Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
176 Cards in this Set
- Front
- Back
|
5 kidney functions
|
1. Waste removal via urine
2. LTR of arterial pressure 3. Reg of acid-base balance 4. LTR of RBC production 5. Reg of minerals |
|
|
1. Kidneys remove _______ products in urine.
|
waste
|
|
|
2. Kidneys perform long term regulation of _______ pressure.
|
arterial
|
|
|
3. Kidneys regulate the ___________ balance.
|
acid-base
|
|
|
4. Kidneys perform long term regulation of _______ production.
|
Red Blood Cell
|
|
|
5. Kidneys regulate __________.
|
minerals
|
|
|
Name all the parts of kidney anatomy you can think of (at least 10):
|
kidney, ureter, bladder, urethra, renal A/V/N, ureter, Minor calyx, Major calyx, Nephron, Papilla, renal cortex, renal medulla, renal pelvis, renal pyramid, capsule
|
|
|
what kind of bilirubin in urine? in feces?
|
conjugated in urine, unconjugated in feces
|
|
|
What can be used as a unit to compare one person's urine to another person's urine?
|
creatine levels
|
|
|
all things not absorbed (filtered) by kidneys are called
|
metabolic waste products and foreign chemicals
|
|
|
name at least 5 things excreted by kidneys
|
urea, uric acid, creatinine, bilirubin, pesticides, food additives, toxins, drugs
|
|
|
made in liver only
*from PROTEIN metabolism |
urea
|
|
|
gout
*from Nucleic Acid metabolism |
uric acid
|
|
|
from muscle metabolism
|
creatinine
|
|
|
from HEMOglobin metabolism (RBC)
|
bilirubin
|
|
|
Basic mechanisms of Urine formation
|
1. FILTRATION
2. RE-ABSORPTION 3. SECRETION 4. EXCRETION |
|
|
Where does FILTRATION take place?
|
Bowman's capsule (filtrate from afferent)
|
|
|
Where does REABSORBED material go?
|
into peritubular capillaries
|
|
|
What kind of things get SECRETED?
|
H+ ions, drugs, toxins
|
|
|
Final stage of basic mechanisms of urine formation?
|
EXCRETION
|
|
|
2 arterioles attached to Glomerulus
|
Afferent (in) arteriole
& Efferent (out) arteriole |
|
|
Glomerular capillaries go to the
|
Bowman's space and capsule
|
|
|
Efferent arteriole goes to the
|
efferent arteriole filter
|
|
|
Bowman's capsule surrounding glomerulus goes to
|
Nephron : where filtration, reabsorption, secretion and excretion all happen
|
|
|
efferent arteriole filter goes to
|
Peritubular capillaries
then to Vasa Recta, then to the Renal vein |
|
|
the back-up plan as well as the gate for reabsorption mechanism of urine formation
|
peritubular capillaries
|
|
|
All the glomeruli are in the
|
Cortex!
**because that's where the afferent and efferent arterioles are |
|
|
Vein portion right after Peritubular capillaries
|
VASA RECTA
|
|
|
Every afferent arteriole is in the
|
Cortex!
|
|
|
Some nephrons drop Loops of Henle into the ___________, so the longer the nephron, the more is ________.
|
medulla
absorbed |
|
|
Functional unit of the kidney
|
Nephron
|
|
|
camels and desert rats have crazy long ___________
|
nephrons (so more will be reabsorbed)
|
|
|
blood supply of nephron
|
interlobar artery and veins
*going to corticolobar and juxtamedullary nephrons |
|
|
brings blood to the glomerulus
|
AFFERENT arteriole -
large size, unfiltered blood |
|
|
blood leaving glomerulus travels through the
|
Efferent arteriole -
provides back pressure |
|
|
How do you tell the difference between the afferent and efferent arterioles physically?
|
Afferent is very large, muscular due to high volume of unfiltered blood
efferent is opposite |
|
|
What percentage of water is reabsorbed of the 100L that goes through the Bowman's space?
|
99%
|
|
|
Step 1: Glomerular filtration takes place where?
|
Glomerulus and Bowman's Capsule
|
|
|
Step 1: Glomerular filtration is based on __________ of molecule.
|
size of molecule (not type)
|
|
|
surrounds glomerulus
|
Bowman's CAPSULE
|
|
|
space around glomerulus
|
Bowman's space (it's in the description)
|
|
|
Percentage of renal plasma flow averaged by glomerular filtration
|
20% of all of your blood is in your kidney right now
|
|
|
the glomerulus is made of capillaries with specialized epithelium - describe?
