![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
45 Cards in this Set
- Front
- Back
|
What are the 7 components of an ophthalmic examination? |
1. anterior segment evaluation (cornea, anterior chamber, iris, lens) 2. confrontational visual fields (CVF) 3. extraocular motility (EOM) 4. fundus examination (vitreous, retina, optic nerve) 5. intraocular pressure (IOP) 6. pupils 7. visual acuity |
|
|
What are the 5 components of a directed patient history for an eye exam? |
1. hereditary eye disorders 2. medical diseases that commonly affect the visual system 3. patient ocular history 4. current eye complaints 5. associated systemic symptoms |
|
|
What are some hereditary eye disorder examples? |
high refractive error strabismus glaucoma retinal detachment |
|
|
What are some examples of medical diseases that commonly affect the visual system? |
diabetes, hypertension, autoimmune disease, neurologic disorders |
|
|
What are some things you may look for in the patient ocular history? |
glasses, strabismus (lazy eye), eye trauma, eye surgery |
|
|
What are some current eye complaints you may hear while taking the directed patient history? |
blurred vision, double vision (diplopia), visual field loss, pain/redness *timing: acute, chronic, intermittent |
|
|
What are some associated systemic symptoms you may need to take note of during the directed patient history? |
fever, headache, nausea, vomiting |
|
|
What is the Snellen Distance Acuity Chart? |
used for monocular testing with good occlusion of other eye |
|
|
When is the Snellen Distance Acuity Chart most accurate? |
when measured at 20 feet (or 6 m) |
|
|
In the Snellen Acuity system, S = ? |
greatest distance a patient can read a given line (numerator) greatest distance a normal observer can read a given line (denominator) |
|
|
In regards to Snellen Acuity, the numerator by convention is what? Why? |
-numerator = 20 -by convention, patient is 20 feet from chart |
|
|
20/60 visual acuity means what? |
that the patient needs to be 20 feet form the chart to view the letter size that a normal person can see at 60 feet |
|
|
How can you measure visual acuity in children? (if cannot read letters yet) |
use picture chart |
|
|
How can you measure visual acuity in bed-ridden, disabled, or hospital exam visits? |
use near chart held at 14 inches |
|
|
What should you ALWAYS do when measuring visual acuity? |
Make sure the patient is wearing his or her glasses!!! |
|
|
If a patient is unable to read letters (literally cannot see them) to measure visual acuity, what are the 4 next steps you would take? |
1. CF = count finger 2. HM = hand motion 3. LP = light perception 4. NLP = no light perception |
|
|
Slit lamp biomicroscopy (Haag-Streit Slit Lamp) (think where you rest your chin at the optometrist's office) provides a magnified view of what ocular structures? |
cornea, anterior chamber, iris, lens |
|
|
What type of lens is used to view the anterior chamber angle? |
Gonioscopy lens |
|
|
What should you do prior to pupil dilation with mydriatic eye drops? |
assess anterior chamber depth with a penlight |
|
|
Dilation of a patient's pupil with a shallow AC may lead to what? |
close angle glaucoma |
|
|
What eyedrops are used for pupil dilation? (2 different types & examples of each) |
1. Mydriatics/Parasympatholytics -atropine -cyclopentolate -tropicamide 2. Sympathomimetics -phenylephrine |
|
|
What is the difference in appearance for a shallow vs. deep AC angle? |
-shallow = iris only partially illuminated by pen light -deep = iris fully illuminated by pen light |
|
|
What is indirect ophthalmoscopy? |
use binocular light source/lens (head piece) and special hand held lens to manually observe the retina (instead of using a machine) |
|
|
What is the field of perception of the eye with the gaze directed straight ahead (eye focused at one point)? |
visual field |
|
|
What are the steps for testing confrontation visual fields? |
1. Examiner/patientone meter apart
2. Examiner/patientfocus on other’s eye while covering opposite eye 3. Examiner bringsobject in from all four quadrants 4. Assessespatient’s field of vision compared to examiner’s |
|
|
What does confrontation visual field screening test for? |
gross defects such as hemianopia and quadrantanopia |
|
|
What does the "kinetics" of the Goldmann Visual Fields test refer to? |
moving points of light of different size/luminance |
|
|
What are the advantages of the Goldmann Visual Fields test? |
-requires good patient/examiner interaction -good for elderly or easily distracted patients, such as children |
|
|
What do you use to administer a Static Visual Field test? |
computerized equipment |
|
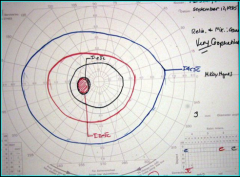
What type of test was administered? What does the outside blue ring represent? The red and black (inner) rings? Which eye is this and how do you know? |
-Goldmann Visual Fields test -outside ring = where patient can see a large, bright target -smaller rings = smaller, darker objects -patient's left eye as if they were looking forward; optic nerve comes in medially, blind spot is then somewhat temporally located (solid circle) |
|
|
What is the test in which a patient monocularly view stationary points of light, with increased light intensity, until it is perceived? |
Static Visual Fields |
|
|
What is the difference in a Static Visual Field Test and a Goldmann Visual Field Test? |
-Static = good for testing in detail a small area of visual field -Goldmann = good for testing entire broad visual field |
|
|
What do the results of a Static Visual Field test look like? |
grayscale representation that is similar to Goldmann's but a little different (many dots) |
|
|
What are the three large categories of clinical visual pathway disorders? |
1. pre-chiasmal 2. chiasmal 3. retrochiasmal |
|
|
Where could the problems be located in a retrochiasmal visual pathway disorder? |
-optic tract/lateral geniculate body -optic radiations -visual cortex |
|
|
A pre-chiasmal visual pathway disorder means what is likely affected? |
the optic nerve |
|
|
What is the impact on vision of a pre-chiasmal clinical visual pathway disorder? |
-ipsilateral vision/visual field loss -typically respect the horizontal midline -scotoma or enlarged blind spot may be present |
|
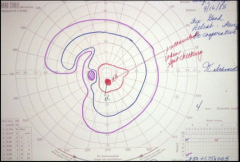
What type of visual pathway disorder does this represent? |
pre-chiasmal (optic nerve) |
|
|
What is the characteristic visual field (VF) loss for a chiasmal lesion? |
bilateral temporal hemianopia |
|
|
The specific location of a chiasmal injury may lead to what type of VF loss? |
unilateral VF oss or quadrantanopia |
|
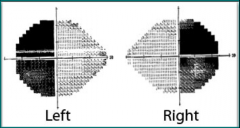
What type of VF loss does this represent? What is that characteristic of lesion wise? |
-bilateral temporal hemianopia -chiasmal lesions |
|
|
What type of chiasmal lesion will arise from below the chasm and compress inferonasal fibers first, leading to bilateral superotemporal hemianopia?
|
pituitary tumors |
|
|
What type of chiasmal lesion will arise from Rathke's pouch, compressing superior/posterior chasm first, and leading to bilateral inferotemporal hemianopia?
|
craniopharyngiomas |
|
|
What type of chiasmal lesion will lead to lateral compression of chiasm (ipsilateral nasal hemianopia), and with furtherenlargement may develop contralateral compression and binasal hemianopia?
|
internal carotid artery aneurysm |
|
|
What type of VF defect is caused by a retrochiasmal lesion? What happens the more posteriorly located the lesion is? |
-homonymous VF defect that respects the vertical midline -more posterior = more congruous the field loss |