![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
270 Cards in this Set
- Front
- Back
|
What are the parts of neuronal structure? |
Dendrite, soma or cell body, axon, myelin sheath |
|
|
What are the possible directions of conduction for neuron? |
Afferent=sensory Efferent=motor |
|
|
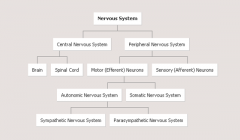
How does the nervous system breakdown? |
|
|
|
Covering of the brain |
bony skull, dura mater, archnoid membrane, pia mater |
|
|
Cushionings of the brain |
Subdural space; subarchnoid space |
|
|
What cushioning of the brain contains the CSF? |
Subarachnoid space |
|
|
Parencimal unit of the nervous system |
neuron |
|
|
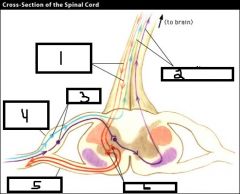
What are the major nerve pathways of the spinal cord? |
Descending (motor) pathway from the motor cortex down Ascending (sensory) pathway: sensory cortex down spinal cord |
|
|
Descending (motor) pathway Ascending (sensory) pathway Sensory neurons Dorsal root ganglion (sensory) Ventral Root Motor neurons |
|
|
What are the peripheral nerves and how many are there? |
8 Cervical, 12 Thoracic, 5 Lumbar, 1 Coccygeal |
|
|
Neurons within peripheral nervous system |
Sensory Neurons and Motor Neurons |
|
|
Motor neurons are involved in what nervous sustems |
Autonomic Nervous System (ANS): SNS and PNS Somatic Nervous system (voluntary) |
|
|
Major (and only) source of fuel for nervous system |
Glucose (brain cannot use anaerobic metabolism) |
|
|
What does peripheral mean in terms of the nervous system? |
Anything that isn't the head or neck |
|
|
What are the types of afferent/sensory tracts? |
Anterolateral and posterior |
|
|
What is the anterolateral afferent (sensory) tract responsible for? What are the characteristics of this tract? Where are the cells of this tract located? |
Pain, temperature, crud or light touch, itch, tickle, sexual sensation Small caliber axons; unmyelinated or lightly myelinated-->slow conduction Cell bodies in contralateral dorsal horn |
|
|
What is the posterior afferent (sensory) tract? What are the characteristics of this tract? Where are the cells of this tract located? |
Position sense (can they feel toe being touched), discriminative touch (what part is being touched), vibration sense, stereognosis (being able to recognize based on touch), graphesthesia (can identify number written on back) Larger caliber axons; heavily myelinated for fast conduction Cell bodies in ipsilateral dorsal horn |
|
|
What type of myelin sheath is involved with pain transmission? |
Thin (slower conduction) |
|
|
Action differences between Autonomic and Somatic Nervous System? |
Autonomic system actions occur without you having to tell it to work; somatic nervous system actions are voluntary |
|
|
Are artery or venous bleeding in the brain more dangerous? Why? |
Venous-->because arterial bleeding shows fast and apparent signs; can be discharged with slow venous bleed |
|
|
Where are the cell bodies for the efferent (motor) tracts located? Fibers? What do the synapses have? |
Cell bodies in contralateral motor cortex; fibers cross in pyramidal decussation (medulla), and synapses with ipsilateral interneurons |
|
|
What produces the cerebrospinal fluid? |
Choroid plexus |
|
|
Efferent (motor) tracts influence the activity of... |
lower motor neurons (LMNs); voluntary control of muscle |
|
|
If neurons do not cross spinal cord (same side), they are called... If neurons do cross spinal cord (opposite side) they are called... |
Ipsilateral Contralateral |
|
|
Cell bodies that are contralateral in dorsal horn are part of what tract? What are their characteristics? |
Anterolateral afferent/sensory tract Slow conduction; un- or lightly myelinated |
|
|
Cell bodies that are ipsilateral in dorsal horn are part of what tract? What are their characteristics? |
Posterior afferent/sensory tract Fast conduction; heavily myelinated |
|
|
What is stereognosis? What is graphesthesia? |
Being able to recognize object solely based on touch; being able to recognize the number being drawn on back |
|
|
What happens if there is stroke located before the medulla? After? |
Same side effected Opposite side effected (because nerves have crossed in medulla) |
|
|
Right brain functions |
Insight, 3-D forms, Art awareness, imagination, music awareness, left-hand control |
|
|
Left brain functions |
Number skills, written language, reasoning, spoken language, scientific skills, right-hand control |
|
|
What cranial nerve is involved with the PNS? |
Vagus nerve (CN 10) |
|
|
Mechanisms of injury to NS |
nHypoxic& ischemic injurynInjuryfrom excitatory amino acidsnIncreasedvolume and pressurenBrainherniationnCerebraledemanHydrocephalus |
|
|
Relationship between ischemia and hypoxia |
Can be hypoxic and not ischemic CANNOT be ischemic and not hypoxic |
|
|
Brain is what % of body weight? Received what % of cardiac output? Consumes what % of oxygen? |
2%; >15%, 20% |
|
|
Impact of hypoxia (but normal blood flow) on the brain |
Deprivation of oxygen with maintained blood-->depressant effect on the brain-->euphoria, listlessness, drowsiness, impaired problem solving (differs person to person) |
|
|
Focal v. global ischemia with examples |
Focal: where blood flow is inadequate to meet the metabolic demands of a part of the brain (ex. stroke) Global=when blood flow is inadequate to meet the metabolic demands of the entire brain (ex. cardiac arrest or circulatory shock) |
|
|
What happens during the course of global ischemia? |
Oxygen consumed in 10 second, glucose sources exhausted in 2-4 minutes, cellular ATP stores depleted in 4-5 minutes Excessive influx of sodium and calcium, efflux of potassium |
|
|
During global ischemia what does the influx of sodium and calcium cause? |
Influx of sodium-->neuronal and interstitial edema Influx of calcium--> Calcium Cascade--> release of intracellular and nuclear enzymes that cause cell destruction |
|
|
Global ischemic injury types |
Laminar necrosis; watershed zones |
|
|
What are watershed zones? |
Types of global ischemic injury types Concentrated damage in anatomically vulnerable border zones between overlapping territories supplied by the major cerebral arteries (middle, anterior, posterior) |
|
|
What is laminar necrosis? |
Global ischemic injury type; occurs in areas supplied by penetrating arteries--gray matter of the cerebral cortex Necrosis that develops is laminar (along a parallel plan or layer) and is most severe in the deeper layers of the cortex |
|
|
Gray matter of the brain contains... Where is gray matter in the brain located? In the spinal cord? What is white matter? Where is it located in brain? |
Cell bodies; outside of brain; inside of spinal cord Axon with myelin sheath; inside brain |
|
|
What is post-ischemic hypoperfusion? |
nDamageto blood vessels and changesin blood flowas a result of ischemia that prevents the return of adequate tissue perfusiondespite reestablishment of circulation |
|
|
What are the mechanisms involved with post-ischemic hypoperfusion? |
Desaturation of venous blood (means arteries are already empty of oxygen); capillary and venous blood; sludging of blood increases blood viscosity and increases resistance to blood flow; immediate vasomotor paralysis d/t extracellular acidosis-->ischemic vasoconstriction; hypermetabolism d/t circulating catecholamines-->increases cerebral metabolic rate and increased need for energy producing substrates |
|
|
Treatment for global ischemia is aimed at: What are the methods of treatment? |
Providing oxygen and decreasing metabolic needs during non-flow state Decrease brain temperature; normovoemic hemodilution to overcome sludging during reperfusion; control of blood glucose 100-200mg/dL |
|
|
What is excitotoxicity? |
Brain injury due to excitatory amino acids Overstimulation of receptors for specific amino acids that act as excitatory neurotransmitters (glutamate and aspartate) |
|
|
What is glutamate? It's activity is coupled with... |
Principal excitatory neurotransmitter in brain; activity is coupled with receptor-operated calcium ion channels-->calcium cascade |
|
|
What happens with glutamate when there is injury to the brain? |
Injury-->accumulation of extracellular glutamine-->glutamate toxicity--> within minutes there is neuronal swelling (d/t sodium influx) and later within hours have the effects of calcium cascade (d/t calcium influx) Accounts for long-term effects of brain injury |
|
|
Normal intracranial pressure (ICP) range? What is the makeup? |
5-15 mm Hg Blood volume 10%, brain tissue 80%, CSF 10% |
|
|
What is the Monroe-Kelli Hypothesis? |
Reciprocal compensation: CSF and BV are most able to compensate for changes in ICP (since brain tissue is not going to move) |
|
|
How can the amount of cerebrospinal fluid be increased? Decreased? |
