![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
Objectives
|
|
|
|
note: exception to the rule. which metastatic cancers can be cured
|
1. testicular
2. ewing's sarcoma 3. gestational trophoblastic neoplasia |
|
|
general principle of chemotherapy...
1. which cells are hit 2. and which systems typically have side fx (3) |
|
|
|
general principles chemotx continued..
|
•Mostagents don’t kill the cell directly
•Createirreparable damage to vital structures (DNA, RNA, critical proteins) •Cellcan’t fix itself and as such dies •Apoptosis: programmed cell death –Thecell recognizes it has an unfixable problem and has a lethal injury –Itdies rather than propagate the injury |
|
|
apparently "nobody will ever ask you how any chemotherapy drug works"
|
k
|
|
|
akylating agents
1. examples 2 2. mech |
|
|
|
platinum analogues
1. examples 2. mech |
|
|
|
antimetabolites
1. examples 2. mech |
|
|
|
topoisomerase II inhibitors
1. examples. 2. mech |
|
|
|
antimicrotubule agents
1. examples 2. mech |
|
|
|
basic principle of chemotherapy dosing |
given cyclically so that normal tissues have time to recover. |
|
|
chemotherapy: explain how "proportion of cells" are killed each cycle |
|
|
|
how much of a kill is expected per cycle? |
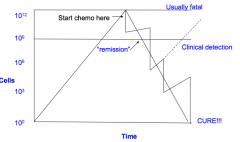
2-3 log kill |
|
|
problem of drug resistance in cancer cells... |
•Cancercells have the ability to rapidly adapt to the stresses placed on them by thechemo •Theyfind ways to circumvent the drug and become resistant •Ifnot all cancer cells are killed quickly, remaining cells become resistant andmore difficult to kill |
|
|
general approach to drug resistance in cancer cells |
basically, anything that limits contact time with cellular DNA. |
|
|
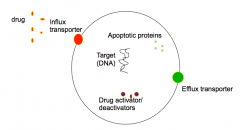
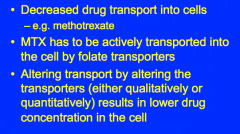
mechanisms of resistance; decresased transport into cells |
|
|
|
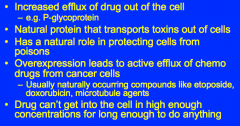
mechanisms of resistance; increased efflux |
|
|
|
mechanisms of resistance; impaired drug activation |
|
|
|
mechanisms of resistance; accelerated inactivation |
|
|
|
mechanisms of resistance; modification of cellular targets |
|
|
|
mechanisms of resistance; impaired cell death pathways |
|
|
|
how do we preevnt resistance 3 |
1. kill all the cells as rapidly as possible 2. multi-agenet combination 3. treat cancer when there are the fewest number of cells (less chance of resistance, fewer cells to kill to get that cure) |
|
|
Hormone therapy: % of male and female cancers (prostate, breast, endometrial) that are hormonally sensitive |
male: 20% female 40% |
|
|
mech of hormone therapy |
•Deprivingcancer cells of a necessary growth factor causes tumourregression •Canbe used in adjuvant setting to improve cure rates "chemotherapy is poison, hormone therapy is starvation" |
|
|
when is it appropriate to consider hormone therapy? when is it unsuitable? |
|
|
|
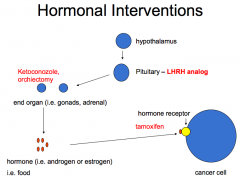
treatment strategies in hormone therapy 4 |
1. remove hormone-producing gland 2. interfere with hypothalamic-pituitary-end organ pathways 3. block hormone synthesis at end organ (eg ketoconazole in adrenal cancers blocks steroid synthessi at adrenal gland) 4. block end organ hormone receptor (eg tamoxifen for breast Ca, Bicalutamide for prostate Ca) |
|
|
examples of hormonal interventions |
|
|
|
Hormones vs. chemotherapy: onset toxicity dosing ROA |
|
|
|
How to tell which hormone receptors are expressed? |
|