![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
161 Cards in this Set
- Front
- Back
|
Sx of pregnanacy |
- Amenorrhea - Morning sickness - Freq micturition w/o dysuria - Fatigue - Breast enlargement/tenderness - Poor sleep/back pain - Enlarged uterus on bimanual (old school) - 8/10 weeks uterus=orange size - 12 wks = fundus at pubic symphisis (if no fibroids) |
|
|
Peak of b hcg |
~9-12 days |
|
|
Beta hcg 48hr rule |
- Bhcg doubles in 48hr (increases by more than 66%) - Indicates viable preg, useful in early preg if USS not conclusive - Non doubling=>non viable (miscarriage or ectopic) - Embryo w heartbeat only definitive way to know |
|
|
Miscarriage RFs |
- 12-19% all pregs - Most common cause 45 XO chromosomal abnorm (Turner's if goes to term) - Older age >43 y/o: 51% chance - Uterine malformations - Infections: rubella, toxoplasma, CMV - Diabetes, renal, thyroid (worse w bad control) - Alcohol - Smoking - Anti phospholipid syndrome |
|
|
Pregnancy failure clues on USS |
- Mean gestational sac diametre 25mm or - CRL ≥7mm, no heart beat - Absence of embryo w heartbeat ≥2 weeks after a scan showing gest sac w/o yolk sac - Absence of embryo w heartbeat ≥11 days after a scan showing gest sac + yolk sac *These signs are conclusive regardless of sx or gestational age, no need for additional tests |
|
|
miscarriage stages |
|
|
|
Miscarriage tx, when to D&C |
- If px haemodynamically unstable + ongoing heavy bleeding - Febrile miscarriage - Incomplete miscarriage can be managed expectantly - Anti D needed if resus neg |
|
|
Miscarriage <13, natural hx |
- 52% will have completed mc in 1 wk - 85% in 2 wks - Medical/surgical tx if longer than 2 wks |
|
|
Medical miscarriage |
- Misoprotol 200mcg tablet eg. 600mcg, 12hrly x4 - PGE1 analogue=>myometrial stimulation=>contractions=>expelling products of conception - Oral or vaginal (vag preferred as less diarrhoea) - Complete miscarriage 80-91% |
|
|
D&C risks |
- Infection (low risk) - uterine perforatuon - Intrauterine adhesions (Asherman sx) - Link w preterm birth (weakened cervix from forced dilation) |
|
|
Ectopic preg RF |
- Endometriosis - Previous pelvic/tubal surgery - IUD in situ, sterilisation - Smoking - Hx infertility or IVF - Hx PID or perforated appendix - 50-70% have no RFs |
|
|
Ectopic sx s/s |
- 50% no sx except amenorrhoea + PV spotting therefore sx not too helpful - Unilateral abdo/pelvic pain - Shoulder tip pain - Urgency to open bowels=>unable to - sx of hypovolaemia - Peritonism - Speculum exam : blood - Bimanual, unilateral tenderness (risk of EP rupture) |
|
|
Ectopic preg B HCG |
- Does not rise appropriately => <66% rise in 48hrs - Ratio >0.8 (change in serum levels over 48 hrs, ie. bhcg:bhcg+48hrs)=> failed preg - BUT caution b/c bhcg can still increase |
|
|
Ectopic preg USS signs |
- Intrauterine preg should be visible on transvag USS if BCG >1500, >3500 should be vis on trans abdo, therefore use USS to confirm. 1. empty uterus in woman w pos preg test (or midline pseudosac=fluid) 2. Corpus luteum: solid mass or cyst w internal scattered echoes or thin walled cyst 3. Ectopic mass: bagel sign, w or w/o yolk sac (pathognomonic) or ring of fire on colour b/c v vascular + may have fluid (blood) in pouch of douglas or adnexa or complex mass (clot) |
|
|
Ectopic mgmt surg |
- Diagnostic laparotomy + curative salpingectomy (used to do salpingiotomy to salvage tube, but high rates of recurrent EP + comps) |
|
|
Ectopic mgmt medical |
- Methotrexate 50mg/m2 single dose IM - Ep must be <3cm, BhCG <5000, non viable preg (no embryo w heart beat), non bleeding - Compliance w f/u essential - BhCG should drop at least 15% on day 7 compared w day 4 => if not repeat MTX dose |
|
|
Ectopic preg medical mgmt f/u |
- Quantitative B-hCG levels weekly until <2IU/L, usually for 4 wks - Failure rate med tx 22% - Reliable contraception for 3 mths (MTX teratogenic and causes NT disorders) |
|
|
Gestational troph. disease/mole s/s |
- Most diagnosed before s/s - Vag bleeding: most common sx (molar tissue separating from decidua) - Distended uterus (bigger than you would expect at that gestational age): large amounts of blood, dark fluid may leak into vag (~50%) - Hypermesis: d/t v high BhCG - Hyperthyroidism: high BhCG is a TSH analogue |
|
|
Complete mole definition |
- 80% cases - Usually normal karyotype - Aetiology: duplication of single sperm + empty ovum - No foetal tissue - BhCG markedly raised - May progress to invasive more ~15% cases, choriocarcinoma in ~5% |
|
|
Partial mole |
- Aetiology: 2 sperm fertilising 1 ovum - Paternal + maternal chromosomes, triploid 69XXX or 69XXY - May contain foetus - BhCG moderately elevated |
|
|
Partial mole s/s |
- Consistent w missed abortion - Vag bleeding - Absence of foetal heart sounds - USS diagnosis difficult |
|
|
Mole tx |