Increased amount with excess production, decreased absorption, or obstructed circulation Decreased amount with translocation to the spinal subarachnoid space or increased resorption |
|
|
How can the amount of blood volume be increased? Decreased |
Increased: vasodilation of cerebral blood vessels or obstruction of venous outflow Decrease: low pressure venous system has limited volume buffering capacity and blood flow controlled by autoregulatory mechanisms (hyperventilation to decreased PCO2 leads to vasoconstriction) |
|
|
Results of excessive intracranial pressure |
Obstructs cerebral blood flow; destroys brain cells (kills brain tissue), displaces brain tissue (herniation) |
|
|
What is cerebral compliance? |
=Change in volume/change in pressure (formula) Brain's ability to adjust to increased volume and pressure |
|
|
You have increased cerebral volume with: |
brain tumor, cerebral edema, bleeding into brain tissue (hematoma) |
|
|
What is the pressure-volume curve? |
nonce compensatory mechanisms have beenexceeded, even small changes in volume result in dramatic increases in pressure |
|
|
Normal cerebral perfusion pressure? How is it calculated? What reading would indicate brain ischemia? What happens if ICP is greater than or equal to MABP |
70-100 mm Hg; CPP=MABP-ICP <50-70 mm Hg Inadequate tissue perfusion, cellular hypoxia, neuronal death |
|
|
What are the stages of intracranial hypertension? |
Stage 1=Compensation Stage 2= Increased ICP Stage 3=Decompensation Stage 4=Herniation or Loss of CPP |
|
|
What happens during stage 1 of intracranial hypertension? |
COMPENSATION Increased volume in one compartment leads to decrease in one or both of other volumes; intracranial pressure remains near normal |
|
|
What happens during stage 2 of intracranial hypertension? |
INCREASED ICP Brain responds by constricting cerebral arteries to reduce pressure but results in hypoxia and hypercarbia and deterioration of brain function |
|
|
What happens during stage 3 of intracranial hypertension? |
DECOMPENSATION Cerebral arteries respond with reflex dilation-->leads to increased blood volume---> which further increases ICP Small changes in intracranial volume result in large changes in pressure |
|
|
What happens during stage 4 of intracranial hypertension? |
HERNIATION OR LOSS OF CPP Swelling and pressure leads to herniation When ICP=MABP-->no cerebral perfusion |
|
|
What is the best sign of increased ICP? What is the relationship? |
A decrease in the level of consciousness is the earliest and most reliable sign of increased ICP. Decreased LOC-->increased ICP |
|
|
What is Cushing Reflex? |
CNS ischemic response triggered by ischemia of vasomotor center in brain: increaseding mean arterial BP, widening pulse pressure, reflex slowing of the heart rate (reflex bradycardia) Late indicator of increased ICP; last ditch effort to maintain cerebral circulation |
|
|
What is cerebral edema and what are its effects? What do the effects depend on? What are the types of cerebral edema? |
Cerebral edema=brain swelling Increased tissue volume d/t abnormal fluid accumulation; may or may not increase ICP (because CSF may be displace down or decreased BV to brain) Impact depends on the brain's compensatory mechanisms and extent of the swelling Types: interstitial, vasogenic, cytotoxic |
|
|
What is interstitial edema? What is the condition? |
Associated with an increased in sodium and water content of the peri-ventricular white matter; involves movement of CSF across ventricular wall; water and sodium pass into peri-ventricular white matter Condition: non-communicating hydrocephalus (fluid no longer flows normally and it is pressed across ventricular wall--dispalced) (increased sodium and water content because Na-K pump system has failed at this point from injury) |
|
|
What is vasogenic edema? |
Results from increase in ECF that surrounds brain cells Brain injury leads to blood brain barrier disrupted leads to increased permeability and free diffusion across capillaries Occurs primarily in white matter (more compliant than gray matter and offers less resistance to fluid accumulation) Can displace cerebral hemisphere and cause herniation |
|
|
Manifestations of Vasogenic Edema What conditions can lead to vasogenic edema? |
nMANIFESTATIONS:focal neurologic deficits, disturbances in consciousness, severe intracranialHTNnCONDITIONS:tumors, prolonged ischemia, hemorrhage, brain injury, infectious processes thatimpair function of the blood brain barrier & allow transfer of water &protein into the interstitial space |
|
|
What is cytotoxic edema? |
Involves actual swelling of brain cells; an increase in intracellular fluid primarily in the gray matter but may also be in white matter; a slowly progressive process; may be severe enough to rupture cells and produce cerebral infarction with necrosis |
|
|
How does cytotoxic edema happen? |
Decreased blood flow-->cellular hypoxia-->decreased ATP production, decreased energy stopres-->decreased function of ion pumps-->water entry and cellular swelling Decreased blood flow also leads to cellular hypoxia-->anaerobic metabolism--> increased lactic acid and extracellular acidosis--> water entry and cellular swelling Pre-synaptic hypo-polarization-->opens voltage-gated calcium ion channels--> increased levels free intracellular calcium-->release of neurotransmitters-->membrane potential to threshold-->electrical hyperactivity (seizure) until exhuastion-->electrical silence (death) |
|
|
Manifestations of cytotoxic edema Conditions of cytotoxic edema |
Major changes, stupor, coma Hypo-osmotic states such as water intoxication, severe ischemia that impairs sodium-potassium pump, hypozia, acidosis, brain trauma |
|
|
Cytotoxic edema involves too much of water in the cells |
Lactate, Na+, K+, and H20 |
|
|
Treatment for cerebral edema |
Localized edema surround brain tumprs respons to corticosteroidsl use in generalized edema in controversial Stablize cell membranes and scavenge free radicals Osmotic diuretics may be useful in acute phase of vasogenic and cytotoxic edema when hypo-osmolarity is present |
|
|
Define: consciousness What are it's components? |
State of awareness of self and environment and ability to become oriented to new stimuli Arousal and wakefulness (mediated by RAS); content and cognition (mediated by cerebral cortex in conjunction with RAS) Reflects orientation to person, place, and time |
|
|
What are some of the abnormal levels of consciousness? |
Confusion, delirium, obtundation, stupor, coma |
|
|
Confusion v. delirium |
Confusion: impaired ability to think clearly; inability to perceive, respond to, or remember current stimuli with customary repetition, disorientation Delirium: disturbed consciousness with motor restlessness, transient hallucinations, disorientation and sometimes delusions |
|
|
What is obtundation? |
Decreased alterness with psychomotor retardation |
|
|
What is stupor? |
Not unconscious but exhibits little or no spontaneous activity |
|
|
What is coma? |
Unarousable and unresponsive to external stimuli or internal needs; determined by Glasgow coma scale |
|
|
Types of abnormal rigidity |
Decorticate, Decerebrate |
|
|
What is decorticate? Caused by... |
Upper arms held tightly to sides with elbows, wrists, and fingers flexed Legs extended and internally rotated with feet plantar flexed Caused by destructive lesion of the corticospinal tracts within or very near cerebral hemispheres |
|
|
What is decerebrate? Causes? |
Jaw clenched and neck extended; arms adducted and stiffly extended at elbows, with forearms pronated and wrists and fingers flexed; legs stiffly extended at knees with feet plantar flexed Caused by lesion in diencephalon, midbrain, or pons; may also be caused by severe metabolic disorders such as hypoxia or hypoglycemia |
|
|
Types of abnormal motor responses |
Flaccidity: no motor response exhibited Purposeful movements: localized to pain stimulus-->unconsciously attempting to remove paiunful stimulus Complete flexion: withdraws or flexes extremity indiscriminately in response to painful stimulus Focal motor responses: grasp reflex, sucking reflex, Babinski reflex |
|
|
Types of pupillary responses with what they indicate? |
Unequal or react sluggishly: compression Pinpoint or midpoint fixed: compression of brainstem Dilated, fixed--> compression of CN III Unilateral, fixed-->compression of one CN III |
|
|
What does presence and absence of oculomotor responses indicate? Types of oculomotor reflexes? |
Oculomotor response-->intact brainstem No response>48 hours--> poor prognosis (brain stem) Oculocephalic reflex and oculovestibular reflex |
|
|
Oculocephalic reflex What is normal? Abnormal? |
