![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
222 Cards in this Set
- Front
- Back
|
Diabetes will show what signs in the eyes? Thyroid issues? |
Retinal hemorrhages; bulging eyes |
|
|
What is a white ring around the eye called? What is it indicative of? |
Arcus senilis; indicative of high cholesterol |
|
|
What is xanthoma? What might it indicate? |
Looks like skin tags in eye on bottom conjunctiva; may indicate lipid problem |
|
|
What is normal vision change in those over 40? |
Depressed myopia: difficulty accommodating to close-up objects |
|
|
What do halos in vision indicate? |
Acute primary angle (closed) glaucoma--> MEDICAL EMERGENCY (indicates innerocular pressure that suddenly occurs, no exchange of fluid) |
|
|
What is red reflex? |
When light is shined in the eye, should see redness reflected from eye as the eye reacts |
|
|
Important steps in given eye drops |
Should use separate R and L eye drop applicator; need to change gloves and do hand hygiene between each eye |
|
|
What is a cataract? How do they form? What are steps in formation? |
Acataract is characterized by a clouding of the eye's lens, which impairsvision. The lens is made up mostly of water and protein. A cataractoccurs when this protein clumps together and prevents some light form reachingthe retina. When first forming, a cataract may affect only a small areaof the lens and may not interfere with eyesight. However, as a cataract grows,in canseverely impair your vision, and treatment becomes necessaryolda); b = safe_add(b, oldb); c = safe_add(c, oldc); d = safe_ |
|
|
Signs of symptoms of cataract? |
Themost common symptoms of a cataract are:cloudyor blurry vision seeinghalos around lights difficultyadjusting to bright light poornight vision frequentchange in eyeglass prescriptions |
|
|
Changes in vision from birth to school age children |
Infants: hyperopic visual 20/200 School age: 20/20 Peripheral vision developed at birth; Central vision develops later |
|
|
How are cataracts treated? |
Inthe early stages of a cataract, eyeglasses, magnifying lenses, or strongerlighting may be effective in improving vision. When these tactics fail,surgery is usually required. In cataract surgery, the lens of the eye isremoved and replaced by an artificial lens. This new lens allows light to passthrough to the retina, restoring vision. Cataract surgery is one of themost common surgeries preformed in the United States. In fact, more than1 million procedures are performed each year, and more than 95% of thesesurgeries are considered successful.:/QZ 8u[DuM5`;J~`u$0E |
|
|
Who is at risk for a cataract? |
Themost common type of cataract, age-related cataract, affects more than half ofall Americans 65 years and older. |
|
|
What is presbyopia? When is it common? |
Difficulty accomodating; 70 years old |
|
|
Vision changes in older adults |
Presbyopia; visual disturbances with night vision, smaller pupil, cataracts common; dry eye common |
|
|
Important considerations for enhancing vision in older adults |
Those >60 require 2 times more illumination for close tasks compared to the average 20 year old. Avoid monochromic colors (blue, green, violet) because the older person will have difficulty discriminating borders. |
|
|
Eye Exam requires |
Snellen Chart, Jaegar Card, Occulder, Penlight, Opthalmoscope |
|
|
Entropian v. Ectropian |
Entropian: lid goes in Ectropian: lid goes out |
|
|
What do we assess lacrimal apparatus for? |
Redness, swelling, and tenderness |
|
|
What is the cornea? What do we evaluate? |
Anterior outer layer that covers pupil and iris Shine light from side; check smoothness, clarity, no breaks |
|
|
What is the iris and pupil? How do we assess them? |
Iris flat, round even color Note pupil size, shape, equality |
|
|
What is Brushfield spots? |
White specks in the iris; sign of Down Syndrome |
|
|
What is PERRLA? How do we test it? |
Pupils Equal Round Reactive Light Accommodation For Pupillary light reflex: darken room, patient looks straight ahead, brng light to side, check direct and consensual response--document in mm. For accomodation: constriction and convergence-- have patient look distant (pupils will dilate), have patients look at object 3 inches from eyes (pupils will constrict with closeness) |
|
|
What are the 2Ds and 3Cs of accomodation? |
2ds: distance-->dilate 3Cs: close, converse, contrict |
|
|
Normal pupillary size to light reflex |
Usually 3-5 mm |
|
|
How is Snellen Chart used? What do results indicate? |
Tests distance vision, stand 20 feet away, leave contacts and glasses, cover one eye, have pt read the smallest line of print Normal=20/20 Numerator=distance from chart (should be 20) Denomintor= distance normal eye could read chart |
|
|
How is a Jaeger Card used? What are normal results? |
Hold card 14 inches away, test eyes individually with glasses; can test myopia and hyperopia Normal: 14/14 in each eye |
|
|
What is the confrontation test? What is normal? What should be documented? |
0Measureof peripheral vision – practitioner’s visual field MUST be normal.0Advancingfrom periphery with finger, slightly behind patient0NORMAL= 50 degrees upward, 90 degrees temporal, 70 degrees down, 60 degrees nasal.0DOCUMENT: Visual fields intact. |
|
|
Extraocular muscle function involves testing what cranial nerves? |
III, IV, VI |
|
|
What is corneal light reflection test? What is normal result? What would documentation be like? |
Assess alignment of eyes, patient looks straight ahead, reflection of light on corneas Normal is symmetric If abnormal then do cover/uncover test (when uncovering, may see drifting of eye "lazy eye") Document: Corneal light reflex bilateral alignment noted |
|
|
What is the cover/uncover test for extraocular muscle function? What are normal findings? |