- Not expectant! - Urgent D&C under USS to ensure complete removal and minimise perf risk - Histology + karyotype - F/U w serial BhCG, undetectable after ~12wks, increases w persistent trophoblastic activity=> CT chest/a/p for distant mets - Gynae onc referral - MTX or multi agent chemo |
|
|
Expected date of delivery; Naegele's rule |
EDD = 1st day LMP + 7 days + 9 mnths = 280 days after LMP (av. preg 281 days), does not account for mnths <31days therefore not perf - If cycle not 28 days, add the no. of days more than 28 to the Naegele calc (eg. if 32 day cycle do naegele + 4 b/c took 4 days longer to fert) - 90% babies born w/i 3 wks of EDD |
|
|
Antenatal screening first visit |
- Blood group - Rhesus - CBE, ferritin - Rubella titre, Hep B/C, HIV, syphilis - Vit D level if at risk - MSSU |
|
|
Antenatal screening 11-14 wks? |
- Foetal aneuploidy T21+18 |
|
|
Foetal morphology USS weeks? |
18-23 |
|
|
OGTT weeks? |
27-28 for screening Early test at 12wks offer if: - Previous GDM - Maternal age ≥40 - BMI ≥35 - Prev. baby >4.5kg or >P90 - PCOS |
|
|
Low vag swab group B strep (culture or NAAT) |
36 wks |
|
|
Rhesus neg, anti-D dosing scheme |
28 + 34 weeks and post delivery - Prophylactic deep IM 625 IU anti-D ALSO for Miscarriage, ectopic preg, TOP, antepartum haemorrhage, abdo trauma, breech - Kleihauer test can tell how much foetal Hb in mum circ and if AntiD dose enough |
|
|
Criteria for gestational DM |
Any one of: - Fasting BSL ≥5.1mmol/L - 1 hr BSL ≥10mmol/L - 2 hr BSL 8.5mmol/L For OGTT |
|
|
Asymptomatic vaginal GBS mgmt |
- IV penicillin-G 6gm during labour - If allergic to penicillin: clindamycin - Prevents early neonatal sepsis (1 in 200 of babs from pos mums) |
|
|
Trisomy 21 + 18 screening dates |
- PAPP-A (9-13 wks) if growth restriction of bub - Nuchal translucency + nasal bone check (11-13+6 weeks) - T21 detection rate 90%, false pos 5%=>detailed cardiac echo if NT >3.5mm at 18-19wks |
|
|
Second trimester screening (14+0)-(20+6) tests |
- Alpha Foeto Protein (foetal liver: spina bifida + T21 marker) *If AFP raised=>detailed morphology USS looking at brain, ventricles, spine - hCG - Uncongugated estriol t21, t18, neural tube |
|
|
5 soft markers for aneuploidy |
- Mild ventriculomegaly - Choroid plexus cyst in brain - Thickened nuchal fold - Echogenic bowel - Echogenic focus in heart |
|
|
Morphology scan things to check |
- Check for morphological probs all organs - Placental position: for placenta previa - Amniotic fluid: *anhydramnios: bilateral renal malfunction or agenesis=>potter's sx, neonatal death *ddx PPROM or leaking AF * Polyhydramnios: Gastro-oesoph fistula or swallowing difficulties |
|
|
Indications for induction of labour |
Risks of continuation preg>risks of delivery for mum+bub *mild gest HTN >39wks or preeclampsia >37wks *psychosocial;mum "fed up", convenience, planning (eg. geographical) *poor controlled gestational diabetes *PPROM w chorioamnionitis *post term preg (40+10 or 42+0) *SGA or IUGR, >37+0wks *rhesus allo-immunisation *recurrent antepartum haemorrhage/pl. abruption *chorioamnionitis *foetal malformations incompatible w life/intraterine foetal death *large for gest age >90P, less dystocia |
|
|
Contraindications for IOL |
- transverse or oblique lie=>rupture - Vasa/placental previa - Presenting umb cord - Previous transfundal uterine surgery, classical c section, myomectomy => inc rupture risk *active genital herpes=>inc risk neonatal sepsis *Cervical cancer |
|
|
IOL |
Artificial rupture of membranes + IV oxytocin |
|
|
Bishop score |
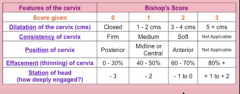
Based on digital exam |
|
|
Priming cervix for IOL |
Bishop score >8 cervix favourable, no need to prepare Bishop score 0-5: unfav, needs priming Options: *transcervical uterine balloon (single balloon on top of cervix in lower uterus or that + one below cervix=>pressure cervix=>prosta release *Prostaglandins (high in vag, close to cervix, or PGE1 oral, 50mcg 4hrly) Balloon favourable |
|
|
IOL |
- Rupture membranes =>oxytocin IV w incremental dose b/c every woman diff sensitivity - Aim for 3-4 contractions in 10mins no more! - Continuous CTG |
|
|
Contraindications to prostaglandins for cervical ripening |
- Px febrile (b/c prostas raise temp) - Active bleeding - Abnormal CTG - Bishop score ≥4 |
|
|
Risks of prostaglandin use for cervical ripening |
- Uterine hyperstimulation = uterine contractions >5 in 10mins = tachysystole + CTG changes - Uterine perf esp if LSCS scar - PG gel hard to remove *maternal side effects eg: nausea, vom, diarrhoea, fever |
|
|
Braxton Hick's |
- Irregular contractions, don't get closer together - May stop when walking, rest, change of position - Usually weak and don't get much stronger - Usually only felt in the front |
|
|
PROM |
Prelabour rupture of membranes |
|
|
PPROM |
ROM <37 wks = Preterm, prelabour rupture of membranes |
|