|
Fenestrations (pores)
Podocytes (reinforcement) Basement membrane (leak prevent) |
|
|
What holds podocytes (reinforcement around glomerulus epithelium) together?
|
glucosamine
(makes sticky ie hyaluronic acid in urine) |
|
|
Podocytes have nuclei & finger-like projections that cover the fenestrated epithelium of the glomerulus. What are these openings called?
|
Slit pores
|
|
|
another term for the epithelial cells of the glomerulus
|
podocytes
|
|
|
restriction site for proteins on glomerulus
|
basement membrane
|
|
|
The pressure gradient of glomerulus uses _______- flow equation.
|
capillary flow equation
|
|
|
How can I increase hydrostatic pressure in glomerulus?
|
make Afferent WIDE or Efferent TINY
|
|
|
How can I decrease hydrostatic pressure in the glomerulus?
|
to decrease hydrostatic pressure, make Afferent narrow and Efferent large
|
|
|
Net Filtration pressure of +10 is got by subtracting what 3 things?
|
glomerular Hydrostatic p.
Bowman's capsule p. glomerular oncotic/Colloidal osmotic p. |
|
|
GFR
|
Glomerular Filtration Rate :
125 ml/min = 180 liters/day |
|
|
Plama volume is filtered ___x a day.
|
60
|
|
|
Glom filtrate and plasma filtrate are about same composition, except what?
|
large proteins should never be in filtrate
|
|
|
You have 90 mg/decaliter glucose in plasma. How much is in your filtrate?
|
90 (same - because it has the same composition of every thing that is small)
|
|
|
Why does Bowman's capsule have NO interstitial colloidal osmotic/oncotic pressure?
|
because it has NO proteins to attract water - better not be!!!
|
|
|
Blood plasma (125 mg/decL NaCl) =
|
Filtrate (125 mg/decL NaCl)
|
|
|
Step 1 was Glomerular FILTRATION.
What is step 2? |
Tubular RE-ABSORPTION
|
|
|
Location of step 2/tubular RE-ABSORPTION
|
Proximal Convoluted Tubule of nephron
|
|
|
How much does the PCT of nephron reabsorb?
|
65% of water
- 100% of glucose and aminos Electrolytes Na+, K+, and Cl- |
|
|
Where is 65% of the 99% of REabsorption taking place?
|
Proximal Convoluted Tubule!
|
|
|
In the PCT, there are 2 paths of REabsorption via the microvilli:
|
1. Paracellular path (between/next to)
2. Transcellular path (through) |
|
|
How does water go through PCT lumen to Peritubular capillary?
|
OSMOSIS - can go paracellularly or transcellularly
|
|
|
How do solutes go through PCT lumen to peritubular capillary?
|
Active (ATP)
or Passive (diffusion) - can go paracellularly or transcellularly |
|
|
How do very small solutes go from the PCT lumen through tubular cells to the peritubular capillary/blood?
|
PASSIVE DIFFUSION for small molecules and ions in PCT
|
|
|
can only be reabsorbed in the PCT
|
K+
|
|
|
can go in on lumenal surface of PCT passively, but can only be pumped out by Na/K-ATPase pump actively to peritubular capillary/blood?
|
Na+
(goes in passive diffusion, needs pumping out active) |
|
|
Na+ comes into the PCT lumenal surface via passive diffusion. Why?
|
Because filtrate that it is in has a Total Osmotic Pressure = to the Capillary Osmotic Pressure.
|
|
|
Na+ comes into PCT from filtrate via passive diffusion due to equal osmotic pressures inside and outside of the capillary? Why, then, does it require the Na/K-ATPase pump to get it out?
|
Because that would be against the concentration gradient since the pressures are the same and passive diffusion was pulling it in just fine. It wants to stay but needs to be asked to leave.
|
|
|
bulk flow
|
water + solutes
some K+ is going both ways |
|
|
results in the reabsorption of sodium and urinary excretion of potassium
|
active transport of sodium via the Na/K-ATPase pump to move Na+ against conc. gradient back into the Peritubular capillary/blood/body
|
|
|
How is Na+ RE-absorbed back into the body so it isn't excreted with filtrate?
|
Na/H+ ANTIPORTER protein in lumenal surface of PCT excretes H+ and absorbs/collects Na+
|
|
|
Glucose has a TRANSPORT MAXIMUM, whether it's facilitated diffusion or secondary active transport. What is this Transport Maximum?
|
max rate of tubular transport due to SATURATION of carriers, limited ATP, etc.
|
|
|
How do both glucose & amino acids travel through the tubular epithelial cells of the PCT (interstitial fluid)?