Patient looks straight ahead at distant object; cover one eye (look at uncovered eye--> normal=fixed); uncover the eye--look at eye that was covered (normal=eye should not move and should also be looking in the same direction); repeat with other eye |
|
|
What are cardinal positions of gaze? What is normal? What should you watch for? |
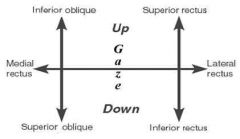
Patient keeps head still and follow finger or penlight with eyes ONLY; move in 6 position--H position Normal-tracking with BOTH eyes Watch for: Lateral gaze, nystagmus |
|
|
Care of eyes includes: |
0Clean frominner to outer canthus with wet, warm cloth, cotton ball, or compress0Use artificialtear solution or normal saline every 4 hours if blink reflex is absent – ifordered by physician00Care foreyeglasses, contact lens, or artificial eye if indicated |
|
|
How do blood vessels in eyes differ from the rest of vessels in body? |
Veins are larger in the eyes than arteries |
|
|
Steps for instilling eye drops |
0Wash Hands0Glove0OfferTissues0CleanEye / Eyelids / Eyelashes0Tilthead back0Holdthe dropper close but DON’T touch eye0Letdrop(s) fall in as prescribed in the conjunctival sac0Presslightly on inner canthus to decrease systemic effect. |
|
|
Steps for applying eye ointments |
0Perform6 rights for medication Administration0WashHands0Wear Gloves0CleanEye / Eyelids / Eyelashes0Tilthead back0Applypressure downward to expose lower eye0Applyprescribed amount along the conjunctival sac0Closeeyes gently |
|
|
What is the main function of the ears? |
Hearing and equilibrium |
|
|
How do sound waves travel through ear? |
Move through the external, middle, and internal ear to stimulate CN VIII; then transmit the impulses to the temporal lobe for sound interpretation Equilibrium is maintained through the vestibule of the inner eye |
|
|
Conductive v. sensorimotor hearing |
Conductive: transmission of sound through external to middle ear Sensorineural: transmission of sound in inner ear |
|
|
How are Eustachian tubes different in children? |
Less air-filled than adults |
|
|
Signs of hearing loss |
Repeating statements, straining, leaning forward, tilting head, shouting in conversation, raising volume, avoiding large groups |
|
|
Ear assessment considerations for infants and children |
Observe ear placement, hearing tests done prior to discharge, ear infections |
|
|
Ear assessment considerations for young and middle-adults |
Excessive or chronic noise exposure |
|
|
Ear assessment considerations for older adults |
Common hearing losses, presbycusis, stiffening of colia causing cerumen to accumulate |
|
|
Objective data examination of ear steps |
0Patientin sitting position0Inspection& palpation of external ear0Palpatefor Tenderness0Palpateear structures ( tragus, helix & mastoid process0Size& Shape0Positioningof Ear0Conditionof skin0Color0Drainage |
|
|
Steps in using otoscope |
Useshortest and largest speculumTilthead to opposite shoulderHoldpatient’s head and hold otoscope with handle up.Pullhelix up and back for adult – insert in ½ inchPullhelix straight back >3 yearsPullear lobe down & back for children under 3 and insert ¼ inch.Viewexternal ear canalAssessthe TM If unable to visualize a cerumen scoop can beused to clear canalNEVER irrigate the canal, unless drumis intact~uHi: |
|
|
What is involved when looking at tympanic membrane in an otoscopic exam? |
Note color, intactness of drum; normal is opaque pearl gray, slight concave, should see cone of light at 5 o'clock on the right, 7 o'clock on the left; assess mobility of drum (should be flat) |
|
|
What does cone of light deviation in the tympanic membrane indicate? |
Can tell us that there is pressure behind the tympanic membrane |
|
|
What is conductive hearing loss? What can cause it? |
Occurs when there is physical obstruction to the transmission of sound waves Cerumen, tumors, ossicles (scar tissue buildup) |
|
|
What is sensorineural loss? What can cause it? |
Due to defect in the organ of corti, CN VIII, or the brain Infections, surgery, DM, medications, trauma, CN VIII damage |
|
|
Result of mixed conductive and sensorineural hearing loss |
Results in severe profound hearing loss |
|
|
What is the Whisper test? |
Hearing test, also called voice test Stand about 1-2 feet behind and whisper, having patient cover one ear, patient should repeat |
|
|
What is the Watch Test? |
Hearing test; holding ticking watch within 5 inches, cover other ear; difficulty often noted in elders |
|
|
What is the Weber test? What is normal? Abnormal? |
Hearing test, involves placing tuning fork on top of patient's head Normal: tone heard midline without lateralization Conductive: Generally lateralizes to ear that does not hear as well Sensorineural: laterized to ear that does not hear as well |
|
|
What is the Rinne test? Normal? Abnormal? |
Place vibrating tuning fork on mastoid process, count time it is heard; have patient signal when sound stops; move to the front of the ear, the length of time AC (in front of ear)>BC (behind ear) in 2:1 ratio Sensory loss: still 2:1 ratio, but both shorter Conductive loss: bone heard longer than in front of ear (decreased ratio) |
|
|
What is Romberg's test? What might be indicated? |
Patient stands with feet together; stand nearby and note patient's ability to maintain balance Vestibular changes may be indicated by swaying (some is normal) |
|
|
Steps in administering ear drops |
0Perform 6rights for medication Administration0Wash Hands0Glove0Positionpatient / affected ear toward you / Unaffected ear is down0Clean anydrainage0Again check 6rights0Stabilizerdropper hand to avoid ear canal damage0Straighten earcanal and instill drops0Have patientremain for 5-10 minutes to allow medication to go into ear canal. |
