![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back
|
1. A bodily sensation with qualities like those reported duringtissue‐damaging stimulation 2. An experienced threat associated with this sensation 3. A feeling of unpleasantness or other negative emotion basedon this experienced threat |
Pain - definition |
|
|
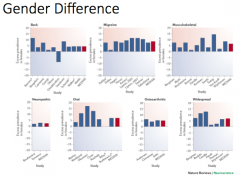
What is the gender difference in pain expression? |
|
|
|
• Pain perceptions and behavior are heavily influenced by ____ and bythe _______ (family support and expression of pain) • Pain assessment may become particularly problematic when patientsand hospital workers have differing _____ background • Pain is the ___ vital sign |
culture and sociocultural context cultural 5th |
|
|
• The 5 racial categories are American Indian or Alaskan Native, Asian, black or African American, Native Hawaiian or Other Pacific Islander, and White. • African American adults vs African American children experience in ED • Black, Hispanic, and Asian women were less likely to receive epidural analgesia than white women. |
Read it... |
|
|
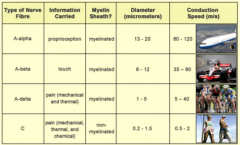
Which two types of afferents carry pain stimuli ? Relative conduction velocity? Predict Myelinated vs non-myelinated, and larger vs smaller? |
|
|
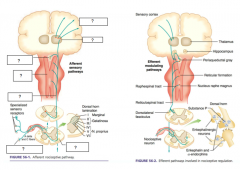
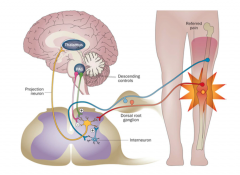
Afferent pathway |
nociceptors -> anterolateral fasciculus -> spinothalamic tract projects to -> reticular formation -> periaqueductal gray -> thalamus -> sensory cortex |
|
|
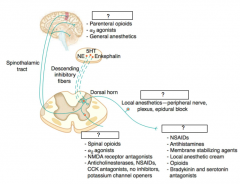
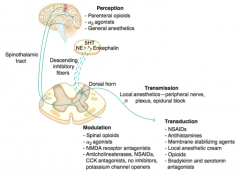
4 aspects of pain processing? |
1. Transduction 2. Transmission 3. Modulation 4. Perception |
|
|
noxious thermal, chemical, or mechanical stimuli are converted into an action potential |
1. Transduction |
|
|
action potential through 1st, 2nd and 3rd order neurons |
2. Transmission |
|
|
inhibition (by glycine and GABA) or augmentation (by norepinephrine, serotonin, and endorphins) of the afferent or efferent pain signals |
3. Modulation |
|
|
final common pathway: integration of painful input into the somatosensory and limbic cortices |
4. Perception |
|
|
|
|
|
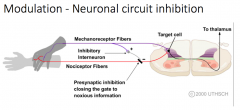
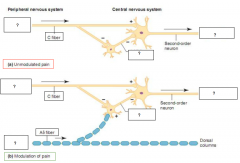
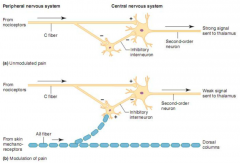
• Endogenous Opioid receptor activation • Neuronal circuit inhibition via interneurons • Central inhibition via periaqueductal gray (PAG) andnucleus raphe magnus (nRM) • Stress Induced Analgesia These are mechs of? |
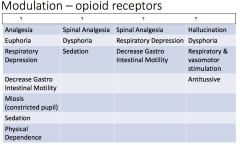
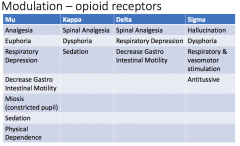
Modulation
|
|
|
This mech of modulation a) block neurotransmitter release byinhibiting Ca2+ influx into thepresynaptic terminal b) open potassium channels, which hyperpolarizes neurons and inhibitsspike activity |
Opioid receptors |
|
|
morphine (mu), ketocyclazocine (kappa), vas deferens (delta), sigma receptors These are types of what receptor family? |
Opioid receptors |
|
|
|
|
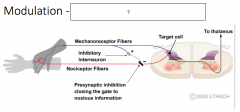
What is happening here? What mech of modulation? |
|
|
|
|
|
|
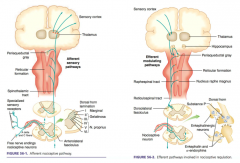
This mech of modulation occurs via stimulation produced analgesia (SPA). PAG or nRM -> inhibit spinal thalamic cells (i.e. spinal neurons that project monosynaptically to the thalamus) so that the noxious information from the nociceptors are modulated at the spinal cord level. (descending tract: dorsolateral funiculus). |