Doll's eye response Normal: when head turned side to side, eyes rotate together to opposite side Abnormal: eyes rotate together in same direction as hea |
|
|
Oculovestibular reflex What is normal? Abnormal? |
Cold or water caloric test Normal: when ear canal irrigated with water, eyes turn toward side being stimulated Abnormal: absence of eye movement |
|
|
Types of breathing patterns |
Cheyne-stokes; central neurogenic ventilation; apneustic ventilation, cluster breathing, ataxic breathing |
|
|
What is Cheyne-Stokes breathing? Cause? |
Alternating pattern of deep and shallow breathing with periods of apnea; common with diffuse cortical injury or coma from metabolic causes |
|
|
What is central neurogenic ventilation? Cause? |
Regular hyperpneic pattern (continual deep breahting)--> decrease PCO2 and increased pH Common with increased ICP and structural damage to upper brain stem or cerebral cortex |
|
|
What is apneustic ventilation? Cause |
Prolonged inspiratory cycle followed by a 2 to 3 second pause, alternating with a prolonged expiratory cycle Indicates damage to lower pons or high medulla |
|
|
What is cluster breathing? Cause |
Clusters of breaths alternating with irregular periods of apnea Indicates damage to lower pons or high medulla |
|
|
What is ataxic breathing? Cause |
Chaotic respiratory effort; indicates damage to the medullary respiratory control center |
|
|
Hypo- or hyperthermia indicates what... |
Hypothalamic or pituitary injuries or with head trauma |
|
|
What is Cushing's triad? Cause? |
Increased SBP and decreased DBP (widening pulse pressure) and decreased heart rate Occurs with increased pressure on lower brain stem before herniation |
|
|
What is involved with the Glasgow Coma Scale? |
Eye Opening: +4 spontaneous, +3 to call, +2 to pain, +1 none Motor Response: +6 obeys commands, +5 localizes pain, +4 normal flexion (withdrawal), +3 abnormal flexion (decorticate), +2 extension (decerebrate), +1 none (flaccid) Verbal Response: +5 oriented, +4 confused conversation, +3 inappropriate words; +2 incomprehensible sounds; +1 none |
|
|
Types of cerebral circulation |
Arterial blood flow: 2 internal carotids, 2 vertebral arteries-->basilar artery; circle of willis at base of brain Venous blood flow: 2 sets of veins WITHOUT valves, flow depends on gravity and pressure in venous sinuses--> increased ICP --deep cerebral venous system; superficial cerebral veins --2 internal jugular veins |
|
|
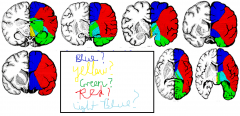
Blue: anterior cerebral artery Yellow: basilar artery Green: posterior cerebral artery Red: middle cerebral artery Light blue: anterior choroid artery |
|
|
Regulation of cerebral blood flow is done through... |
Through autoregulatory or local mechanisms that respond to metabolic needs -Deep cerebral: autoregulatory -Superficial cerebral blood flow: sympathetic-->responsible for vasospasm seen in cerebral aneurysm rupture |
|
|
What are metabolic factors affecting cerebral blood flow? |
Carbon dioxide concentration: 2x CO2= 2x cerebral blood flow Hydrogen ion concentration (pH): extracellular acidosis can also induce vasomotor paralysis Oxygen concentration: decreased oxygen-->increased blood flow |
|
|
Definition of stroke |
n“Clinicalsyndrome consisting of a constellation of neurologic findings, sudden or rapidin onset, which persist for more than 24 hours and whose vascular origins arelimited to thrombotic or embolic occlusion of a cerebral artery resulting ininfarction or a spontaneous rupture of a vessel resulting in intracerebral orsubarachnoid hemorrhage” |
|
|
Key aspects of strokes |
Pathologic process affecting blood vessels that results in occlusion or rupture of blood vessels Resultant damage to brain tissue in area served by occluded or ruptured vessel Neurologic sequelae as a result of interrupted blood flow |
|
|
Types of strokes? How common? |
Ischemic stroke (80%) Hemorrhagic stroke (20%) |
|
|
What is ischemic stroke? |
80% of all strokes; caused by an interruption of blood flow in a cerebral vessel of thrombotic (50%) or embolic (30%) origin; most common type of stroke |
|
|
What is hemorrhagic stroke? |
Caused by bleeding into brain tissue due to hypertension (10%), aneurysms (6%), AV malformation, head iinjury, or blood dyscrasias (abnormal elements in the blood) Less common but higher fatality rate |
|
|
Most common warning signs of stroke: |
Sudden numbness, weakness, or paralysis of the face, arm, or leg; usually on one side of the body; loss of speech, or trouble talking or understanding speech; sudden blurred or decreased vision, usually in one eye; dizziness, loss of balance or loss of coordination; sudden. severe headache with no apparent cause, difficulty swallowing |
|
|
What is a transient ischemic attack (TIA)? Causes? S/S depend on... and may include... |
Characterized by focal ischemic cerebral neurologic deficits that last less than 24 hours, may provide warning of impending stroke; early diagnosis may permit early intervention and prevent extensive damage Causes: atherosclerotic disease and emboli S/S depend on cerebral vessel involved Can include numbness and mild weakness on 1 side of the body; forearm, hand, and angle of mouth commonly affected; transient visual disturbances--graying out, blurring, fogging of vision Rarely: isolated vertigo or dizziness, confusion, amnesia, or seizures |
|
|
Diagnosis of TIA involves: |
CT scan, cerebrovascular arterial imaging, cardiac imaging |
|
|
TIA treatment may involve... |
Depends on type of location; may be pharmacologic (aspirin, antiplatelet drugs, anticoagulants); avoidance of dehydration and hypotension; judicious use of medication to lower BP for HTN; surgery to remove atherosclerotic plaques |
|
|
Surgery types for TIA |
Carotid endarterectomy: indications are one or more TIAs or mild stroke in past 6 months and carotid stenosis>70% Extracranial-intracranial bypass: redirecting blood flow from an artery in the scalp through the cranium to cerebral arteries |
|
|
What is a thrombotic stroke? |
Most common cause of ischemic strokes; usually occur in atherosclerotic blood vessels--primarily at bifurcations, often accompanied by evidence of arteriosclerotic heart disease Not associated with activity--may occur at rest; consciousness may or may not be lost; tend to occur in older persons |
|
|
What are lacunar infarcts? Result from.... Causes? |
Small infarcts located in deeper noncortical parts of the brain or in the brain stem; found in area of deep penetrating arteries supplying the internal capsule basal ganglia, or brain stem Result from occlusion of smaller branches of large cerebral arteries; most commonly middle or posterior cerebral arteries; in process of healing, leave behind small cavities or "lacuna" Causes: embolism, hypertension, small-vessel occlusive disease, hematologic anobormalities, small intracerebral hemorrhages, and vasospasm Do not usually cause profound deficits |
|
|
What is a cardiogenic embolic stroke? Most frequent sites/origin? Predisposing conditions? |
Embolism: moving blood clot Usually affects smaller cerebral vessels, often a bifurcations; most frequent site=middle cerebral artery distribution; most often originate in left heart, may also originate in carotid Sudden onset with immediate maximum deficit Predisposing conditions: rheumatic heart disease, atrial fibrillation, recent MI, ventricular aneurysm, bacterial endocarditis |
|
|
What is ischemic penumbra? Survival depends on... |
Central core of dead/dying cells; surrounded by ischemic area of minimally surviving cells= the "penumbra" (halo) Brain cells in the penumbra receive marginal blood flow, metabolism is altered, and undergoes electrical failure BUT structural integrity of brain cells maintained Survival depends on: return of adequate circulation, volume of toxic products released, degree of cerebral edema, alterations in local blood flow |
|
|
What is a hemorrhagic stroke? What is the most common predisposing factor? Causes? |
Rupture of a blood vessel and bleeding into the brain: leading to edema, compression of brain contents, spasm of adjacent blood vessels Most common predisposing facotr=HTN Causes: aneurysm, spontaneous intracerebral hemorrhage, AV malformations, other includes trauma, erosion of the vessels by tumors, coagulopathies, vasculitis, drugs |
|
|
Acute manifestations of stroke may include... |
Loss of consciousness, cognitive and motor disorders, specific motor and cognitive disorders, specific motor or sensory impairment, aphasia, hemi-neglect syndrome |
|
|
Stroke in the anterior cerebral artery involves what brain areas? |
Infarction of medial aspect of 1 frontal lobe (if distal to communicating artery); bilateral frontal infarction (if flow in other anterior cerebral artery is inadequate) |