|
|
What is epistaxis? |
Hemorrhage from nose, most commonly anterior septum, can be serious problem resulting is significant blood loss or airway compromise |
|
|
What is leukoplakia? |
Whitish patch in mouth where smokeless tobacco has been used, can quickly turn into cancer |
|
|
Aspects of headache evaluation |
Onset, duration, location, character, severity, presence of visual prodromal event, pattern, associated symptoms, precipitating facts, efforts to treat |
|
|
What is photophobia? Phonophobia? |
Sensitivity to light; sensitivity to sound |
|
|
Types of headaches |
Sinus: pain is usually behind the forehead and/or cheekbones Cluster: pain is in and around one eye Tension: pain is like a band squeezing the head Migraine: pain, nausea, and visual changes are typical of classic form |
|
|
How is symmetry of the face assessed? |
Comparing naso-labial folds (smile lines) and palebral fissures (under eye lines) |
|
|
What causes microcephaly? Macrocephaly? |
Micro: Zika, fetal alcohol syndrome, sometimes Down's syndrome Macro: acromeglia, hydrocephaly |
|
|
How are sinuses evaluated? |
Transillumination, palpation, percussion |
|
|
What is turbinence? What do color differences indicate? |
Inner part of the nose; normal is pink, if infected, will be red, allergies could result in light blue |
|
|
How are nasal sprays used? |
Occlude one nostril, aim to outside of nostril, take short respirations in |
|
|
Rhinitis and Sinusitis |
Rhinitis: Enlarged nasal mucosa, occluded sinus openings, edemalous conchae, polyps may develop, discharging mucus Rhinosinusitis: Thick mucus occludes the sinus cavity prevents drainage |
|
|
Treatment of epistaxis |
Topical vasoconstrictors: adrenaline, cocaine, phenylephrine Packing of nasal cavity or balloon catheter |
|
|
Nursing care of patients with epistaxis |
Assessment of bleeding, monitor airway, breathing; vital signs; reduce anxiety; patient teaching-->avoid nasal trauma, nose picking, nose blowing, pressure on nose to stop bleeding; if bleeding does not stop in 15 minutes, seek medical attention |
|
|
What is torticolis? |
Neck muscles have shortened so they cannot move their head back into place (requires immediate PT)--> head stuck looking sideways, head over shoulders |
|
|
What are the salivary glands? |
Sublingual gland, submandibular gland, parotid gland |
|
|
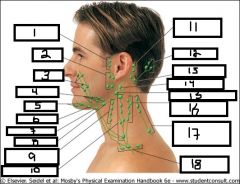
Preauricular nodes, parotid, facial, submandibular, submental, sublingual, suprahyoid node, thyrolinguofacial, anterior deep and superficial servical, internal jugular chain, posterior auricular (mastoid nodes), occipital nodes, sternomastoid nodes, external jugular, retropharyngeal (tonsilar), posterior cervical spinal nerve chain, posterior superficial cervical chain, supraclavicular nodes |
|
|
What is involved with assessment of thyroid? |
Inspection, palpation, and auscultation Check for masses, scars, and lesions (trauma) Atrophy, hypertrophy Exopthalamos (bulging eyes) Goiter |
|
|
Categories of cancers of the larynx |
Supraglottic: false vocal cords above vocal cords Glottic: true vocal cords Subglottic: below vocal cords |
|
|
Key signs of hypocalemia from a hypothyroidism issue |
Trosseau's sign (fist clenches when BP cuff inflated), parethesias (tingling or pins and needleS), Chvostek's sign (twitching of facial muscles in response to tapping over the area of the facial nerve) |
|
|
Definition of Law |
Standard orrule of conduct established and enforced by government; Designed toprotect the rights of the public |
|
|
Public v. private v. criminal law |
Public law: government directly involved; regulates relationships between individuals and government Private law: civil law, regulates relationships among people Criminal law: concerns state and federal criminal statutes--defines criminal actions |
|
|
Reasons for suspending or revoking licenses in nursing |
0Drug oralcohol abuse0Fraud,deceptive practice0Criminal acts,previous disciplinary actions0Gross orordinary negligence0Physical ormental impairments including age |
|
|
What is tort? Types? |
A Wrong committed by a person against another person of or his or her property; tried in civil court Can be intentional or unintentional |
|
|
Misdemeanor v. felony |
Misdemeanor: punishable by fines or less than 1 year imprisonment Felony: punishable by imprisonment for more than 1 year |
|
|
Types of intentional torts |
Assault and battery, defamation of character, invasion of privacy, false imprisonment, fraud |
|
|
Types of unintentional torts |
Negligence, malpractice |
|
|
Types of technical safeguards in nursing care |
Access control, audit controls, integrity controls, and transmission security |
|
|
Most common form of medication error Most common cause of medication errors |
Omitted doses Transcription errors |
|
|
Single most preventable cause of patient injury |
Medication errors |
|
|
Types of Medication Errors |
Prescribing errors, dispensing errors, administration errors |
|
|
Prescribing errors include: |
nincorrectdrug dose, strength, route, quantitynfailureto comply with legal requirements for prescription writing. The prescriber mustspecify the information which the pharmacist needs to dispense the drug in thecorrect dosage and form nadversepatient effects, drug allergies, wrong drug name, dosage form or abbreviation nincorrectdosage calculations nincorrectfrequency |
|
|
What are dispensing errors? |
nDispensingerrors are errors that occur at any stage during the dispensing process fromthe receipt of a prescription in the pharmacy through to the supply of adispensed product to the patient. |
|
|
Dispensing errors include: |