|
Tests for ROM |
Do not do digital vag exam because of risk of ascending infection (sterile spec exam instead) instead: - Fern test (fluid on glass=>dry=>crystallises + looks like fern under microscope) - pH test; 7-7.5= ROM (normal vag pH 4.5-6) - Immunoassay test: self collected high vag swab, testing for placental amniotic fluid (PAMG-1 (alphamicroglobulin-1)) |
|
|
Mechanism of labour pain |
- Uterine contractions=>visceral pain T10-L1 - Second stage: descent of foetal head exerts pressure on mum's pelvic floor, vag, perineum, causing somatic pain=>pudendal nerve (S2-S4) |
|
|
Active mgmt for 3rd stage delivery (placental) |
- Uterotonic drugs (oxytocin + ergometrin) - Early clamping of cord - Controlled Cord traction (no effect on PPH rates, red chance woman needs manual removal of placenta) =>less blood loss SEs: inc vom, lower abdo pain, inc diastolic BP |
|
|
Delayed cord clamping effects in infant |
- 33% higher chance of needing therapy for jaundice - Slightly Higher Hb |
|
|
RFs for PPH |
- Retained placenta - Failure to progress in 2nd stage - Placenta accreta - Lacerations - Instrumental delivery - Large for gestational age baby - Hypertensive disorders - Induction of labour - Augmentation of labour w oxytocin |
|
|
Baby blues definition, rx |
- Occurs in ~70% of women b/w day 3-5, before day 14 - Difficult adjustment b/c of life changing event - Sudden drop in placental hormones Manage: support and validation, encourage to do enjoyable activities and bond w baby |
|
|
Post natal depression |
- Adjustment disorder w depressed mood - Occurs in ~15% - Sx of major depression - Occurs <12mnths after delivery and lasts at least 14d - Aetiology: biological, fam hx, cultura, psychosoc |
|
|
PND mgmt |
- Healthy lifestyle, nutrition, brisk walk, social support - Force yourself to do pleasant activities/mindfulness every day - Coping skills Medical: - SSRIs: not much more effective than placebo - Refer to psychiatrist if MDD sx or suicidal ideation |
|
|
Mastitis, aetiology, s/s |
- Fever - Chills - tachycardia - Mastalgia - Mostly staph aureus from infant nose+throat |
|
|
Mastitis rx |
- Fluclox 500mg QID for 5 days - Maintain breastfeeding - After 78hrs of abx there should be less pain/erythema/swelling. If not =>?abscess=>uss guided drainage=>surgical incision+drainage + biopsy, could be atypical presentation of CaBreast |
|
|
Endo/myometritis |
- Fever >38 on day 2-10 - Lower abdo pain - Offensive lochia (anaerobic bacteria) - Centrally tender uterus - Raised WCC + CRP |
|
|
Endomyometritis ix+rx |
ix: cannot swab because of vaginal flora contamination rx: abx covering gram + and - and anaerobes ie triples: - Cephlasporin or augmentin duo: gram + - Gentamycin: gram neg - Metronidazole: anaerobes - IV for first 48hrs=>orals + analgesia |
|
|
antepartum haemorrhage ddx |
- Placenta praevia - Placental abruption - Incidental maternal findings eg. ectropion - Infection eg. chlamydia - Genital tumour or abraision - A "Show" - Varicosities - Vasa praevia |
|
|
Antepartum haemorrhage definition |
Bleeding ≤24 wks |
|
|
Vasa praevia definition |
- Foetal blood vessels lie inferiorly to presenting part of foetus, unprotected by any placental coverings - They begin to bleed with onset of labour/ROM - Causes rapid foetal distress/exsanguination - 33-100% mortality |
|
|
RFs for vasa praevia |
- Low lying placenta - Multiple pregnancy - IVF preg - Bilobed or succenturiate placenta |
|
|
History questions antepartum haemorrhage |
- Dates, singleton or multi - Time course - Amount of blood - Abdo pain - Iniating factors (coitus/trauma?) - Previous PV bleeds this preg? - Rhesus status + blood group - Obstetrical hx - Obstetric/abdo surgery - Infection RFs - Position of placenta if known - Leakage of PV fluid - Smoking and rec drugs esp cocaineI |
|
|
PE for antepartum haemorrhage |
- Pulse/BP/haemodynamic status - Uterus: foetal size/lie/presenting part/engagement(not PP if head is engaged) - Uterine tenderness - Remember no PV until PP excluded, then do a spec exam to look at local causes haemorrhage + PV to assess for cervical changes |
|
|
Antepartum haemorrhage foetal ax |
- Assess HR: mum may be v tachy so take care - Commence FHR monitoring if >26 wks gestation |
|
|
mgmt of placenta praevia major |
- Admit women who have previously bled from 34 wks - W who haven't make sure they are close, aware of risks and have constant companionship -Delivery by CS if placenta w/i 2cm of cervix, esp if posterior and thick |
|
|
mgmt minor antepartum haemorrhage |
- Admit for 24hrs as this is the most likely time to have a repeat bleed - Kleihauer test for isoimmunisation and AntiD if needed - FBC, group and hold serum - Coagulation panel - USS to determine foetal wellbeing/placental pos - Doppler umbilical artery as placental abruption even small can alter placental fcn - Inc. F/u before + after delivery |