|
|
Signs and symptoms of a stroke in the anterior cerebral artery include... |
Paralysis of contralateral foot or leg; impaired gait; paresis of contralateral arm; contralateral sensory loss over toes, foot, and leg; problems making decisions or performing acts voluntarily; lack of spontaneity, easily distracted; slowness of thought, aphasia depends on the hemisphere involved, urinary incontinence, cognitive and affective disorders |
|
|
Brain area in involved in stroke in middle cerebral artery? |
Massive infarction of most lateral hemisphere and deeper structures of the frontal, parietal, and temporal loves; internal capsule, basal ganglia |
|
|
Signs and symptoms of stroke in middle cerebral artery? |
Contralateral hemiplegia (face and arm); contralateral sensory impairment, aphasia; homonymous hemianopsia; altered consciousness; inability to turn eyes toward paralyzed side; denial of paralyzed side or limb (semi-attention); possible acalculia (inability to do calculations); alexia (word blindness); finger agnosia (inability to identify fingers); left-right confusion; vasomotor paresis and instability |
|
|
Brain areas involved with stroke in posterior cerebral artery? |
Occipital love; anterior and medial portion of temporal lobe; thalamus involvement; cerebral peduncle involvement |
|
|
Signs and symptoms of stroke in posterior cerebral artery in occipital love or anterior and medial portion of temporal lobe? |
Homonymous hemianopsia, color blindness, loss of central vision, visual hallucinations, memory deficits, perseveration (repeated performance of same verbal or motor response) |
|
|
Brain area involved with stroke in basilar and vertebral arteries? |
Cerebellum and brain stem |
|
|
Signs and symptoms of stroke in basilar and vertebral arteries? |
Visual disturbances, diplopia (double vision), dystaxia (issues with muscle coordination), vertigo, dysphagia (difficulty swallowing), dysphonia (difficulty speaking) |
|
|
Tools used to may a stroke diagnosis? |
nCompleteHx& Px withthorough neurologic examnComputedTomography (CT)nMagneticResonance Imaging (MRI)nArteriographynMagneticResonance Arteriography (MRA)nPositronEmission Tomography (PET)nSingle-PhotonEmission Computed Tomography (SPECT)nDopplerultrasound (US) |
|
|
Treatments for stroke |
Emphasis on salvaging brain tissue and minimizing long-term disability; window of opportunity for ischemic stroke--use of thrombolytic agents in early treatment; education, early rehabilitation |
|
|
Long-term disabilities in motor deficits with stroke: What areas of brain are affected? What are symptoms? |
With stroke affecting corticospinal tract-->profound weakness on contralteral side Areas: motor cortex, posterior limb or internal capsule, medullary pyramids Symptoms: decrease/absence normal muscle tone, immediate loss of fine manipulative skills, affected limbs tend to move as a whole-->foot drop, outward rotation of leg, dependent edema in affected extremity When muscle tone returns flaccidity replaced by spasticity (6-8 weeks)-->altered limb posturing |
|
|
Long-term disabilities in language with stroke involve what part of the brain |
Involves higher order integrative functions of the forebrain Wernicke's area: understanding language (in dominant temporal lobe) Brochea's area: produces speech (in temporal lobe) |
|
|
Long-term disabilities in language and speech problems with stroke: |
-Disturbancces of the central processing mechanisms of language-->aphasia (language and speech difficulty) -Dysfunction of the larynx, pharynx, palate, tongue, lips, or mouth--> dysarthria (difficult speech) -Inability to sequence of voluntary movements needed for speech despite absence of motor deficits-->apraxia (no purposeful action) |
|
|
What is asphasia? Most common cause? |
Encompasses varying degrees of inability to comprehend, integrate, and express language Most common cause is middle cerebral artery of dominant hemisphere |
|
|
What is receptive or fluent aphasia? Affected area? |
Represents a sensory agnosia or inability to comprehend verbal spoken words--may be visual or auditory Affected area: posterior temporal or lower parietal lobe |
|
|
What is expressive or nonfluent disability post-stroke? Affected area? |
Characteried by inability to translate thoughts or ideas into meaningul speech or writing Affected area: Broca's area (precentral gyrus) of the dominant frontal love |
|
|
What is dysarthria? Cause? |
Imperfect articulation of speech sounds or changes in voice pitch or quality; caused by disturbed motor control |
|
|
What is ataxia? |
Defective muscular coordination |
|
|
What is agnosia? Cause |
Inability to recognize an object--may be tactile, visual, or auditory Involves structural damage to association center of parietal, temporal, and occipital lobes |
|
|
What is alexia? |
Word blindness |
|
|
What is anomia? |
Difficulty recognizing or naming objects or colors |
|
|
What is conduction aphasia? Cause? |
Inappropriate word use despite good comprehhension Results from destruction of fibers connecting Wernicke's and Broca's area |
|
|
What is receptive/fluent changes with stroke? |
Involves appearance of neologisms=invented words |
|
|
What is denial or hemi-attention? |
nnability to analyze & interpretsensory information and internal production of abnormal signals à denial of illness and denial of ½ bodyand surrounding environmentnImpaired spatial orientationnDifficulty localizing stimuli,their own limbs, & objects in spacenMore common in strokes that affectnondominant side of brain (right hemisphere) which is usually involved inspatial orientation, body image, and inductive reasoning |
|
|
A stroke on the right side may result in... |
nWeakness(hemiparesis), paralysis (hemiplegia), or lack of coordination of the face, armor leg on the left side of the body nLackof feeling and position on the left side of the body nDecreasedability to judge distances, size, position, rate of movement and form* nInabilityto think clearly nLossof awareness of forgetting objects on the left side (left-sided neglect). Theneglect is usually more severe with strokes on the right side of the brain nQuickand impulsive behavior Difficultydrawing, dressing, or following a map |
|
|
A stroke on the left side may result in... |
nWeakness(hemiparesis), paralysis (hemiplegia), or lack of coordination of the face, armor leg on the right side of the body nLackof feeling and position on the right side of the body nDifficultyin speaking (slurred or distorted speech), listening, writing, reading,calculating with numbers or understanding what others say (aphasia)* nBehaviorchanges (slow, cautious and somewhat disorganized) nLossof awareness or forgetting objects on the right side |
|
|
What decreases the incidence of embolic stroke? |
Increased treatment of heart disease |
|
|
Symptoms of hemorrhagic stroke |
Occurs SUDDENLY usually when person is active; vomiting is common at onset, sometimes with headache Focal symptoms depends on which vessel is involved Clinical course often progresses rapidly to coma and frequently to death |
|
|
What happens with hemorrhagic stroke with hemorrhage into internal capsule? |
Contralateral hemiplegia with initial flaccidity progressing to spasticity Clinical course often progresses rapidly to coma and frequently to death |
|
|
Acalculia |
Inability to perform calculations |
|
|
Alexia |
word blindness |
|
|
Finger agnosia |
inability to identify fingers |
|
|
Signs and symptoms of stroke in posterior cerebral artery with thalamus involvement? |
Loss of all sensory modalities, spontaneous pain, intentional tremor, mild hemiparesis, aphasia |
|
|
Signs and symptoms with stroke in posterior cerebral artery when cerebral peduncle is involved? |
Oculomotor nerve palsy with contralateral hemiplegia |
|
|
Diplopia |
Double vision |
|
|
Dystaxia |
issues with muscle coordination |
|
|
Dysphagia |
Difficulty swallowing |
|
|
Dysphonia |
Difficulty with speech |
|
|
When are the R and L sides of visual field reversed? |
After they cross at the optic chiasm |
|
|
How is the binocular field divided? Purpose of the divisions? |
Into central and peripheral portions Central portions of retina provide high visual acuity, peripheral portions of the retina provide the ability to detect moving objects |
|
|
What is involved with monocular vision? |
The left peripheral field is seen exclusively by the left nasal retina; the right peripheral field is seen exclusively by the right nasal retina |
|
|
What is anopia? |
a |
|
|
What would occur if there is a lesion in the right optic nerve? |
Right nerve tract will not work; results in unilateral blindness; full vision in left eye and complete blindness in the R eye |
|
|
Hemianopia |