ntheselection of the wrong strength/product (two or more drugs have a similarappearance or similar name)nTheuse of computerized labeling which has led to the emergence of transpositionand typing errors which are now among the most common causes of dispensingerror nwrongdosenwrongdrugnwrongpatient |
|
|
What are administration errors? Examples of this type of error? |
Occurs when there is a discrepancybetween the drug therapy received by the patient and the drug therapy intendedby the prescriber. largely involve errorsof omissionwhere administration is omitted due to a variety of factors e.gwrong patient, lack of stock Othertypes of drug administration errors include: wrong administration technique administration of expired drugs wrong preparation administered
|
|
|
Contributing factors to prescribing error occurrence: |
nIllegiblehandwriting nInaccuratedrug history taking nDrugname confusionnInappropriateuse of decimal points nUseof abbreviations nUseof verbal orders |
|
|
What does IX ss stand for? |
9.5 |
|
|
Formula for calculating IV drip rate |
(Total amount to be infused (ml)/total time to be infused (min)) x drip factor= # gtts/min |
|
|
General rules for medication administration |
1. Before giving any drug, nurse must befamiliar with the drug, generic and trade names, usual dosage, route ofadministration, anticipated results and toxic effects. 2. Check if patient has any allergies 3. Student must check originalphysicians order against the medication sheet before giving any med. Consultthe charge nurse or doctor if a written order is not clear. To be complete, order must containmedication, dosage, frequency, route, and patient name. Orders must be dated and timed and must besigned by the provider. |
|
|
Six rights in giving medication Seventh? |
the right patient; the right time; theright medicine; the right dose; the right method of administration (route); andthe right documentation Right reason |
|
|
Establishing the right time step for medication administration includes |
(a) What time IS it (b) Has it been signed for as given (c) Is the drug time-limited |
|
|
Excess medication from stock supply refused by a patient should be discarded per agency EXCEPT for: |
1. Controlled drugs must be saved to verify the correct count 2. Unopened unit doses may be returned to drawer |
|
|
How does medication administration change once a patient goes to the operating room? |
All medication orders are discontinued and new orders must be written post operatively by physician |
|
|
How is error in medication reported? |
Reported immediately to the instructor and nurse in charge. Fill out incident report |
|
|
How is the step of confirming right patient made when administering medications? |
Asking his/her name and DOB and checking the identification band against the MAR |
|
|
When is medication administration recorded? How? |
nMedicationis recorded by the nurse AFTER ADMINISTERING THE DRUG. Sign initials on med sheet but also use legalsignature and title on bottom of med sheet or a designated “signature sheet”,e.g., "Susan Murphy, SUNY-SN" and not"S. Murphy" or "Sue Murphy". |
|
|
Special considerations for administration of controlled medications |
nControlledmedications (e.g. narcotics, hypnotics) must be double‑locked in a stationarycupboard at all times. Controlled drugsmust be signed for on a registry or computer at the time they are removed fromthe locked cupboard. |
|
|
What happens with surplus of medication? |
nSurplusof medication should be returned to the pharmacy for billing credit after orderis discontinued or patient is discharged. A nurse may NOTgive these medications to patient/family to take home. |
|
|
What is the red box rule? |
When someone is passing medication, they are in a "red box"--> they should not be interupted or distracted unless it is an emergency |
|
|
Types of drugs that are time limited? What does time limited mean? |
Time limited=can only be given for certain number of days and then must be reordered by physician Controlled substances, antibiotics, anticoagulants, steroids |
|
|
Steps in Administration of Oral Medication |
1. Checkmedication order: Compare med sheet withoriginal doctor's order. Considerany adverse effects of drug or combination of drugs. Know generic and trade names. Know Pregnancy category & DEA Schedule. Know if drug is time limited. 2. Check allergies. 3. Perform hand hygiene. 4. Go to medication supply (drawer, cart, computer system). 5. Remove medication from supply, read label (1st time) and compared with med sheet. If a locked control drug, sign for it in appropriate book. 6. Calculate dose if necessary; validate. 7. Choose appropriate container (paper, plastic med cup) 8. Reread medication label (for 2nd time) 9. Once med is prepared, it MUST remain in your sight until administered. 10. Read label (for 3rd time) before returning medication to drawer by comparing med sheet with medication prepared 11. Six patient rights: right drug, right dose, right route, right time, right patient, right documentation (and right reason) 12. Clean area and return contain to drawer 13. Identify patient 14. Place patient in suitable position for swallow. 15. Provide liquid with which patient will swallow medication. 16. Assist patient as necessary. 17. Remain with patient until all swallowed. 18. Document medication given. If refused, document reason. 19. Check on patient in 30 minutes if possible. |
|
|
Steps in preparing for tablet or capsule from multi-dose supply |
a. Pour or tap required number into containercap. b. Transferto paper or soufflé cup. c. Forcertain medications, pour into separate cup (e.g., digitalis preparations). d. Donot touch with fingers or palm of hand. e. Donot return excess to bottle by touching (pour ortap it in). f. Only break scored tablets. Do not crushenteric coated tablets. |
|
|