Central Inhibition |
|
|
• Delayed pain in soldiers and athletes • Flight or fight response • influenced by variables such as age, sex, degree of sensitivityto opiates, and past stressful experiences. • opioid and non‐opioid mechanisms (cannabanoid, endorphins) Mech of modulation? |
Stressed Induced Analgesia |
|
|
• noxious stimulus • tissue damage (eg, postoperative pain). • somatic pain: injury to body tissues, localizable • visceral pain. Mediated by stretch receptors. It is poorly localized, deep, dull, and cramping (eg, pain associated with appendicitis, cholecystitis, or pleurisy) Type of pain? |
Nociceptive pain |
|
|
• abnormal neural activity secondary to disease, injury, or dysfunction ofthe nervous system. It commonly persists without ongoing disease (eg,diabetic neuropathy, trigeminal neuralgia, or thalamic pain syndrome) Type of pain? |
Neuropathic |
|
|
Two types of Pathologic Pain |
Central or Peripheral Sensitization |
|

Central sensitization can cause? |

Hyperalgesia abnormally heightened sensitivity to pain. Allodynia is pain, generally on the skin, caused by something that wouldn't normally cause pain |
|
What type of pain is this? |
Pathologic; periperal sensitization |
|
|
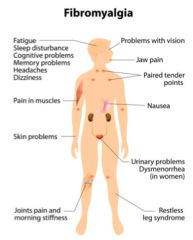
• Widespread musculoskeletal pain accompanied by fatigue,sleep, memory and mood issues • Pathology in the all 4 pain pathways (transmission, transduction, modulation, and perception) |
|
|
|
• NSAIDS (Non‐steroidal anti‐inflammatory drug) • Acetaminophen • Opiates • Ketamine Type of pain treatment? |
Pharmacological |
|
|
• Spinal • Epidural Type of pain treatment? |
Regional Anesthesia |
|
|
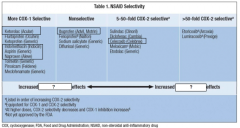
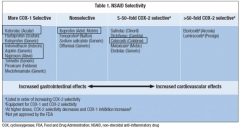
• Ketorolac • Indomethacin • Aspirin • Naproxen (Aleve) • Ibuprofen (Advil) • Celecoxib • Steroid These are what kind of drugs for treating pain? |
• NSAIDS (Non‐steroidal anti‐inflammatory drug) |
|
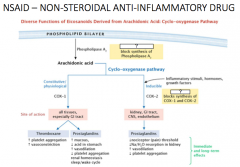
Which drug blocks: -synthesis of PLA ,inhibiting synthesis of AA? -synthesis of COX-1 (and COX-2), inhibiting synthesis of PGs? |
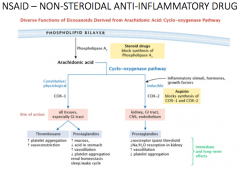
Note the site of action! |
|
|
• Ketorolac • Indomethacin • Aspirin • Naproxen (Aleve) NSAIDS + selectivity for inhibition of COX synthesis? |
COX-1 KIAN |
|
|
• Ibuprofen (Advil) NSAIDS + selectivity for inhibition of COX synthesis? |
Non-selective! |
|
|
• Celecoxib NSAIDS + selectivity for inhibition of COX synthesis? |
COX-2 • Celecoxib |
|
|
Inc COX-1 selectivity -> increase effects here |
Gastrointestinal effects |
|
|
Inc COX-2 selectivity -> increase effects here |
Cardiovascular effects |
|
|
|
|
|
Cardiovascular risk associated with this NSAID |

|
|
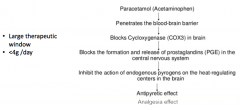
Mech of which drug? Note the window! |
Acetaminophen/paracetamol |
|
|
1. Block neurotransmitter releaseby inhibiting Ca2+ influx intothe presynaptic terminal 2. Open potassium channels,which hyperpolarizes neuronsand inhibits spike activity. Does this look familiar? Mech of which class of synthetic drug? |
Opiates NB - these are the synthetic version of the endogenous opioids |
|
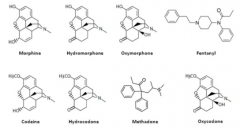
Morphine Hydromorphone Oxymorphone Fentanyl Codeine Hydrocodone Methadone Oxycodone Belong to which class of drug? |
Opiates |
|
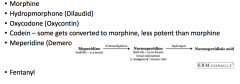
What class of drugs? |
Opiates |
|
Guess the drug! |
Fentanyl! |
|
|
• Cheap synthetic opioid • More potent • Fast acting • Takes away the pain with intubation • Unfortunately, it is a drug of abuse The drug is? |
Fentanyl! |
|
|
• Risk factors: • Alcohol Use • Age: Youth • Previous drug abuse (17X more) • 4/5 users previously used painkillers • Scare tactic advertisements prevent good pain management to those that need it Addiction to these two similar drugs? |
Heroin and Opiate addiction |