|
|
Placental Abruption definition, freq |
- Part of the placenta detaches from uterus before birth - Space behind fills w blood - 25% have no PV (concealed) - 75% bleed PV - Freq. 1% all preg |
|
|
Placental abruption s/s |
- Abdo pain or back pain for posterior placenta - Pain sudden onset, constant, severe - PV bleed, often dark blood - Uterine activity common - Uterine tenderness - Uterine hardness (woody) - 50% of presentations will be in labour - Maternal signs of shock - Foetal distress=>foetal death |
|
|
Placental abruption mgmt |
- Admit - Group and hold - CTG and urgent USS - If foetal distress or maternal compromise, resuscitate and deliver - If pain desists and mother/baby stable, manage expectantly |
|
|
Oligohydramnios definition |
- Not enough amniotic fluid - Measured w USS, if deepest pool is <2cm or deepest pools in 4 quadrants add to <8 |
|
|
Oligohydramnios complications |
- Lung hypoplasia if <22 wks - If prolonged MSK abnormalities eg. talipes - Oligohydramnios <22wks has very poor prognosis - IUGR - PROM |
|
|
Oligohydramnios ix |
- USS + doppler of foetus - Speculum to ax SROM - if SROM: vag swabs, CBE, CRP should be taken |
|
|
Oligohydramnios mgmt |
- If SROM ≥34 wks=>induce unless CS indicated for another reason - If SROM <34: give erythromycin, daily CTG, 4hrly temps, monitor unti 24wks=>induce - Unless d/t IUGR, then mgmt according to umbilical doppler + USS - If isolated oligohydramnio, reconsider cause + monitor |
|
|
Oligohydramnios causes |
- Leakage of amniotic fluid: SROM - Dec. foetal urine prod: *renal issues *Post dates *IUGR - Posterior urethral valve of bub obstructing urine outlet |
|
|
Polyhydramnios definition |
- Deepest pool >8cm - AFI (combined 4 quadrant depth>22cm) |
|
|
Polyhydramnios causes |
- Inc. foetal urine prod: *maternal diabetes *twin-twin transfusion syndrome (recipient twin) *foetal hydrops - Dec. ability to swallow/absorb amniotic fluid *Facial abnormalities *Neurological or MSK probs (anencephaly, myotonic dystrophy *GI obstruction (eg. duodental atresia, tracheo-oesophageal fistula) - Idiopathic (usually mild) |
|
|
Polyhydramnios comps |
- Preterm delivery (uterine stretch) - Malpresentation b/c of inc. room to move - Abdo discomfort for mum d/t distention - Assoc. w cause eg. duodenal atresia assoc.w trisomy 21 |
|
|
Polyhydramnios mgmt/ix |
ix: USS and OGTT to exclude GDM mgmt: *If severe amnioreduction (drainage of fluid) or NSAIDs *If premature, assess risk of delivery w fibronectin, consider steroids *if twin/twin transfusion or foetal abnormality=>refer to foetal medicine centre *If malrotated=>CS **be careful of NSAIDs as can cause foetal oliguria + constrict ductus arteriosus |
|
|
IUGR importance |
More liklihood of - Stillbirth (30% SB have IUGR) - Emergency CS - Hypoglycaemia/hypocalcaemia - Cerebral palsy (4x greater risk) - Foetal distress and asphyxia - Meconium aspiration - Necrotising enterocolitis - Perinatal mortality inc. |
|
|
IUGR causes, maternal |
- Chronic disease: HTN, renal, cardiac - Autoimmune disorders eg. antiphospholipid syndrome - Congenital diseases eg. phenylketonuria - Alcohol, smoking, rec. drugs - Low SES - Poor nutrition |
|
|
IUGR causes placental (most common) |
- Placental invasion problems: *preeclampsia *accreta - Abruption - Placenta praevia - Two vessel cord, abnormal insertion - Placental infarction - Tumours eg. chorioangiomas |
|
|
Foetal IUGR causes |
- Multiple pregnancy - Trisomy 21, 18, turner's triploidy - Congenital conditions: transposition of great vessels, TOF, gastroschisis - Infection: CMV, rubella, toxoplasmosis |
|
|
symmetric vs asymmetric IUGR |
- Symmetric: equally small eg. chromosomal causes, early onset - Asymmetric: head sparing, abdo circumference + thin limbs, head normal. Last onset + placental causes (spares vital organs as defence mech) |
|
|
IUGR mgmt + outcomes |
- Surveillance until birth - 1/3rd to not reach predicted adult height, inc. risk of cardiac disease, HTN, abnormal glucose/insulin metab, high cholest in adulthood :o |
|
|
Causes of malpresentation |
- Maternal *multiparity *Pelvic tumours *Congenital uterine abnorms *Pelvic contractures - Foetal *Multiple pregnancy *Congenital abnorms (anencephaly, hydrocephaly, cystic hygroma) *Macrosomia *Intrauterine death *Prematurity - Placental: *Amniotic bands *Placenta praevia *Polyhydramnios |
|
|
Brow presentation signs and mgmt |
VE: both chin and occiput, nasal root, anterior fontanelle, frontal suture, eyes palpable - Will not progress past ischial spines mgmt: Watch and wait, may revert to face or vertex - CS if not reverted |
|
|
Face presentation signs and mgmt |