Loss of half of the visual field for one or both eyes |
|
|
What happens if there is a lesion at the optic chiasm? |
If it only involves fibers that originate in the nasal half of each retina, there will be loss of peripheral vision If the entire optic chiasm is affected, there will be complete blindness |
|
|
Temporal v. nasal half of retina |
Temporal is ipsilateral (same side) Nasal is contralateral (crosses) |
|
|
What is homonymous hemianopia? |
Loss of the corresponding visual half-field in each each Interrupts fibers and vision originating on the same side of both eyes (homonymous) with loss of vision from half of each field (hemianopia) |
|

|
bitemporal hemianopsia |
|

|
binasal hemianopsia |
|

|
left homonymous hemianopsia (stroke on the right) |
|

|
right homonymous hemianopsia (stroke on the left) |
|
|
Endocrine glands |
Pituitary, adrenal, thyroid, parathyroid, pancreas, ovaries, testes |
|
|
What is the Hypothalamic-Hypophysial Portal System? |
Hypothalamus nerve endings secrete neurohormones-->blood picks up neurohormones in pituitary stalk--> inflowing blood joins-->all blood follows through portal blood vessels to the secretory cells in the anterior pituitary-->Neurohormones from the hypothalamus stimulate or inhibit the release of anterior pituitary hormones--> anterior pituitary hormones then leave gland in the blood |
|
|
What hormones does the posterior lobe on the pituitary stimulate the release of? Where do these hormones go? |
Antidiuretic hormone (kidney tubules) Oxytocin (uterine muscles and mammary glands) |
|
|
What hormones does the anterior lobe of the the pituitary stimulate the release of? Where do these hormones go? |
Prolactin PRL (mammary glands) Growth hormone GH (bones and muscle tissue) Gonadotrophins: Follice-stimulating hormone FSH and Luteinizing Hormone LH (goes to ovaries and testes to stimulate production of estrogens/progesterone and testosterone, respectively) Adrenocorticotropic hormone ACTH (adrenal cortex and stimulates release of glucocorticoids, mineralocorticoids, androgens) Thyroid stimulating hormone TSH (thyroid--> stimulates release thyroxine, triodothyronine, thyrocalcitonin) Melanocyte-stimulating hormone MSH Somatotropic Growth-Stimulating Hormone STH |
|
|
Where is the pituitary gland located? What is it influenced by? What does it do? |
The master gland located at the base of the brain, influenced by the hypothalamus Directly affects function of other endocrine glands, promotes growth of body tissue, influences water absorption by the kidney, controls sexual development and function |
|
|
Anterior lobe production is also known as... Posterior lobe production is also known as... |
Adenohypophysis Neurohypophysis |
|
|
What are pituitary disorders? |
Anterior pituitary: acromegaly, giantism, dwatfism Posterior pituitary: diabetes insipidus, SIADH (syndrome of inappropriate secretion of antidiuretic hormone) |
|
|
What is acromegaly? When does it usually occur? |
The hypersecretion of growth hormone (GH) by the anterior pituitary gland Acromegaly occurs in middle age, after the closure of the epiphyses of the long bones |
|
|
Assessment of acromegaly would reveal what signs? |
Large hands and feet, visual problems, headache, hyperglycemia (using too much glucose), hypercalcemia, deepened voice, thickening and protrusion of the jaw, increased hair growth, joint pain, diaphoresis, oily/rough skin, mentrual disturbances, impotence Headaches, goiter, enlargement of visceral organs, thickening of skull, cardiomyopathy, diabetes mellitis, enlarged but week skeletal muscles |
|
|
What is involved in caring for someone with acromegaly? |
•Provide emotional support to client•Encourage client to expressfeelings related to altered body image•Provide frequent skin care•Provide pharmacological &nonpharmacological interventions for joint pain•Prepare client for radiation ofpituitary gland if prescribed•Prepare client for hypophysectomy if planned |
|
|
What gland has both endocrine and exocrine function? |
Pancreas |
|
|
What does endocrine function mean? |
Secretion of hormones |
|
|
What does exocrine function mean? |
Secretion of other products into ducts (non-hormonal) |
|
|
What is giantism or gigantism? When does it occur? Assessment would involve what? |
The hypersecretion of growth hormone (GH) by the anteror pituitary gland, occurs in childhood before the closure of the epiphyses of the long bones Overgrowth of long bones, increased height in early adulthood, deterioration of mental and physical status |
|
|
What is involved with carrying for someone with giantism or gigantism? |
•Provideemotional support to client & family•Encourageclient and family to express feelings related to altered body image•Prepareclient for radiation of pituitary gland, if prescribed•Prepareclient for hypophysectomy, if planned |
|
|
What is hypophysectomy? What are possible complications? What is post-operative procedure |
Removal of the pituitary gland Complications include increased ICP, bleeding, rhinorrhea, and meningitis Post-op: Care similar to craniotomy care; monitor vital signs, assess LOC, assess neurological status, monitor for increased ICP, monitor for bleeding, elevate the HOB, Monitor for adrenal insufficiency, Administer corticosteroids asprescribed on time, Monitor fluids and electrolytevalues, Monitor for temporary diabetesinsipidus due to antidiuretic hormone (ADH) disturbances, Avoid water intoxication, Instruct client to avoid sneezing,coughing, and blowing nose•Instruct client in theadministration of prescribed medications |
|
|
What is a characteristic common to all hormones? |
Exert their effects by altering the rate of a body reaction |
|
|
How do target cells respond to a continued decrease in hormone levels? |
Reducing the number of hormone receptors on their cell surface |
|
|
What is dwarfism? When does it occur? Assessment of dwarfism would reveal what? |
Hyposecretion of growth hormone (GH) by the anterior pituitary gland; occurs in childhood Retarded physical growth, premature aging, low intellectual development, dry skin, poor development of secondary sex characteristics |
|
|
What is involved with taking care of someone with dwarfism? |
•Provideemotional support to client and family•Encourageclient and family to express feelings related to altered body image•Prepareto administer hGH(human growth hormone) |
|
|
What is diabetes insipidus? |
The hyposecretion of ADH and a deficiency of vasopressin, results in failure of tubular reabsorption of water in the kidneys |
|
|
What is a tropic hormone? |
Hormone that is released that leads to release of another hormone (not an affect on body) |
|
|
Steps in growth hormone release What opposes growth hormone (counterregulatory)? |
Hypothalamus releases growth hormone releasing hormone to the anterior pituitary, causing release of growth hormone into the body Hypothalamus releases somatostatin that opposes growth hormone effect (also has to do with satiety) |
|
|
With diabetes insipidus, what would be found during assessment? |
Polyuria of 2-24 L per day, polydipsia (abnormally great thirst), dehydraation, decreased skin turgor, dry mucous membranes, inability to concentrate urine, a low urine specific gravity, fatigue, muscle pain and weakness, headache, postural hypotension, tachycardia |
|
|
What is involved with treatment of someone for implementation? |
•Monitor vital signs, neurological& cardiovascular status•Monitor electrolyte values•Administer vasopressin (Pitressin) or DDAVP (desmopressin) asprescribed•Monitor I & O, weight, specificgravity of urine•Instruct client to avoid foods orliquids with a diuretic-type action•Maintain intake of adequate amountsof fluids•Instruct client in administrationof medications as prescribed•Instruct client to wear Medic-Alertbracelet |
|
|
What is Syndrome of Inappropriate Secretion of ADH (SIADH)? |
A disorder of the posterior pituitary gland in which a continued release of the ADH occurs, results in water intoxication |
|
|
What is involved with assessment of someone with syndrome of inappropriate secretion of ADH (SIADH)? |
Changes in LOC, mental status changes, weight gain, hypertension, signs of fluid volume overload, tachycardia, anorexia, nausea and vomiting, hypoatremia |
|
|
What is involved with caring for someone who has syndrome of inappropriate secretion of ADH (SIADH)? |
•Monitor vital signs•Monitor neurological status•Monitor cardiac status•Protect the client from injury•Monitor I&O•Obtain daily weights•Restrict water intake as prescribed•Monitor fluid and electrolytebalance•Administer diuretics and IV fluidsas prescribed |
|
|
Role of adrenal glands |