Steps in preparing for liquid medication |
nIs it a solution or suspension.Adequately shake a suspension.nPour away from the label intoplastic calibrated medicine cup.nHold the medicine cup at eye level.nRead the bottom of the meniscus.Wipe"drip" off top of bottle before replacing the cap -Liquid is to be administeredthrough a straw IFthe medication will potentially stain the patient's teeth or is especiallydifficult to take. -A syringe (with needle removed) maybe used to measure and administer a SMALL amount of liquid especially inPediatrics. Give into the side of themouth with head elevated. If spitting islikely, squeeze cheeks.ni.Donot hide a liquid medication in a beverage or food to ”trick” a patient intotaking |
|
|
What happens if a medication order is outside of the parameter of safe administration (outside the range of therapeutic dose)? |
Nurse has an obligation to contact the prescriber and clarify the order |
|
|
Rights of medication administration. Which are core rights? |
1.Rightpatient 2. Rightmedication 3. Right dosage 4. Right route 5. Right time 6. Right reason 7. Right Assessment 8. Right Documentation 9. RightResponse 10. Right to education 11. Rightto refuse (bold are the core ones) BOLD=core |
|
|
How large of a window do you have to give a medication at a scheduled time? |
One hours for most medications; 1/2 hour for antibiotics and insulin |
|
|
What are pregnancy categories for medication administration? |
From A (safe) to X (teratogenic) |
|
|
Criteria for choosing equipment for injections |
nRouteof administrationnViscosityof the solutionnQuantityto be administerednBodysizenTypeof medication |
|
|
What is involved with withdrawing medication accurately and with sterile technique? |
nDrawup correct amount of air in syringe.n Cleanse top of vial or pull cover off vial(clean with alcohol).n Inject air into the airspace of the vial.n Withdraw accurate amount of medication intosyringe.n Eject air bubbles.n Remove needle from vial. |
|
|
With IM injection, do you use larger or smaller needle? With subcutaneous, use smaller needle? |
Larger needle and larger lumen, smaller gauge Smaller needle and smaller lumen, larger gauge |
|
|
What must be used with ampules? |
Filter needle to withdraw, then replace with regular needle |
|
|
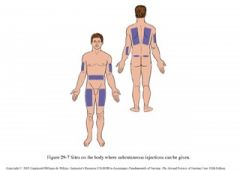
Subcutaneous sites |
Back of arm, stomach (2 inches away from umbilicus-- muffin top), subscapular, quad area |
|
|
Maximum amount of injection for subcutaneous injection? |
1 mL |
|
|
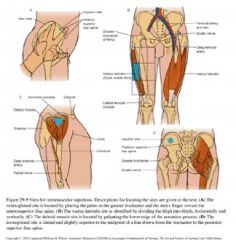
IM sites Who are different sites best used for? |
nVentroglutealsite (great for adults) nVastuslateralis site (great for children) nDeltoidmuscle sitenDorsoglutealsite – No longer recommended (because of deepness of muscle and sciatic nerve) |
|
|
Procedure for alcohol wipe for injections |
Clean area from center outward, place alcohol wipe next to area and let the alcohol dry |
|
|
How is skin held for injections? |
Stretch taut for IM or pinch for SC |
|
|
Correct angles for IM v. SC v. Intradermal |
IM: 90 degrees SC: 45 degrees with bevel up Intradermal: 5-15 degrees |
|
|
Why is aspiration performed once needle is stabilized during injection? |
To ensure that no blood is seen, if no blood is seen, we know we are in correct space If blood is seen, pull out needle, dispose, and start over |
|
|
How are medication patches disposed of? |
Sharps containers |
|
|
Steps for administering nasal sprays |
nSitpatient upright and tilt head back slightlynOccludeone nostril with fingernInserttip into open nostrilnAskpatient to inhale while squeezing atomizernRepeatas orderednAdministerin other nostrilnWashatomizer tipnWashhands |
|
|
Steps for instilling eye drops |
nWashHandsnGlovenOfferTissuesnCleanEye / Eyelids / EyelashesnTilthead backnHoldthe dropper close but DON’T touch eyenLetdrop(s) fall in as prescribed in the conjunctival sacnPresslightly on inner canthus to decreasesystemic effect Must wash hands, change gloves between eyes |
|
|
Respiratory drugs must be... Why? |
water soluble (or pneumonitis may occur) |
|
|
Steps in using metered dose inhalers |
nWashhands.nExplainsteps to patient:nAssembleunit, inspect mouthpiece (remove mouthpiece cover).nHavepatient exhale fully.nShakeunit to disperse medication.nPlacemouthpiece in front of mouth or in mouthnaccordingto manufacturer’s recommendations.nWhileinhaling slowly and deeply through mouth, depress medication canister fully.nHavepatient hold breath for 10 seconds or as long as possible or according tomanufacturer’s recommendations and exhale through pursed lips nWait5 minutes between puffs or as ordered by physician or according tomanufacturer’s recommendations.nUsesequential inhalers according to doctor’s orders. -Rinse mouth -Rinse mouthpiece and wash hands |
|
|
Pictoral of IM sites |
|
|
|
Steps for applying topical meds |
Applied to skin; there is decreased absorption on cornified (hardened) skin but increased on inner limbs and trunk; do not apply to open cuts, concentration of med more important than the amount applied, wear gloves |
|
|
Steps for applying patches/transdermal medications |
nCheckfor the presence of the old patch andremovebefore applying new patch. Cleanse skin.nCheckskin for any sign of irritation and promptlyreport.nApplynew patch to appropriate body sitesasrecommended by the manufacturer and rotatesites.nIfa patch requires date and time of application onthepatch, mark the patch before applying to theskin.nWashhands after application |
|
|
How are nose drops given? |
Place in supine position; push tip of nose up; position dropper above nostril directing tip toward midline of nose, count drops, keep head back for 5 minutes, clean and flush dropper |
|
|
How are eye ointments applied? |