|
CO-TRANSPORT: attached to Na+
1. Na+ assisted Facilitated Diffusion 2. Na/K-ATPase pump as Secondary Active Transport |
|
|
NORMAL glucose transport maximum
|
80-120 mg/min (on T.M.curve)
|
|
|
Excretion (the amt of glucose in urine) is found by ?
|
EX glucose = Filtered load - Transport Maximum
|
|
|
the tubular load at which transport maximum is EXCEEDED in some nephrons
|
Threshold
|
|
|
Is threshold the same as the transport maximum in all parts of the kidney?
|
no, some nephrons have lower transport max's than others
|
|
|
GFR: 150 ml/min
FL: 300 mg/ml What is EX rate of glucose? |
EX glucose= Filtered Load - Trans Max
300mg/100ml x 150ml/min = 450 ml/min so... 450 mg/min - 300 mg/min = 150 mg/min so abnormal (80-120) |
|
|
What goes into the PCT (5)
|
water
Na+ Cl- bicarbonate K+ |
|
|
What goes out of the PCT (You 3 out!)
|
H+
organic acids organic bases |
|
|
Why is pH lower in PCT?
|
Na/H+ antiporter in PCT
|
|
|
Plasma Colloidal Osmotic pressure is always
|
32
|
|
|
Why is hydrostatic pressure of PCT lower?
|
because of so much water left in glomerulus
|
|
|
When figuring the Peritubular Capillary REABSORPTION, add things going ___, and subtract things going ____.
|
add in (+) to interstitial fluid
subtract out (-) to peritubular cap |
|
|
function of Loop of Henle
|
Concentration of Urine
|
|
|
How does Loop of Henle concentrate urine (mechanism)?
|
Counter-current concentration
|
|
|
Loop of Henle DESCENDING water permeable?
|
yes
water reabsorbed into the interstitium |
|
|
Is the Ascending Loop of Henle permeable to water?
|
no
NaCl is reabsorbed here, increasing osmolarity of interstitium to suck water from descending loop (counter current or trade agreement!) |
|
|
Water permeability in what parts of nephron?
|
Descending loop
(skip ass) Collecting duct ...this is counter current concentration |
|
|
Describe counter current concentration short version?
|
Loop of Henle:
Descending - Water Ascending - Salt collecting duct - Water |
|
|
Total osmotic pressure in glomerulus
|
300
|
|
|
By the end of PCT, 65% of the total 99% has be reabsorbed, but osmotic pressure has?
|
remained the SAME on both sides so the cells don't shrink or swell
|
|
|
Osmolarity of Filtrate =
|
Osmolartity of Plasma
|
|
|
How do we concentrate the urine?
|
Counter current CONCENTRATION in the Loop of Henle
(Descending - Water, Ascending - Salt) collecting duct - Water |
|
|
lowest osmolarity of Loop of Henle
|
Distal Convoluted Tubule
(because of NaCl being reabsorbed instead of water) |
|
|
Where is osmolarity MOST (1200) concentrated in the Loop of Henle?
|
at bottom where descending meets ascending (1200)
|
|
|
What begins the final squeeze of water (last bit of 99%) in the collecting ducts?
|
urea passive diffuse into medulla so water will follow it
|
|
|
At top of collecting duct, what promotes water reabsorption?
|
ADH-dependent with aquaporins
|
|
|
adrenal medulla vs. renal medulla
|
adrenal: post ganglionic sympathetic 2nd order neuron
renal: loop of Henle & collecting duct + most interstitial osmotic pressure + most concentrated urine |
|
|
which is more permeable to water:
the thin loop of Henle or the thick loop of Henle? |
thin!
very permeable to water |
|
|
thick loop of Henle
|
- Not water permeable
- kicks out H+ - absorbs Na, Cl, K, Ca, HCO3, Mg (think thin, think water) |
|
|
Tubular SECRETION site:
|
DCT
|
|
|
Substances that get quickly dumped (secreted) in the DCT?
|
H+
foreign substances (including drugs) |
|
|
The Distal Convoluted Tubule is the site of the 99% of solutes are reabsorbed - how is permeability to water determined at this point?
|
HORMONES!