VE: mentum, orbital ridges, gums/mouth, nose can be felt mgmt: - Mentoanterior (90%): watch+wait, head can flex to allow delivery - Mentoposterior: w+w, ~25% will revert when reaching pelvic floor - If persistent=>CS - Forceps contraindicated as can cause cord prolapse/foetal cervical cord injury. Unless MA well below spines - Ventouse absolutely contraind |
|
|
Causes intrapartum haemorrhage |
- Intrapartum placental abruption - Uterine rupture - Amniotic fluid emobolism - Placenta accreta or percreta - Tears to broad or angular lig in CS, other comps of CS |
|
|
mgmt postpartum haemorrhage for Atony |
- Physical compression:rubbing up, bimanual - Medical: *ergometrineIV=>oxytocin infusion=>oxytocin IV stat=>misoprostol rectally=>carboprost myometrially x4 doses If failure to respond to above=>surgical examination + fix |
|
|
Surgical mgmt PPH |
- Rusch balloon - Repair of lacs - Oversewing of uterus - Internal iliac or uterine artery ligation/embolisation - Total (lower segment bleeding:placenta praevia, accreta or tears) or subtotal hysterectomy (quicker and safer) - Remove retained products/foetus |
|
|
GDM Rfs |
- Previous GDM - BMI >30 - Previous macrosomic baby >4.5kg - First degree relative with DM - Ethnicity with high proportion of DM (south asian, middle eastern, black carribean) 20-30% GDM just previously unrecognised T1 or 2 DM |
|
|
GDM mgmt |
- Diet and exercise first line - If fasting glucose >6.0 or 1hr post prandial >7.5 start insulin - Otherwise intrapartum mgmt the same as for established diabetes - Post partum stop insulin and glucose infusions - BSL test before d/c - OGTT at 6wks - Educate that 50% will get T2DM in the next 25yrs, avoidable with exercise + avoidance of obesity |
|
|
Amniotic Fluid Embolism definition |
Diagnosis of exclusion (traditionally foetal squamous cells found in maternal pulm vasc. @autopsy, but often absent or present w diff sx) - More like anaphylaxis than embolism |
|
|
Amniotic fluid emobolism path |
- Incompletely understood - Postulated foetal antigens enter maternal circ during labour=>complement activation=>DIC - High death rate (mat 80%, foetal 20%) - Progression in 2 phases - I: pulm art vasospasm+ pulm HTN + inc RV pressure=>hypoxia=>myocardial +pulm capillary damage=>left heart failure, +ARDs. - Phase II: hemorrhagic: massive hemorrhage w uterine atony+DIC; fatal consumptive coagulopathy may be the initial presentation |
|
|
Amniotic fluid embolism RFs |
- Multiparity - Hx of allergy (40%) - Male foetus - Advanced maternal age - Maternal chronic medical prob - Trauma - Medical induction of labour - CS/operative delivery - Placenta praevia - Placental abruption - Cervical laceration - Uterine rupture |
|
|
Amniotic fluid embolism complications |
- Pulmonary oedema - LV failure - DIC - Death in 80% mothers, 20% bubs - Risk to subsequent pregnancies unknown |
|
|
Amniotic fluid embolism presentation |
- Sense of impending doom/agitation/altered mentation - Respiratory compromise (dyspnoea + sats <90%) - Hypotension - Seizures - Cardiac arrest - DIC/massive haemorrhage Foetal: - Evidence of compromise (loss of heart rate variability=>decelerations=>terminal bradycardia - Terminal bradycardia |
|
|
Pemphigmoid gestationalis definition, s/s |
- Autoimmune condition - Occurs in mid-late pregnancy - Ab attack basement membrane b/w epidermis and dermis=>bullae or rarely plaques - Intensely itchy - Usually resolves after delivery but can remain up to years - Sometimes flares with OCP, menstruation |
|
|
Pemphigmoid gestationalis tests |
- Skin biopsy y'all, will see abs - Direct immunofluorescence in blood for ABs |
|
|
Pemphigoid gestationalis rx |
- Antihistamines for itch - Topical corticosteroids for mild, oral for med and IV Ig for serious |
|
|
Pemphigoid gestationalis comps |
- Secondary infection and scarring - Premature delivery - Transient infection of the baby that clears after a few months |
|
|
Serum triple test for down's |
- AFP: low - BetaHCG: High - Oestriol: high If AFP high indicates risk of: - Neural tube defects - Anterior abdo wall defects - Patau's (trisomy 13) |
|
|
Causes of high AFP |
Pathological: - Neural tube defects - Anterior abdo wall defects - Patau's syndrome Physiological: - Ethnicity, maternal diabetes/Liver disease - Multiple preg - Oligohydramnios - IUGR |
|
|
Risks of epilepsy in pregnancy (to mother) |
- Higher plasma volume => lower circulating antiepileptics=>more chance of fit=>more risk to babis - Inc tiredness and hyperemesis=>inc. fits |
|
|
Risks of epilepsy in pregnancy to baby |
- 7% risk of congenital defects in baby for one anti-epileptic, risk gets higher with more - Risk of hypoxia during maternal fits (this is why we take the risk of fits and keep mums on antiepileptics) - Similar risk with all anti-epileptics, but choose levitiracetam - Baby has inc risk of being epileptic |
|
|
Optimising epileptic mums for pregnancy |