Perform patient rights for medication administration, wash hands, wear glove, clean eye/eyelids/eyelashes, tilt head back, apply pressure downward to expose lower eye, apply prescribed amount along the conjunctival sac, close eyes gently |
|
|
Steps in administering ear drops |
Perform patient rights for med administration, wash hands, glove, position patient with affected ear up/toward you, clean any drainage, stabilize dropper hand to avoid ear canal drainage, for adult pull ear up and back, for child under three pull ear down and back before instilling drops; have patient remain for 5-10 minutes to allow medication to go into ear canal |
|
|
Rectal medications are often used for: What are the forms of rectal medications? What are important considerations for rectal medications? |
-Used for nausea, vomiting, unconsciousness, foul odor/taste, infants -Usually a suppository, may be a retention enema -Do not use an oral med for this route -Lubricant; insert past sphincter; if sphincter control is poor, hold buttocks closed after inserting -Be aware of possible vagal stimulation -Wear gloves |
|
|
How are vaginal medications given? |
Usually an applicator is used, keep patient supine Wear gloves |
|
|
Primary chronic disease of the elderly |
Arthritis and hypertension |
|
|
Chronic Illness Trajectory Model Stages of Corbin and Strauss |
8 stages: pre-trajectory, trajectory onset, crisis. acute, stable, downward, dying |
|
|
What is the shifting prospective model of chronic disease? |
Can have illness in the foreground on wellness in the foreground (with the other falling into the background) |
|
|
What is elder speak? |
Similar to baby talk, patronizing/conveys messages of dependence, incompetence control |
|
|
What are the biological, sociological, and psychological theories of aging? |
Bio: focus on physiological processes that occur in all organisms as they chronically age Socio: changes of roles and relationships Psychological: developmental aspects of aging |
|
|
What are the three most common Error (Stochastic) Theories of aging? |
-Wear and tear theory: cell errors are the result of wearing out, internal and external stressors -Cross-link theory: aging as accumulation of errors by cross-linking or stiffening -Free radical theory: most understood and accepted; random damage from molecules in cells called free radicals |
|
|
What are Programmed Aging Theories (Nonstochastic theories) of Aging? |
-Contribute the changes of aging to programming at the cellular level -Biological Clock: each cell is born with a limited number of replications |
|
|
What is the disengagement theory of aging? |
Sociological Theory Withdrawal from one's society and community is natural and acceptable |
|
|
What is the activity theory of aging? |
Sociological Theory -Individuals need to stay active if they are to age successfully -Promotes satisfaction and positive self concept -Physical or intellectual |
|
|
What is the continuity theory of aging? |
Sociological Theory With aging personality traits remain stable, as they age try to maintain previous habits, preferences, commitments, and beliefs |
|
|
Hazards of hospitalization for the elderly |
Decline in muscle strength, vasomotor instability, reduced bone density, diminished pulmonary ventilation, sensory deprivation, tendency to urinary incontinence |
|
|
Difference in delirium v. dementia |
Delirium is not dementia; delirium is preventable |
|
|
The greatest physiological changes with age are what type of changes? |
Sensorimotor changes |
|
|
Changes in body contour with age |
Bony prominences show, weight distributes to waist and hips, subcutaneous tissue leave the face and arms and move to abdomen/hips, height decreases |
|
|
What is sarcopenia? |
Loss of lean muscle mass; typical in aging |
|
|
How does weight change with aging? |
Unintentional weight loss is not a normal part of aging, there is a decrease in total body water content |
|
|
Differences in older adult's temperature regulation |
Less likely to have fever, more likely to have hypothermia, slower metabolism, produce less body heat, thermoregulatory impairment, sweat gland diminishes in size and function, reduced sensory input |
|
|
Median body temperature for older adult |
96.8 F (36 C) |
|
|
What is xerosis? |
Dry skin accompanied by pruritus |
|
|
What happens to the epidermis with age? |
Regeneration slows, reduced barrier protection |
|
|
What is the change in tactile perception with age and why does it occur? |
-Tactile sensation is decreased with age due to skin and sensory neuron changes -Difficult to determine if neuropathy is a natural aging process or an effect of disease -Possible delayed pain transmission (does not mean patient has reduced pain perception) |
|
|
Hair changes with age |
Loss of melanin Alopecia may occur |
|
|
Changes in nails with age |
Thicken, brittle/flat, vertical ridges (onchychorrhexis), oncholysis (fungus) |
|
|
Head and neck changes with age |
-Bones and orbits are more prevalent -Great vessels may have bruits -Neck shortens d/t osteoporotic changes: thyroid NOT usually palpable, there is loss of SQ tissue |
|
|
Physiologic changes in the eyes with age |
-Decreased eyelid elasticity -Conjunctiva become thinner and yellow with increased risk of infection -Lacrimal gland and ducts loose fatty tissue and tears decrease -Eyeballs sit deeper in sockets -Cornea flattens and iris fades -Increased connective tissue may cause sclerosis of sphincter muscles -Pupils becomes smaller, sclera becomes thick and rigid |
|
|
What is presbyopia? |
Decreased ability to adjust to near/far vision; common with increasing age |
|
|
Vision impairments often seen with aging |