Regulates sodium and electrolyte balance; affects carbohydrate, fat, and protein metabolism; influences development of sexual characteristics, sustains "fight or flight" response Secrete hormones which help regulate chemical balance, regulate metabolism, and supplement other glands |
|
|
Where is the adrenal cortex? What does it do? |
Outer shell of adrenal gland Synthesizes glucocorticoids (cortisol), mineralocorticoids (aldosterone), secretes small amounts of sex hormones (androgens, estrogens) |
|
|
Where is the adrenal medulla and what does it do? |
Inner core of adrenal cortex Works as part of sympathetic nervous system; produces epinephrine, norepinephrine |
|
|
Disorders of the adrenal glands? |
Adrenal cortex: Addison's disease, Cushing's syndrome, Aldosteronism (Conn's syndrome) Adrenal medulla: pheochromocytoma |
|
|
What is Addison's Disease? |
Hyposecretion of adrenal cortex hormones (glucocorticoids and mineralcorticoids); Condition if fatal if left untreated |
|
|
Assessment of Addison's Disease would include? |
•Weakness•GI disturbances•Weight loss•Emotional disturbances•Bronze pigmentation to skin•Electrolyte imbalances•Hyponatremia•Hyperkalemia•Hypotension•Hypoglycemia•Elevated BUN |
|
|
What is involved with caring for someone with Addison's Disease? |
•Monitor vital signs•Monitor weight and I&O•Maintain fluid and electrolytebalance•Monitor for infection•Instruct client in a high-protein,high-carbohydrate diet•Instruct client in the avoidance ofstress•Instruct client to avoidindividuals with an infection•Instruct client in the need forlifelong corticosteroids•Instruct client to avoidover-the-counter medications•Instruct client to avoid strenuousexercise•Instruct client to wear aMedic-Alert bracelet•Observe for Addisonian crisis secondary to stress,infection, trauma, surgery |
|
|
What is an Addisonian Crisis? What can it cause? What are the symptoms? |
A life-threatening disorder caused by acute adrenal insufficiency; precipitated by infection, trauma, stress, or surgery Can cause hypoatremia, hyperkalemia, hypoglycemia, and shock Severe headache, severe abdominal, leg, and lower back pain, generalized weakness, irritability and confusion, severe hypotension, shock |
|
|
What is involved with caring for someone in Addisonian Crisis? |
•Monitor vital signs•Monitor neurological status, notingirritability and confusion•Monitor I&O•Administer IV fluids as prescribedto restore electrolyte balance•Administer adrenocorticosteroids as prescribed on time schedule•Protect client from infection•Maintain bedrest and provide aquiet environment |
|
|
What is Cushing's syndrome? What is it often the result of? |
A condition resulting from the hypersecretion of glucocorticoids from the adrenal cortex; can result from prolonged administration of corticosteroids |
|
|
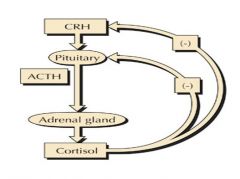
Pathway of cortisol secretion |
|
|
|
Types of hypercortisolism |
ACTH independent: Iatrogenic Cushing's Syndrome (Exogenous steroid acts on pituitary to increase stimulation of cortisol secretion) and Adrenal Tumor (Tumor on the adrenal gland causes too much release of cortisol) ACTH dependent: Cushing's disease pituitary ademona (tumor on pituitary causes too much release of ACTH); Ectopic ACTH (tumor effects adrenal gland to change way ACTH is received) |
|
|
What are signs of Cushing's syndrome? |
•Obesity with thin extremities•Moon face•Buffalo hump•Fragile skin that easily bruises•Hirsutism (masculinecharacteristics in female)•Mood swings•Muscular weakness•Signs of infection•Signs of osteoporosis•Hypertension•Hypokalemia•Hyperglycemia & glycosuria•Elevated white blood cells•Sodium and water retention |
|
|
What is involved with caring for someone with Cushing's syndrome? |
•Monitor I&O•Monitor weight•Monitor glucose levels and urinaryglucose•Provide good skin care•Allow client to discuss feelingsrelated to body appearance•Provide high-protein, low-caloriediet with potassium supplements•Prepare client for adrenalectomy ifprescribed•Prepare client for radiation ifprescribed •Administer hormone replacementtherapy as prescribed•Administer steroids as prescribedif adrenalectomy was performed•Administer chemotherapeutic agentsas prescribed•Instruct client in theadministration of medications as prescribed•Instruct client to avoid infectionand, stress•Instruct client in measures foradequate nutrition and rest |
|
|
What is aldosteronism (Conn's syndrome)? What are the symptoms? |
A hypersecretion of aldosterone from the adrenal cortex of the adrenal gland; due to an adrenal lesion that is usually benign Generalized weakness, increased thirst, nocturia, and polyuria; edema; weight gain, headache, hypertension, positive Chvostek's sign, increased urinary aldosterone, hypokalemia, hypernatremia, metabolic alkalosis |
|
|
What is Chvostek's sign? |
Chvostek's sign is the twitching of the facial muscles in response to tapping over the area of the facial nerveW |
|
|
What is involved with caring for someone with Aldosteronism (Conn's Syndrome)? |
•Monitor vital signs•Monitor weight•Monitor I&O•Assess muscular strength•Monitor for positive Chvostek’s sign•Monitor electrolytes•Maintain sodium restriction asprescribed•Administer potassium supplements asprescribed•Administer antihypertensives, such as spironolactone (Aldactone) as prescribed•Prepare client for surgical removalof tumor if prescribed |
|
|
What does an aldosteronoma cause? |
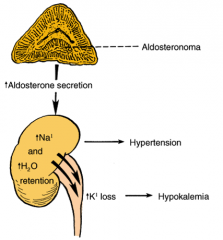
Aldesteronism (Conn's syndrome) |
|
|
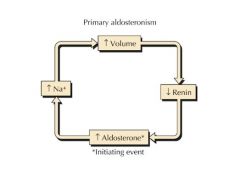
What is involved with primary aldosteronism? |
|
|
|
What is the best measure of fluid volume? |
Daily weight |
|
|
What is a pheochromocytoma? What does it cause? What is treatment? Complication associated Why might it result in death? |
A catecholamine-producing tumor usually found in the adrenal gland but also may be found in the abdomen; typically a benign tumor can be malignant Causes hypersecretion of the hormones of adrenal medulla and the secretion of excessive amounts of epinephrine and norepinephrine Surgical excision of adrenal gland is primary treatment; symptoamatic treatment is initiated if surgical excision is not possible Complication include hypertensive retinopathy and nephropathy, myocarditis, CHF, increased platelet aggregation, and CVA Death can occur from shock, CVA, renal failure, dysrhythmias, and dissecting aortic aneurysm |
|
|
Assessment of someone with a pheochromocytoma would reveal.. |
hypertension and headaches, hypermetabolism, diaphoresis, palpitation and tachycardia, apprehension, emotional instability, hyperglycemia and glycosuria, pain in chest or abdomen with nausea and vomiting, weight loss, fatigue and exhaustion |
|
|
What is involved with caring for someone with pheochromocytoma? |
•Monitor vital signs•Monitor cardiovascular,neurological, and renal status•Monitoring for hypertensive attackssuch as hypertension can precipitate a CVA or sudden blindness•Keep phentolamine (Regitine) at thebedside for hypertensive crisis•Prepare to administer analpha-adrenergic blocking agent, phenoxybenzamine (Dibenzyline), as prescribedto control blood pressure •Be alert to stimuli that canprecipitate a paroxysm, such as increased abdominal pressure, micturition, andvigorous abdominal palpation•Avoid opiates preoperatively asthey can precipitate a hypertensive crisis•Monitor urine for glucose andacetone•Promote rest and nonstressfulenvironment•Provide a diet high in calories,vitamins, and minerals•Prohibit caffeine-containingbeverages and food |
|
|
What is an adrenalectomy? What are post-procedures for bilateral v. unilateral adrenalectomy? What can occur after surgery? |
Surgical removal of an adrenal gland Lifelong steroid replacement is necessary with bilateral adrenalectomy; temporary steroid replacement up to 2 years is necessary for a unilateral adrenalectomy Catecholamine levels drop as a result of surgery, which can result in cardiovascular collapse, hypotension, and shock, and the client needs to be monitored closely; hemorrhage can also occur due to high vascularity of adrenal glands |
|
|
Preoperative implementation from adrenalectomy |
•Prepareclient for surgical procedure•Monitorelectrolytes and correct electrolyte imbalances•Assessfor dysrhythmias•Monitorfor hyperglycemia•Protectclient from infections•Administersteroids as prescribed |
|
|
Postoperative implementation for adrenalectomy? |
•Monitor vital signs•Monitor I&O, and if urinaryoutput is less than 30 mL per hour, notify the physician, as this may beindicative of impending shock and renal failure•Monitor daily weights•Monitor electrolytes•Monitor for signs of shock andhemorrhage, particularly during first 24 to 48 hours•Assess dressing •Monitor for paralytic ileus, asmanifested by abdominal distention and pain, nausea, vomiting, diminished orabsent bowel sounds, as paralytic ileus can develop from internal bleeding•Administer IV fluids as prescribedto maintain blood volume (***) •Administer pain medication asprescribed, remembering that meperidine (Demerol) can cause hypotension•Administer steroid replacement asprescribed•Instruct client in the importanceof steroid therapy following surgery |