- Refer to neurology, try to get mum onto a single drug. If no seizures for 2 years, try to go without drugs - Use 5mg folic acid b/c of consuming effect AEDs have - Mum education, advise to keep using med - Detailed anomaly scan at 18-20wks looking for cardiac probs - Start vitamin K from 36wks to minimise chance of clotting prob - Antiepileptics are not contraindicated in breast feeding |
|
|
GDM risks to baby |
- Macrosomia - Hypoglycaemia - Neonatal resp distress syndrome - Inc. stillbirth rate - Polyhydramnios |
|
|
GDM mgmt |
- Optimise BS; nutritionist, GP, O&G - No oral hypoglycaemics! use insulin - Measure BGL pre+post prandial - Regular foetal growth scans for polyhydramnios - Delivery by 40 wks - Sliding scale insulin in labour - Insulin stop immediately post partum as Glucose tolerance restores immediately - Monitor baby for hypoglycaemia - Mother have OGTT in 6wks to rule out ongoing DM |
|
|
Options in down's screening |
- Nuchal translucency 11-13+6wks - Serum test (AFP, BHCG, oestriol) - Amniocentesis at 15wks - Chorionic villus sampling 11-14wks |
|
|
Impact of maternal anaemia in pregnancy on baby |
- Low birth weight - Foetal anaemia - Cognitive impairment |
|
|
VBAC |
- Successful in 70%, emergency caesar in 30% - 1:200 risk of uterine rupture (scar dishisence - Do not augment labour - Fast patient, have close CTG monitoring + IV (plan for failure) |
|
|
Risks of caesarian section |
- Thromboembolic events, haemorrhage and infection - Mobility + ability to care for baby red. d/t major abdo surgery - After 2 caesars one cannot have vag birth - Maximum is usually 4 caesars b/c uterus gets too scarred and could rupture |
|
|
Risks of multiple pregnancy (to mum) |
Higher risk of: - Hyperemesis gravidarum - Pre-eclampsia - Foetal loss - antepartrum haemorrhage - GDM - Anaemia - Thrombosis - Caesaraen - Preterm labour |
|
|
Risks of multiple pregnancy (to babies) |
- IUGR - Prematurity - Still birth - Operative delivery - Congenital abnormalities - Neonatal death |
|
|
External cephalic version |
- Used to turn breech babies - 50% success rate, some revert to breech after version - Usually salbutamol given to relax uterus first - Contraindicated: previous uterine surgery, pre-eclampsia, IUGR, oligohydramnios - Sometimes results in foetal heart abnormalities=>caesaraen |
|
|
RFs for breech |
- Multiparity - Uterine abnormality (eg. fibroids) - Placenta praevia - Multiple preg - Oligohydramnios - Polyhydramnios - Prematurity - Congenital abnorm in foetus - Check the hips of breech babies! |
|
|
Considerations in maternal HIV in preg |
- Elective caesaraen - Get viral load as low as poss - NRTI for baby for first 6wks of life (zidovudine) also should be given to mum IV intrapartum - Avoid breast feeding - Confidentiality |
|
|
Pregnancy induced cholestasis |
- Usually occurs in final trimester - Causes itching from serum bile acid build up - No lasting effects for mother - Assoc. w increased still birth - Elevated liver enzymes - Use antihistamines to control itch - Do a liver USS to exclude other causes of cholestasis + a foetal one for maternal reassurance - Give vitamin K because absorption may be impacted -50% chance of reoccurence in later pregs or with OCP use |
|
|
Hypothyroidism in preg |
- Usually no dangerous effects on mum. Titrate thyroxine to keep TSH <5ug - Assoc w: infertility, still birth, miscarriage, pre-eclampsia, anaemia Anti-TSH antibodies can rarely cross the placenta and cause neonatal hypothyroidism, watch for baby goitre |
|
|
Necessary tests when intrauterine death occurs |
- Basic bloods and coags to test for DIC or sepsis from reatined foetus - Kleinhauer: to assess foeto-maternal haemorrhage - Antiphospholipid syndrome: anticardiolipid antibodies + lupus anticoagulant - BSL - Skin biopsy and swabs of baby for karyotyping + infectious - Post mortem if parents agree |
|
|
DDX intrauterine death |
- Maternal diabetes, infection, thrombophilia - Foetal abnormalities (chromosomal or other), cord incident - Placental: abruption, postmaturity, uteroplacental insufficiency (d/t pre-eclampsia) - Idiopathic |
|
|
Puerperal pyrexia ddx |
B-5W Breast: engorgement, mastitis Wind: atelectasis, pneumonia Water: UTI Wound: episiotomy, C/S site infection Walking: DVT, thrombophlebitis Womb: endometritis |
|
|
Post-partum psychosis rx |
- Atypical antipsychotics are better - Treat for at least one year, sometimes lifetime prophylaxis is needed - Olanzapine, quietiapine, risperadone preferred - Can also use benzotropine at the same time to red. EPSEs - ECT can be used if refractory or non-compliant - All antipsychotics pass into breast milk, but some have negible effect on baby. assess case by case |
|
|
Post-partum psychosis prophylaxis in bipolar women |
- This is a high risk group for post-partum psychosis. They need good education. - Insomnia can be an early sign and can be treated with lorazapam post-partum - Mood stabilisers should be used prophylactically immediately post-partum |