Aldosterone (reabsorbs Na + Water and secretes K) Anti-diuretic hormone reabsorbs water |
|
|
Tell me about Big Al Dosterone
|
Lives in Zona Glomerulosa of adrenal cortex. Reabsorbs Na + Water, kicks out Potassium bums.
|
|
|
Early DCT is not permeable to
|
water or urea
|
|
|
Late DCT is not permeable to ______ but permeability to water depends on __________.
|
not to urea but permeability of water depends on ADH
|
|
|
kind of cells that use big Al Dosterone
|
Principal cells (columnar epithelium) in LATE DCT to drive Na/K pump to pull water out into blood
|
|
|
The LATE DCT is completely dependent on ADH so it inserts ___________ and water will follow sodium out to the tissues.
|
aquaporin
|
|
|
What special cells are in the
LATE DCT? |
a. Principal cells (Al Dosterone, aquaporins, ADH)
b. Intercalated cells (K + HCO3) |
|
|
big Al Dosterone actions in late DCT
|
Up Na+ reabsorb - principal cells
Up K+ (bums)secretion - principal cells Up H+ secretion - Intercalated cells |
|
|
3 actions of Aldosterone
|
1. Increase Na reabsorption (principals)
2. Increase K secretion (principals) 3. Increase H & Bicarbonate secretion (intercalated) |
|
|
How does ADH (antidiuretic hormone) get in the blood to start with?
|
responding to Na+ conc. in blood via the SUPRAOPTIC NUCLEI of the hypothalamus detects - talks to posterior pituitary that actually secretes the ADH
|
|
|
Where is Big Al?
|
distal tubule
|
|
|
Where is ADH?
|
collecting tubule
|
|
|
increases water permeability and reabsorption in the distal (Big Al) and collecting tubules (_____).
|
ADH
|
|
|
allows differential control, solute excretion via AQUAPORINS insertion into cell membrane of principal cells
|
ADH secreted by posterior pituitary -
*important controller of extracell. fluid osmolarity |
|
|
Why does big Aldosterone show up?
|
there is not enough Na to attract water for re-absorption, so he pulls Na to attract water
|
|
|
Anti-diuresis
|
increases blood volume so increases blood pressure (ADH to increase water perm and re-sorb)
|
|
|
Water ONLY comes out in late DCT and Collecting tubule if?
|
ADH
|
|
|
No ADH, no
|
no permeable/no water reabsorbed
|
|
|
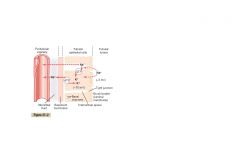
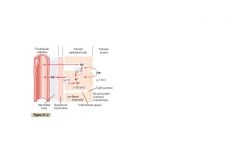
what's the only thing that goes back into the medullary collecting tubule? (fig 27-13 Guyton)
|
H+
|
|
|
If water is reabsorbed to a greater extent than the solute, the solute will become?
|
more concentrated in the tubule
*creatinine, inulin are NOT absorbed |
|
|
If solutes are reabsorbed more than water, then the solutes become?
|
less concentrated in the tubule
***amino acids & glucose ARE absorbed |
|
|
The appearance of glucose in the urine (above 125 mg/min) at threshold occurs before _____________ is reached.
|
Transport Maximum
|
|
Kind of transport of Na+ through tubular epithelium
|
ACTIVE
|
|
|
Long term blood pressure control by the kidney:
|
via renin-angiotensin system
|
|
|
Kidney uses ? to control renal blood flow?
|
Renin-Angiotensin system
|
|
|
How does the GFR and renal blood flow remain constant?
|
Blood pressures within physiological range:
Feedback mechanisms of Juxtaglomerular Complex & Renal-Arteriole Resistance |
|
|
Location of Macula Densa
|
DCT between afferent and efferent tubules
|
|
|
Structure of Juxtaglomerular apparatus
|
Macula Densa
& Juxtaglomerular cells |
|
|
Sensa-tive to NaCl
|
Macul-a Dens-a
|
|
|
The Mac-u-la Dens-A is very sens-A to
|
NaCl
|
|
|
controls long term blood pressure regulation
|
JUXTAglomerular Apparatus
|
|
|
sensitive to Renin
|
Juxtaglomerular cells
|
|
|
sensitive to NaCl concentration, Beta-receptor stimulation (epinephrine) and Drop in BP due to mechanical stretch
|
Macula Densa
|
|
|
JG cells are in the walls of the
|
afferent and efferent arterioles
|
|
|
JG complex stores and releases
|
RENIN (an enzyme)
|
|
|
cells in the distal tubule ADJACENT to the afferent and efferent arterioles
|
Macula Densa
sensa to NaCl, B-receptor stim and Drop in BP |
|
|
Renin-Angiotensin-____________ Pathway
(RAAP) |
Aldosterone
|
|
|
Step 1 RAAP:
Release of ________ due to _____ concentration |
Renin
NaCl (low in macula densa) |
|
|
RAAP step 1 is release of Renin due to LOW ______ in macula densa
|
NaCl
Renin dilates the afferent arterioles |
|
|
Salt is low in Macula Densa, so _______ arterioles dilate to increase blood flow to the glomerulus. This increases G. hydrostatic pressure and increases GFR!
