesia,
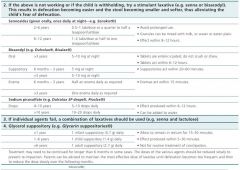
occurring in 95% of pa,ents The effect is dose‐related, but it can be prevented by the regular use of laxatives Commence regular laxa,ve protocol on ini,a,on of opioid analgesia Administer (strictly) docusate with senna, 1–2 tablets twice daily Encourage mobilisa,on, fluids Increase dose of docusate with senna if necessary up to 2 tablets three to four ,mes daily For persistent cons,pa,on, add alternate‐day glycerin suppository or disposable enema Alterna,vely, reduce docusate with senna dose by half and add sorbitol solution 70% 20 mL three times daily (an osmotic laxative) |
|
|
Contipation in Children
|
Reassure parents that some irregularity is normal and cons,pa,on is likely
to improve with age Psychological factors are important, e.g. fear of previous treatments for cons,pa,on, pain from anal problems Most cases will resolve with simple interven,ons Ensure regular toilet habits (use encouragement/rewards to improve compliance) and adequate intake of dietary fibre and fluids Laxatives are useful when children are unable to comply with regular toileting |
|
|
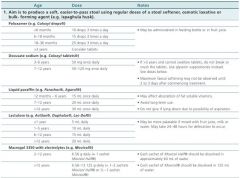
doses of constipation in children
|
|
|
|
summary of laxatives in children - if 1st line not working
|
|
|
|
Treatment Points
|
Except for opioid‐induced cons,pa,on, reserve treatment for pa,ents
who do not respond to simple measures such as increasing dietary fibre and fluid intake Long term laxa,ve use is not necessary unless cons,pa,on or faecal impac,on is likely to recur, e.g. opioid‐induced cons,pa,on, immobility due to old age or illness, and in some children to prevent relapse Some OTC combina,on products contain herbal ingredients, most of which act as stimulants; avoid long term use |
|
|
Laxative Abuse
|
Prolonged use of laxa,ves is very common in the community
Once the bowel is clear, most pa,ents should be able to avoid cons,pa,on by following the dietary and lifestyle measures However, a minority require laxatives to maintain an acceptable bowel habit S,mulant laxa,ves can cause hypokalaemia Excessive or inappropriate use of other types of laxa,ves can also result in hypokalaemia, and may be a feature of ea,ng disorder syndromes (e.g. anorexia and bulimia) Some proprietary laxa,ves are labelled inappropriately to suggest they promote weight loss May cause colonic inertia Structural or funti,onal nerve damage |
|
|
Constipation in the Elderly
|
20% of aged people living in the community
50% of aged people living in aged care facili,es Mainly due to chronic cons,pa,on Review of laxa,ves in the elderly failed to determine superior clinical efficacy between classes |
|
|
flow chart of constipation management
|

|
|
|
onset and summary of laxatives
|

|
|
|
shelf talker
|
|
|
|
Treatment‐Related Questions
Pregnancy and breast feeding: |
S,mulant laxa,ves such as senna and bisocodyl are ADEC category A
Phenolphthalein is ADEC B2 and is not recommended Fibre supplements, stool soYeners, osmo,c laxa,ves and glycerol suppositories are all considered safe in pregnancy Laxa,ves are safe to take while breast feeding if taken at the recommended dose |
|
|
Treatment‐Related Questions - surgery, elderly, heart liver problems
|
Recent surgery:
Adhesions aYer surgery can cause cons,pa,on, medical referral is required Inac,vity aYer surgery and the effects of anaesthe,cs and opioids may be a cause Elderly: More suscep,ble to electrolyte disturbance Sodium and magnesium containing laxatives should be used with caution Heart of kidney problems: Electrolyte disturbances |
|
|
practive points on laxatives
|
|
|
|
self care
|

|
|
|
self care 2
|

|