Presbyopia: decreased ability to adjust near/far vision; decreased visual acuity (especially near vision) and narrowing of visual field; difficulty gazing upward and maintaining convergence, adapting to lighting changes |
|
|
Factors affecting hearing with age |
Cerumen buildup and hardening, corti and the auditory nerve atrophy, tympanic membrane thickening, tinnitus |
|
|
What changes in hearing occur with age? |
Decreased tone discrimination, presbycusis (difficulty hearing high frequency sounds), decreased ability to discern consonants, decreased equilibrium due to vestibular changes |
|
|
How does smell perception change with age? |
Decline after 60, rapid decline at 80 Cell loss in olfactory bulb and sensory cells Decrease in appetite and smell |
|
|
Teeth changes with age |
Teeth loose enamel and dentin: becomes more vulnerable to caries, incidence of periodontal disease increases |
|
|
Changes in taste perception with age with reasons for changes |
Very gradual decline; decreased taste--taste buds atrophy, amylase decreased in saliva, more noticeable with estrogen and protein deficiencies, accelerated with dental problems, medications, or smoking |
|
|
Changes in musculoskeletal structure with age |
Disks become thin and shortening, slight forward bent posture |
|
|
Changes in bones with age |
Decrease in bone density because resorption is more rapid than deposition |
|
|
Changes in joints, tendons, and ligaments with age |
Cartilage changes, tendons may shorten |
|
|
Changes in cardiovascular conductivity with age |
SA node firing isn't as fast, so heart rate decreases Atrial fibrillation can occur from fibrosis of SA node |
|
|
Changes in cardiovascular system with aging |
Elasticity of blood vessels decreased because of changes in collagen; vessel walls become thick and frayed |
|
|
What blood vessels are most likely to show changes with age? Why? |
BloodVessels of lower Extremities More likely to show s/s of cardiovascular Changesr/t dependent and distal position. |
|
|
Changes in respiratory system with age |
Depends on musculoskeletal and nervous system: Loss of elastic recoil, stiffening of chest wall, inefficiency in gas exchange, resistance flow, increased risk for infection because of less responsive cilia and diminished cough |
|
|
Changes in kidneys with age? What is the result? Changes in |
Loss of nephrons, decreased kidney mass, decreased GFR in linear fashion->medications stay in body longer |
|
|
Changes in ureters, bladder, and urethra with age |
Decreased tone and elasticity, decreased bladder holding capacity, urgency and frequency increases, nocturia |
|
|
Changes in thyroid gland with aging |
Increased incidence of hypothyroidism, decreased serum T3 from increased TSH, usually requires lower doses of thyroid replacement |
|
|
Changes in parathyroid gland with aging |
Changes in PTH may be cause of alterations in calcium homeostasis/bone loss |
|
|
Changes in endocrine pancreas with age |
Secretion does NOT decrease, tissues may develop decreased sensitivity to insulin |
|
|
Changes in esophagus with age |
Contractions increase, propulsion is decreased |
|
|
Changes in stomach with age |
Decrease motility, GERD r/t decrease in resting pressure of esophageal sphincter--INCREASED risk for aspiration; reduction secretion of bicarbonate and gastric mucous; decreased production of instrinsic factor, increased weight loss r/t anorexia |
|
|
Changes in neurotransmitters with age |
Decreased catecholamines, decreased serotonin, decreased choline acetylase, increased monoamine oxidase (MAO) |
|
|
Changes in female reproductive system with age |
Decreased estradiol, decreased estrone, breast size decreases, breast lumps more evident, menopause, cessation of menses, atrophy of ovaries |
|
|
Changes in male reproductive system with age |
Benign prostatic hypertrophy (BPH)-->dribbling/difficulty initiating urine stream May see an increase in fatty tissue of the breast-->self-breast exam increasingly important |
|
|
Cellular changes of the immune system with age |
Decrease in T-cell function, decrease in response to foreign antigen |
|
|
Changes in gait in each gender with age |
Male gait: smaller steps, wider base Female gait: waddling gait, bowing of legs |
|
|
Changes in sleep with age |
Interrupted REM episodes, increased total daily sleep, increased awakening after sleep onset-->wake up feeling tired |
|
|
Changes in intelligence with age |
Crystallized intelligence remains the same Fluid intelligence becomes more difficult-->requires more repetition |
|
|
Depression v. delirium v. dementia |
Depression: most often found, characterized by low mood, difficulty thinking, and somatic changes Delirium: an acute and sudden impairment of cognition that may be considered temporary Dementia: chronic, progressive, insidious, and permanent states of cognitive impairment |
|
|
Documentation should be done in what tense |
Document in 3rd person NOT 1st person |
|
|
Developmental issues with infant, toddler, preschooler, school age, and adolescent understanding of health and illness |
Infant: issues with attachment Toddler: disruption of routine/separation from parents Preschooler: loss of self-control, fear dark, injury (highest risk for regression) School age: loss of control/privacy Adolescent: understand causes of illness |
|
|
Aspects of assessing the pediatric client |
Doorway assessment: LOC, respiratory effort, color Primary assessment: ABCDE: airway and patency, breathing, circulation, disability presence, environment Secondary assessment: SAMPLE: s/s, allergies, medical history, past medical, last meal eaten, environmental influences to illness |
|
|
Order of infant and toddler vital sign |
1. Count respirations first (before disturbing the child) 2. Count apical HR second (in 4th intercostal) 3. Measure BP third 4. Measure temperature last (under 1 axillary, over 1-4 rectal or temporal) |
