![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
Most common sites of lumbar disk herniation
|
L4-L5 L5-S1
|
|
|
Most common pattern of lumbar disk herniation |
Posterolateral disk herniation causing asymmetrical nerve root symptoms |
|
|
Spondylolithesis |
Slippage of one vertebral body relative to another |
|
|
Spondylolysis
|
Bilateral pars interarticularis defect
Can lead to vertebral slippage |
|
|
Spondylytis |
Osteomyelitis of the axial skeleton |
|
|
Malignancies most likely for bony metastisis |
Breast Lung Prostate Thyroid Kidney Lymphoma |
|
|
Roses recommended back pain Questions |

|
|
|
Red flag back pain diagnosis |
Cauda equina Spinal fractures Spinal malignancy Spinal infection |
|
|
L3 Radiculopathy
Stress test Sensation Reflex Strength |
Stress test: Reverse Straight leg raise Sensation: Medial thigh Reflex: - Strength: Hip flexion |
|
|
L4 Radiculopathy
Stress test Sensation Reflex Strength |
Stress test: Reverse Straight leg raise
Sensation: Medial foot Reflex: Patellar Strength: Knee extension |
|
|
L5 Radiculopathy
Stress test Sensation Reflex Strength |
Stress test: Straight leg raise Sensation: Between 1st and 2nd web space Reflex: - Strength: Big toe/ankle dorsiflexion |
|
|
S1 Radiculopathy
Stress test Sensation Reflex Strength |
Stress test: Straight leg raise Sensation: Lateral foot Reflex: Achilles Strength: Ankle plantar flexion |
|
|
Spinal stenosis/pesudoclaudication |
Chronic low back pain and leg radiculopathy Occurs with walking (especially downhill) and relieved by rest and sitting forward after about 15 minutes |
|
|
Anklyosing spondylitis |
Consider in younger patients with back pain, morning stiffness that improves with exercise |
|
|
At risk of cauda equina syndrome |
- bilateral radicular pain - bilateral sensory disturbance - bilateral motor weakness - bilateral loss of reflexes |
|
|
Incomplete cauda equina syndrome |
- subjective and/or objective evidence
- impaired urethral sensation, impaired rectal sensation
- objective genital/peri-anal (S3–S5) sensory
- must still have normal bladder function |
|
|
Complete cauda equina syndrome |
bladder becomes paralysed and this leads to painless retention of urine with overflow incontinence |
|
|
Most consistent physical exam finding in cauda equina syndrom |
Urinary retention (PVR >100 ml) |
|
|
Patients at risk for spinal infections |
IVDU Immunocompromised Elderly Hx of blunt trauma to back Indwelling Foley catheter Recent dental GI/GU/Spinal instrumentation |
|
|
Most common organism for spinal infection |
S Aureus
GNB, TB, and pseudomonas and IVDU also possibilities |
|
|
Risk factors for malignancy back pain |
Older than 50 Worse at night Known history of cancer elevated ESR Hematocrit <30 Clincal gestalt |
|
|
Grading spondyolithesis |
I: 0-25% II: 25-50% III: 50-75% IV: >75% |
|
|
Indications for plain films in patients with low back paon |
• Age younger than 18 or older than 50 years
|
|
|
Plain film findings of spondylitis |
erosion of contiguous vertebral endplates and a shortened disk space height, best seen on the lateral view |
|
|
Bladder volume estimation on U/S
|
Length X Width X Height X 0.52
|
|
|
Rosens DDx Low Back Pain |

|
|
|
Spinal stenosis - potential surgical indications |
- progressive neurologic deficit - progressive reduction in ability to walk secondary to pseudoclaudication - evidence of cauda equina syndrome - intractable pain |
|
|
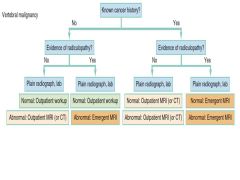
Approach to w/u query vertebral malignancy |
|
|
|
DDx of thoracic back pain |
• Uncomplicated musculoskeletal back pain
|
|
|
Hall Back pain syndromes
|
1: Back pain dominant, flexion exacerbated
2: Back dominant, no flexion component, extension worsens 3: Leg dominant, worse with flexion "sciatica" 4: Leg dominant, worse with extension/walking better with flexion "claudication" |