|
|
Treatment threshold for antihypertensive therapy in pre-eclampsia |
- Only prescribe antiHTN if >160/110mmHg OR - Mum is at risk of hypertensive crisis This is because you don't want to risk insufficient placental blood supply |
|
|
Absent diastolic flow of foetus |
- Not an indication for urgent delivery (unless coupled with IUGR) - Indicates LSCS because baby will not survive stresses of vaginal birth |
|
|
HYpertension in pregnancy definiton |
>140/90mmHg (confirmed by 2 readings at least 2hrs apart) - Don't aim to lower <120/80 - Important to lower BP to protect mum from effects of high BP, but does not alter course of pre-eclampsia |
|
|
Post partum mgmt of HTN |
- BP peaks 3-5 days post delivery - Mehtyldopa should not be used after delivery b/c of risk of PPDepression - Use a B blocker, catopril or nifedipine these are safe in Bfeeding - F/y appt with GP at 6wks, if still high, look for important 2o causes |
|
|
Pre-eclampsia definition |
- BP >140/90mmHg + 300mg proteinuria per day OR > BP by 30 systolic or 15 diastolic if woman is already hypertensive pre-preg |
|
|
Pre-eclampsia screening |
- PAPP-A - Raised uric acid, low platelets, raised Hb may indicate pre-eclampsia per proteinuria occurs - Uterine artery dopplers at 11 or 22wks are preictive of severe or early onset pre-eclampsia - Combined screening of hx, PAPP-A and uterine artery doppler at 12wks usually used |
|
|
Pre-eclampsia prophylaxis |
- Low dose aspirin before 16wks in subsequent pregs after having pre-eclampsia reduces risk of repeat preeclampsia by a fifth |
|
|
Pre-eclampsia s/s |
- RUQ pain - Vision disturbance (flashing) - Facial oedema - Headache - HTN - Proteinuria >300mg/day - Confusion - Hyperreflexia + >3 beats clonus (cerebral irritation) - Abruption of placenta (vag bleding + uterine tenderness) - IUGR on USS |
|
|
Pre-eclampsia ix |
- Inc Urea + creatinine - Inc urate - Inc Hb d/t haemoconcentration - Low plt - Ind LDH as a marker of hameolysis - Inc liver enzymes - Prolonged PT and aPTT - >300mg proteinuria/day |
|
|
Complications pre-eclampsia |
- IUGR - Cerebral haemorrhage - HELLP - Renal failure - Placental abruption - Eclampsia - Low birth weight and preterm birth |
|
|
Chronic hypertension diagnosis |
Chronic hypertension refers to hypertension before 20 weeks gestation and persisting beyond twelve weeks postpartum
|
|
|
Indications to manage pre-eclampsia as an outpatient |
- BP <160/110, low proteinuria - Difficulty in distinguishing from preg induced HTN - Sensible px who understands risks, lives close and has constant supervision - Twice weekly BP and urine checks, weekly bloods |
|
|
Very high BP mgmt |
(start mgmt at >160/110) - Labetalol IV with a 250ml fuid bolus to stop precipitous drop in BP which may cause placental insuff - Otherwise nifedipine oral - Methyldopa oral is an option, must be stopped post-natal b/c depression risk |
|
|
Indications for admission in pre-eclampsia + suveillance of moderate (<160/110) pre-eclampsia |
- High proteinuria MGMT: - Admit, 4hrly BP - Daily urinalysis, 24hr urine protein - Daily CTG - Bloods 3x weekly - Foetal growth scan 2wkly +/- Doppler/liquor vol |
|
|
Severe pre-eclampsia mgmt |
• BP needs to be stabilized with antihypertensive medication (must aim for <160 systolic and <110 diastolic).• Initially use PO nifedipine 10mg: can be given twice 30min apart.• If BP remains high after 2–3 nifedipine doses:• start IV labetalol infusion• i infusion rate until BP is adequately controlled.• Start maintenance therapy, usually labetalol; methyldopa if asthmatic.Other management• Take bloods for FBC, urea and electrolytes (U&E), LFTs, and clotting profile.• Strict fluid balance chart: consider a catheter.• CTG monitoring of fetus until condition stable.• Ultrasound of fetus:• evidence of IUGR, estimate weight if severely preterm• assess condition using fetal and umbilical artery Doppler. If <34wks, steroids should be given and the pregnancy may be managed expectantly unless the maternal or fetal condition worsens
|
|
|
Foetal fibronectin test use |
- Test for likely pre-term labour - FFN leaks into vag - Binds decidua to chorion, so when they separate it leaks - Can be used b/w 22 and 34 weeks - It has a high negative predictive value (same as D-Dimer), so a positive result doesn't mean much, but a negative result is a good indicator nothing is going on! |
|
|
CMV in preg epidemiology and transfer rates |
- 50% will transfer to baby - Of those only 10% will be symptomatic - 90% of the symptomatic bubs will have significant long term impairment |
|
|
Congenital CMV impacts on baby |
- Ascites/enlarged liver - IUGR - Poly or oligohydramnios - Hydrops - Ventriculomegaly - Cerebral or intrabdominal microcalcifications - Hearing impairment in 25% - Visual impairment - Learning probs - Mental retardation - Neonatal death |