|
|
Placement of pediatric BP cuff |
Brachial artery, radial artery, popliteal artery, dorsalis pedis and posterior tibial artery |
|
|
Newborn axillary temp, pulse, respirations, BP |
36.8 C 80-180 pulse 30-80 respirations 73/55 BP |
|
|
What is the FLACC scale? |
Physical indicator of pain, used when faces scale cannot be answered, objective measure Facial expression, Legs (normal relaxed, tense, kicking, drawn up), Activity (quiet, squirming, arched, jerking), Cry (none, moaning, whimpering, scream, sob), Consolability (content, easy or difficult to console) |
|
|
What growth measurements are taken in pediatrics> |
-Recumbent length for infants up to age 36 months + weight and head circumference -Standing height and weigh after 37 months -Plot on growth chart: by gender and prematurity; <5th or >95th percentile considered outside expected parameters for height, weight, head circumgerence |
|
|
Physical growth in infants |
Double birth weight by age 6 months, triple birth weight by age 1 year |
|
|
Physical growth in toddlers |
Weight gain slows to 4-6 pounds a year, birth weight quadrupled by 2.5, height increases 3" per year |
|
|
Physical growth in preschoolers |
Physical growth slows and stabilizes, average weight gain remains about 5 lb/year, average height increases 2.5 to 3" per year |
|
|
Physical growth in school age children |
Height increases by 2 in per year, weight increases 2-3 kg per year |
|
|
Physical growth in adolescents |
20-25 % of total height achieved during puberty, usually occurs within 24-36 months |
|
|
When do anterior and posterior fontanel close? |
Anterior fontanel closes ~18 months Posterior fontanel closes between birth and 2 months |
|
|
Sinuses develop when? |
By about age 7 |
|
|
When do teeth begin to erupt? Dentist visit by what age? |
7 months, 1 year |
|
|
What is tonic neck (TNR) or fencing reflex? Problems with this? Is a precursor to: |
-Present at 1 month of age and disappears at around 4 months -When the child's head is turned to the side, the arm on that side will straighten and the opposite arm will bend -If the infant is unable to move out of this position or the reflex continues to be triggered past six months of age, the child may have a disorder of the upper motor neurons -Tonic neck reflex is a precursor to the hand-eye coordination of the infant. Prepares infant for voluntary reaching |
|
|
What is the Babinski reflex? |
-The sole of the foot is gently stroked. The big toe rises and the other toes fan out; disappears between 1-2 years A positive Babinski after that age is indicative of brain damage |
|
|
What is the Moro reflex? |
The startle reflex •Present at birth, peaks in the firstmonth of life and begins to disappear around 2 months of age. Occurs if theinfant's head suddenly shifts position, the temperature changes abruptly, orthey are startled by a sudden noise. •The legs and head extend while the armsjerk up and out with the palms up and thumbs flexed. Shortly afterward the armsare brought together and the hands clench into fists, and the infant criesloudly.•The reflex normally disappears by threeto four months of age |
|
|
Rooting reflex |
•Present at birth and disappears at around four months of age•A newborn infant will turn his headtoward anything that strokes his cheek or mouth, searching for the object bymoving his head in steadily decreasing arcs until the object is found. •Can usually only be elicited in a hungryinfant |
|
|
Palmer grasp reflex |
-Present at birth, persists until 5 or 6 months of age -When an object is placed in the infant's hand and strokes their palm, the fingers will close and they will grasp it |
|
|
Order of gross motor development |
Cephalocaudal direction of development; head control, rolling over ages 5-6 months, sit alone 7 months, crawling age 6 to 7 months, creeping age 9 months, move from prone to sitting position 10 months, walk with assistance 11 months, walk alone 12 months |
|
|
Order of fine motor development |
Grasping object 2-3 months, transfer object between hands 7 months, pincer grasp age 10 months, remove objects from container 11 months, build tower of two blocks 12 months |
|
|
Respiratory red flags for pediatrics include: |
Grunting and/or nasal flaring |
|
|
Apical pulse location in children |
4th intercostal under 7 years of age; 5th intercostal for 7 years of age and older |
|
|
Important aspects of cardiac assessment inpediatrics |
Up to 50% have innocent heart murmur, also normal to hear S3 r/t rapid ventricular filling, femoral pulses of greater importance--decrease or absence indicative of congenital heart defect |
|
|
When is sphincter control gained? |
2-3 years of age, older in boys |
|
|
How many wet diapers per day are expected in newborn? |
With every feeding, 6-8 per day as newborn |
|
|
Assessment readiness for toilet training |
•Voluntary sphincter control •Able to stay dry for 2 hours •Fine motor skills to remove clothing•Willingness to please parents•Curiosity about adult’s or sibling’stoilet habits•Impatient with wet or soiled diapers |
|
|
Sleep amounts for infants, toddler, preschoolers, school age, and adolescents |
Infants: sleep 16 hours Toddler: 12 hours at night with 2 daytime naps Preschoolers 9-16 hours at night, naps gone by age 5 School age: 8-10 hours Adoelscents: varies with growth spurts |
|
|
What are the deep tendon reflexes and what nerves do they test? |
Bicep reflex-C5, C6 Triceps reflex-C7 Brachioradialis reflex-C6 Patellar Reflex-L4 Achilles Tendon Reflex-S1 |
|
|
How are coordination and gait assessed? |
-Finger-nose-finger test -Rapid alternating movements -Precision finger tap -Heel shin test -Romberg test |