|
|
Where is the thyroid gland located? What does it control? What does it produce? |
Located in the anterior part of the neck; controls the rate of body metabolism and growth, produces thyroxine (T4), triiodothyronine (T3), and thyrocalcitonin |
|
|
What do the follicular cells of the thyroid gland do? What do the parafollicular (C-cells) of the thyroid gland do? |
Produce two thyroid hormones: thyroxine and triiodothryonine Produce hormone calcitonin |
|
|
Thyroid hormones released from follicular cells of thyroid gland regulate.... The homrone produced by parafollicular cells of the thyroid gland does what? |
Oxygen use and basal metabolic rate, cellular metabolism, growth and development Calcitonin, helps regulate calcium homeostasis |
|
|
5 Steps in control of thyroid hormone secretion |
1. Low levels of T3 and T4 or low metabolic rate stim hypothalamus to secrete thyrotropin releasing hormone (TRH) 2. TRH enters hypophyseal portal veins and is carried to the anterior pituitary gland, where it stimulates thryotrophs to secrete thyroid stimulating hormone (TSH) 3. TSH stimulates almost all aspects of thyroid follicular cell activity, including iodide trapping, hormone synthesis and secretion, and growth of follicular cells 4.. Thyroid follicular cells release T3 and T4 into the blood until the metabolic rate returns to normal 5. An elevated T3 inhibits release of TRH and TSH |
|
|
What test is used to test for Addison's disease? Results? |
ACTH stimulation test; with normal functioning blood cortisol level will have sharp peak after ACTH injection; with adrenal insufficiency, no spike in blood cortisol level after ACTH injection If you repeat the test and see some improvement, indicates pituitary disease (secondary Addisons), no improvment indicates primary adrenal disease |
|
|
Differences in primary v. secondary adrenal insufficiency |

|
|
|
Primary v. secondary adrenal insufficiency |
With primary: defect is in adrenal gland, does not matter how much ACTH is given, cortisol levels will not change With secondary: defect is in the pituitary, so if you inject ACTH, cortisol will be made |
|
|
Effect of ATP demand on thyroid hormone secretion |
With increased ATP demand (cold environment, hypoglycemia, high altitude, pregnancy) there is increased secretion of thyroid hormones |
|
|
Initial S/S of hyperthyroid Later S/S of hyperthyroid Incidental S/S of hyperthyroid |
Goiter, nervousness/irritbaility, palpatations (tachycardia), unexplained weight loss, diarrhea, sleep disturbances, vision changes (exopthalmos), amenorrhea/oligomenorrhia Tremor, muscle weakness and fatigue, dyspnea, dependent edema, impaired mentation (confusion) Heat intolerance, diaphoresis, increased appetite |
|
|
Initial S/S of hypothyroid Later S/S of hypothyroid Incidental S/S of hypothyroid |
Depression and loss of concentration, dry skin and pruritis, cold intolerance, myalgias, somnolence and fatigue, menorrhagia Goiter, unexplained weight gain, constipation, myxedema, memory loss/impairment Bradycardia, habitual abortion/sterility, impotence, anorexia |
|
|
Altered lab findings for hypothroidism: primary (thyroid), secondary (pituitary), tertiary (hypothalamus) |
Primary (thyroid): Increased TRH, increased TSH, decreased T3/T4 Secondary (pituitary): increased TRH, decreased TSH, decreased T3/T4 Tertiary (hypothalamus): decreased TRH, decreased TSH, decreased T3/T4A |
|
|
Altered lab findings for hyperthyroidism: primary (thyroid), secondary (pituitary), and tertiary (hypothalamus) |
Primary (thyroid): Decreased TRH, decreased TSH, elevated T3/T4 Secondary (pituitary): Decreased TRH, Increased TSH, Increased T3/T4 Tertiary (hypothalamus): Increased TRH, Increased TSH, increased T3/T4 |
|
|
What is the structure involved with primary hypothyroidism and primary hyperthyroidism? Secondary? Tertiary? |
Thyroid, Pituitary, Hypothalamus |
|
|
What is a radioactive iodine uptake (RAI) test? What are normal values? What do elevated values indicate? What do decreased values indicate? |
Thyroid function test that measures the absorption of the iodine isotope to determine how the thyroid gland is functioning; the amount of radioactivity is measured 2, 6, and 24 hours after ingestion of capsule Normal value: 5-35% in 24 horus Elevated values: hyperthyroidism, thyrotoxicosis, decreased iodine intake, or increased iodine excretion Decreased values: low T4, the use of antithyroid medications, thyroiditis, myzedema, or hypothyroidism |
|
|
What is the T3 and T4 resin uptake test? What do findings indicate? |
Blood tests for the diagnosis of thyroid disorders; T3 and T4 regulate thyroid-stimulating hormone Normal t3: 25-35% and T4: 3.8-11.4% T3 elevated in hyperthyroidism and T3 toxicosis, decreases with aging process, and may be decreased in hypothyroidism T4 is elevated in hyperthyroidism and decreased in hypothyroidism |
|
|
What is thyroid-stimulating hormone (TSH) test? What do findings indicate? |
Blood test used to differentiate the diagnosis of primaru hypothyroidism; normal value is 0-6 microunits/mL Elevate values indicate primary hypothyroidism, decreased valued indicate hyperthyroidism or secondary hypothyroidism |
|
|
What is purpose of a thyroid scan? What is involved? |
•Performedto identify nodules or growths in the thyroid gland•Aradioisotope of iodine or technetium is administered prior to the scanning ofthe thyroid gland•Reassurethe client that the level of radioactive medication is not dangerous to selfand others |
|
|
What are disorders of the thyroid gland? |
Hypothyroidism: Cretinism, Myxedema Hyperthyroidism: Graves' disease. thyrotoxicosis |
|
|
Symptoms of hypothyroidism |
Slowing of mind and body, weak heartbeat, constipation, myxedema, high LDL, slow reflexes, hair thinning, depression, "scizophrenia", irritability, big tongue, croaky voice, dry skin, cold skin, cold intolerance |
|
|
Causes of hypothyroidism |
Primary (most common): Hashimoto's throiditis: autoimmune Secondary: failure of HP axis d/t deficient TRH or TSH secretion Also, treatment related (2nd most common)-->radioactive iodine tx or surgery for hyperthyroidism; iodine deficiency; rare inherited enzyme deficiences |
|
|
What is primary hypothyroidism v. secondary hypothyroidism |
Primary: Thyroid can't produce the amount of hormones the pituitary is calling for Secondary: Thyroid isn't being stimulated by pituitary to produce hormones |
|
|
What is cretinism? What are the symptoms? |
A severe thyroid hypofunction that results in hyposecretion of thyroid hormones in the fetus or soon after birth Pot belly with umbilical hernia, sensitivity to cold, severe physical and mental retardation, dry skin, coarse, dry, brittle hair, slow teething, large tongue, poor appetite, constipation, yellowish coloration to skin |
|
|
What is involved with caring for someone with cretinism? |
•Provide emotional support•Provide warmth and skin care•Prevent injury•Prevent constipation•Encourage parents to discussfeelings regarding the disorder•Administer hormone replacement ofdesiccated thyroid, thyroxine (Synthroid), or triiodothyronine (Cytomel) as prescribed•Instruct parents regarding theadministration of medication |
|
|
What is Trosseau's sign? |
When blood pressure is pumped on arm, causes flexing of fist inwardW |
|
|
What is myxedema? What are symptoms? |
A hypothyroid state resulting from hyposecretion of thyroid, condition occurs in adulthood •Slowed rate of body metabolism•Lethargy and fatigue•Intolerance to cold•Weight gain•Dry skin and hair; loss of bodyhair•Bradycardia•Constipation•Generalized puffiness and nonpitting edema•Forgetfulness and loss of memory•Menstrual disturbances•Cardiac disorders |
|
|
What is involved with caring for someone with myxedema? |
•Monitor vital signs•Monitor for cardiac complications•Administer & monitor thyroidreplacement of desiccated thyroid, thyroxine (Synthroid) or triiodothyronine (Cytomel) as prescribed•Instruct client in low-calorie,low-cholesterol, low-saturated fat diet•Assess client for anorexia &fecal impaction•Provide roughage & fluids toprevent constipation•Provide a warm environment for theclient•Avoid sedatives & narcotics dueto intolerance•Monitor for overdose of thyroidmedications, characterized by tachycardia, restlessness, nervousness, &insomnia |
|
|
What is a myxedema coma? Causes? Symptoms? |