|
afferent
(NaCl down-afferent dilate-up hydrostatic p. in glomerulus-raises GFR!) Then...Renin is released |
|
|
Renin is released in response to
|
low salt levels in macula densa. Afferent arteriole dilates, pressures rise in glomerulus and RENIN gets released
|
|
|
Low salt - dilate afferent arteriole - RENIN released in order to?
|
Angiotensin I is made and shot out of the liver when the liver detects renin
|
|
|
Angiotensin I from liver keeps afferent arterioles __________.
|
dilated
|
|
|
Angiotensin I from liver sparks ______ from lung. This causes what to constrict the efferent arterioles?
|
Angiotensin II
|
|
|
Angiotensin I =
|
constriction of afferent arterioles (Renin)
|
|
|
Angiotensin II =
|
constriction of EFFERENT arterioles (ACE)
|
|
|
2 functions of Angiotensin II (ACE)
|
1. constricts efferent
2. release Al Dosterone **RESULT: increase GFR via pressure |
|
|
which keeps afferent arteriole open
|
JG complex
|
|
|
which constricts efferent arteriole and causes GFR to rise?
|
Angiotensin II
|
|
|
Angiotensin II is constricting efferent while Angie I opens Afferent - where does Al Dosterone come in?
|
Angiotensin II signals Big Al to come from his neiqhborhood (zona glomerulosa) in adrenal cortex. He grabs Na and gets water to follow, meanwhile kicking out K bums in DCT
|
|
|
If there is high Na, high BP, what happens to the RAAP?
|
Off.
*don't need Big Al to come raise salt even higher so RAAP off. |
|
|
Increase blood volume, increase blood pressure, increase ______
|
GFR
|
|
|
If Beta-receptors are stimulated in the afferent arteriole, the Macula Densa causes?
|
DILATION of afferent arteriole, increasing blood flow to glomerulus and increasing GFR
|
|
|
In response to HYPOtension
|
the macula densa causes dilation of afferent arteriole, increasing blood flow to glomerulus and increasing GFR
|
|
|
2 situations when Macula Densa DILATES afferent arteriole and results:
|
1. B-receptors stimulated
2. Hypotension (low bp) Dilation of afferent a. increases blood flow to glomerulus, then increase GFR |
|
|
How do the kidneys regulate the Acid-Base balance?
|
Excrete acids (kidneys are it!)
Regulate BODY BUFFERS (bicarb) |
|
|
determines peritubular capillary fluid reabsorption
|
balance of hydrostatic and colloid osmotic forces in the peritubular capillaries
|
|
|
__________ efferent arteriole resistance reduces peritubular capillary hydrostatic pressure.
|
Increased, therefore increases fluid reabsorption
|
|
|
Mg+ reabsorption area of nephron
|
ASCENDING loop of Henle
|
|
|
water reabsorption area of nephron
|
PROXIMAL Convoluted Tubule
|
|
|
lungs combine _____+_____ to release bicarbonate buffer
|
CO2 + H20
|
|
|
kidneys combine ________+__________ to release bicarbonate
|
H+ and HCO3
|
|
|
How many bicarbonate ions are absorbed for each H+ released from the kidneys?
|
1:1 ratio of H to H2CO3
|
|
|
What is passively excreted along with the H+ in exchange for bicarbonate?
|
Cl- ion
|
|
|
Where does the bicarbonate to H+/Cl- and HCO3 exchange take place in the kidneys?
|
DCT & collecting duct
|
|
|
buffer system stimulated by an increase in extracellular H+,
GLUTAMINE metabolized |
Ammonia Buffer System (GLUTAMINE)
yields 2 ammonia, 1 bicarbonate |
|
|
buffer system that allows excess H+ to be excreted when bicarbonate buffer system is EXHAUSTED
|
Phosphate buffer system
regenerates bicarbonate ion when bicarbonate buffer sys is EXHAUSTED |
|
|
How is RBC production regulated by the kidneys?
|
hormones!
|
|
|
________delivered to the kidney, ups Erythropoetin production, ups erythropoetin production in bone marrow
|
O2
|
|
|
the delivery of O2 to the kidneys has what effect?
|
Ups erthyropoetin then production f erythropoetin in bone marrow
|
|
|
How are minerals regulated in the kidney?
|
vitamin D
|
|
|
What does the kidney produce to regulate calcium and phosphate metabolism?
|
vitamin D
(1,25-dihydroxy vitamin D3) |