|
|
Previous CMV risk on future pregs |
- High risk for a number of years post seroconversion with same risks as first preg - Can test bab's status by amniocentesis at 20wks |
|
|
Chorioamnitis s/s |
- Maternal fever, malaise - Uterine tenderness - Offensive green/brown discharge - Foetal and maternal tachycardia - Don't do VE because it can introduce infection, do spec - Important because it can cause PPROM and early labour |
|
|
Chorioamnitis ix |
- High and low vag swabs - CBE/CRP - MSU - USS for foetal wellbeing, position, liquor vol |
|
|
Chorioamnitis mgmt |
- Betamethasone IM 2 doses - Deliver whatever the gestation - Broad spec abx (triples) |
|
|
Umbilical artery doppler |
Increased resistance in the fetal umbilical arterial circulation detected by Doppler suggests high resistance within the placenta. This is indicative of placental insufficiency, the leading cause of IUGR. Umbilical artery Doppler is likely to be normal in a fetus which is small for dates, but otherwise healthy.If there is absent end-diastolic flow this suggests more than 60% of the villous vasculature is damaged. Any reversal of end-diastolic flow will indicate severe impairment of the villous vasculature and high risk of fetal death
|
|
|
Indications for continuous CTG |
- Epidural - Syntocinon infusion - Meconium stained liquor - Obstetric complications predisposing foetus to hypoxia |
|
|
Obstructed labour signs |
- Often assoc w maternal tachycardia - Cervix fails to dilate + oedema - Head above ischial spines - Excessive caput and moulding - Relative cephalopelvic disproportion (foetal malpresentation) |
|
|
Foetal Warfarin syndrome s/s |
- IUGR - CNS, cardiacmalformations, skeletal, soft tissue - Deafness - Marked intellectual disability - Feeding difficulties |
|
|
- Foetal warfarin syndrome indicidence |
1/3 of babies to mothers who have warfarin in 1st trimester |
|
|
Ovarian Hyperstimulation syndrome, definition, patho |
- Rare emergency occuring in IVF - Too much FSH/LH(from exogenous source) + postive feedback from BHCG from successful pregnancy - Hyperstimulation of ovaries=>ovarian VEGF=> inc vascular permeability => massive ovarian cysts + ascites=>fluid shift to third space |
|
|
Ovarian Hyperstimulation syndrome s/s |
- Severe abdo pain - Intractable n/v - Ascites - Sometimes pleural effusion - Hypovolaemia and oliguria - Hyperkalaemia and hyponatraemia - Derangement of LFTs |
|
|
Ovarian hyperstimulation syndrome mgmt |
- Fluid and electrolyte replacement - Analgesia (opiate) - VTE prophylaxis - high dependency care - Do not operate |
|
|
Human placental lactogen definition |
- Hormone produced in preg, similar to growth hormone and prolactin - Produced by syncitiotrophoblast |
|
|
Human placental lactogen physiology |
- Dec. insulin sensitivity of mum=>greater level of glucose to bub - Dec. glucose utilisation by mum=>more for bub - Inc. lipolysis in mum => more glucose for bub + ketones produced from FFAs can be used by bub - Higher levels in multipe gestation - Potent prolactin receptor agonist, weak growth hormone receptor agonist - Can ensure foetal nutrition in the context of maternal malnutrition |
|
|
Acute fatty liver of pregnancy patho |
- High morbidity and mortality for both mother and infant - Only occurs in pregnancy (normal fatty acid metabolism otherwise) - Autosomal recessive gene coding for LCHAD. Effected mums are heterozygous, babies who are homozygous can't metabolise fatty acids=>pass these to mum, who has deficient ezyme action (b/c heterozygous)=> build up=>hepatic strain |
|
|
Acute fatty liver of pregnancy presentation |
- Nausea and vom (common, sometimes not until 3rd trimester) - LUQ pain (common) - Malaise - Upper GI bleeding - Pancreatitis - Infection - Hypoglycaemia - Acute renal failure - Fulminant liver failure + hepatic encephalopathy - HTN - Jaundice (this should raise alarm bells! can happen in pre-eclampsia, but more comm this) - Bleeding - Confusion |
|
|
Acute fatty liver of preg surgery and anaesthetic considerations |
- Do not use anaesthetics that are hepatotoxic, regional anaesthesia better - After vag delivery, inspect carefully for vag lacs, b/c mother may be more bleedy that usual - Good haemostasis if caesarean is done for same reason |
|
|
Acute fatty liver of pregnancy mgmt |
- Delivery of baby is the only cure, needs to be done w/i 24hrs of diagnosis. If can't deliver witin 24hrs vaginally do caesarean - Replace coagulation factors - Give 5% dextrose, mum could die w/o b/c of hypoglycaemia. Monitor BSL carefully until liver fcn returns and mum can tolerate diet - Fluid balance: haemorrhage can cause acute tubular necrosis, but APO can develop d/t low oncotic pressures - Post-partum plasma exchange/phoresis is an emerging technique for severe AFLP |