A rare but serious disorder that results from a persistent, low thyroid production; can be precipitated by acute illness, rapid withdrawal of thyroid medication, anesthesia and surgery, hypothermia, and use of sedatives and narcotics Hypotension, hypothermia, bradycardia, mental depression, mood swings, hyponatremia, hypoglycemia, coma |
|
|
What is hyponatremia? |
Not enough sodium in the blood |
|
|
What is the implementation for someone in myxedema coma? |
•Maintain a patent airway•Monitor vital signs and LOC•Assess client’s temperature frequently•Assess blood pressure•Administer IV fluids as prescribed•Monitor electrolytes and glucoselevel•Administer IV glucose as prescribed•Keep client warm•Monitor for changes in mentalstatus•Administer levothyroxine sodium IVas prescribed•Administer corticosteroids asprescribed•Avoid the use of sedatives andhypnotics |
|
|
Symptoms of hyperthyroidism |
Wide pulse pressure, "lid lag", strong rapid pulse, sweating, "neurotic anxiety", fine tremor, brisk reflexes, low LDL, diarrhea, weight loss despite increased appetite, osteoporosis, atrial fibrillation |
|
|
What is Graves disease? Symptoms? |
•Ahyperthyroid state resulting from a hypersecretion of thyroid hormone •Alsoknown as thyrotoxicosis •Increased rate of body metabolism•Enlarged thyroid gland (goiter)•Cardiac dysrhythmias, such astachycardia and palpitations•Protruding eyeballs (exophthalmos)•Hypertension•Heat intolerance•Diaphoresis•Weight loss•Smooth, soft skin and hair•Nervousness and fine tremors ofhands•Personality changes•Irritability & agitation•Mood swings |
|
|
Exopthalmos v. proptosis? |
Protruding eyeballs, sunken eyeballs
|
|
|
Implementation for someone with Graves' disease |
•Provide adequate rest•Administer sedatives as prescribed•Provide cool and quiet environment•Obtain daily weights•Provide a high-calorie diet•Avoid stimulants•Provide psychosocial support •Administer antithyroid medications, methimazole (Tapazole), or propylthiouracil, which blocks thyroid synthesis,as prescribed•Administer iodine preparations, Lugol's solution, saturated solution ofpotassium iodide (SSKI), which inhibits the release of thyroid hormone, asprescribed•Administer propranolol (Inderal)for tachycardia as prescribed•Prepare the client for radioiodinetherapy as prescribed to destroy thyroid cells•Prepare client for thyroidectomy ifprescribed |
|
|
What is a thyroid storm? Symptoms? |
•Anacute and fatal thyroid condition that occurs from manipulation of the thyroidgland during surgery and the release of thyroid hormone into the bloodstream•Itcan also occur from severe infection and stress •Fever•Diaphoresis•Dehydration•Tachycardia•Congestive heart failure andpulmonary edema•Nausea, vomiting, and diarrhea•Systolic hypertension•Tremors•Irritability, agitation, andrestlessness•Delirium and coma |
|
|
Implementation for someone with a thyroid storm? |
•Monitor vital signs•Decrease temperature, avoiding theuse of salicylates as they increase free thyroid hormone levels•Avoid palpating thyroid gland•Monitor I&O•Monitor fluid and electrolytebalance•Monitor for dehydration and overhydration•Monitor pulmonary and cardiacstatus •Administer iodine preparations, Lugol's solution, or saturated solution ofpotassium iodide (SSKI), which inhibits the release of thyroid hormone, asprescribed•Administer propranolol (Inderal)for tachycardia and to reverse toxic manifestations of thyroid storm asprescribed•Administer glucocorticoids asprescribed to allay stress effects•Administer cardiac medications asprescribed to decrease heart activity |
|
|
What is a thyroidectomy? Why would it be performed? |
•Removalof the thyroid gland•Performedin conditions where persistent hyperthyroidism exists |
|
|
What are preoperative implementations for thyroidectomy? |
•Obtain vital signs •Obtain weight •Assess electrolyte levels•Assess for hyperglycemia andglycosuria•Assess level of consciousness•Assess for signs of thyroid storm•Administer antithyroid medications as prescribed todeplete iodine and hormones•Administer iodine as prescribed todecrease vascularity of the thyroid gland |
|
|
Postoperative implementations for thyroidectomy? |
•Monitor for respiratory distress•Have tracheotomy set, oxygen, andsuction at the bedside•Maintain semi-Fowler's position•Monitor for signs of bleeding•Check dressing anteriorly and atthe back of the neck•Limit talking and assess level ofhoarseness•Monitor for laryngeal nerve damage,as evidenced by respiratory obstruction, dysphonia, high-pitched voice,stridor, dysphagia, and restlessness•Monitor for signs of tetany, whichcan be due to trauma to the parathyroid gland•Prepare to administer calciumgluconate as prescribed for tetany |
|
|
What are signs of Tetany? |
•Positive Chvostek’s sign•Positive Trousseau’s sign•Numbness of extremities and spasmof glottis •Irritability•Wheezing and dyspnea•Visual disturbances•Muscle and abdominal cramps |
|
|
Where is the parathyroid gland located? What does it do? |
Located near the thyroid, controls calcium and phosphorus metabolism; produces parathyroid hormone (PTH) |
|
|
What are disorders of the parathyroid gland? |
•Hypoparathyroidism•Hyperparathyroidism |
|
|
What is hypoparathyroidism? Symptoms? |
•Acondition caused by hyposecretion of parathyroid hormone by theparathyroid gland•Occursfollowing thyroidectomy from removal of parathyroid tissue •Hypocalcemia and elevatedphosphorus levels•Numbness and tingling ofextremities•Cramping•Signs of tetany, such as muscularspasms, irritability, seizures, positive Trousseau’s sign, positive Chvostek’s sign, laryngospasm, and cardiacdysrhythmias •Signsof hypocalcemia, such as weakness and tingling of the extremities, painfulmuscle spasms, dysrhythmias, irritability, and anxiety •Increasedneuromuscular irritability •Confusion•Visualproblems•Depression |
|
|
Implementation for someone with hypoparathyroidism |
•Monitor vital signs•Monitor cardiac status•Monitor for tetany•Initiate seizure precautions•Place a tracheotomy set, oxygen,and suctioning at the bedside•Provide a high-calcium,low-phosphorus diet•Provide quiet environment with nostimulus•Administer aluminum hydroxide asprescribed to decrease phosphate levels•Administer parathyroid hormone asprescribed•Prepare to administer IV calciumgluconate for hypocalcemia•Instruct client in theadministration of calcium carbonate (OsCal) and vitamin D (Calciferol) as prescribed |
|
|
What is hyperparathyroidism? Symptoms? |
Condition caused by hypersecretion of parathyroid hormone by the parathyroid gland •Bonedeformities•Fractures•Calciumdeposits in organs•Gastriculcers•Nausea,vomiting, anorexia, constipation•Personalitychanges•Polydipsiaand polyuria•Elevatedcalcium and low phosphorus levels |
|
|
Implementation for someone with hyperparathyroidism |
•Monitor cardiac function•Monitor renal status•Monitor I&O•Provide hydration•Monitor fluid and electrolytebalance•Monitor calcium and phosphoruslevels•Administer furosemide (Lasix) asprescribed to lower calcium levels•Administer IV saline as prescribedto lower calcium levels•Notify physician immediately if aprecipitous drop in the calcium level occurs•Assess client for tingling andnumbness in the muscles, which is caused by a sudden drop in calcium levels•Administer phosphates asprescribed, which interfere with calcium absorption•Administer calcitonin (Calcimar) as prescribed to decreaseskeletal calcium release and increase renal clearance of calcium•Administer cytotoxic antibiotics asprescribed to lower calcium levels, and monitor client closely forthrombocytopenia and renal and hepatic toxicity•Prepare client forparathyroidectomy as prescribed |
|
|
What is a parathroidectomy? What are preoperative implementations? |
Removal of one or more of the parathyroid glands •Monitor electrolytes, calcium,phosphate, and magnesium levels •Ensure calcium levels are decreasedto near- normal•Inform client that talking may bepainful for the first day or two postoperative |
|
|
Postoperative implementations for parathyroidectomy? |
•Monitor for respiratory distress•Place a tracheotomy set, oxygen,and suctioning at the bedside•Monitor vital signs•Position client in semi-Fowler’s•Assess neck dressing for bleeding,1 to 5 mL of serosanguineous drainage is expected•Monitor for hypocalcemic crisis, as evidenced by tinglingand twitching in the extremities and face•Assess for positive Trousseau's andChvostek’s sign, which signals the potential oftetany•Monitor for laryngeal nerve damage•Monitor for changes in voicepattern and hoarseness•Instruct client in theadministration of calcium and vitamin D as prescribed |
|
|
What is counteractive to parathyroid hormone? |
Calcitonin secreted from C cells of the thyroid gland |
|
|
Is goiter in hyper- or hypo- thryroidism? |
Both--> initial S/S in hyperthyroid, later S/S in hypothyroidism |