Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
12 Cards in this Set
- Front
- Back
|
1. List the four basic types of receptors as targets for drug action.
|
a. Ligand-gated ion channels (ionotropic receptors)
b. G-protein couples receptors (metabotropic) c. Kinase-linked receptors d. Nuclear receptors |
|
|
2. Describe the effect of drug-receptor interactions on receptor equilibrium.
|
- The drug-receptor interaction can either move equilibrium towards and increase or decrease in affinity. Agonists will favor the binding of a drug to a receptor and antagonist will reduce the affinity.
- At equilibrium, receptor occupancy is related to drug concentration. The higher the affinity of the drug for the receptor, the lower the concentration at which it produces a given level of occupancy, but not necessarily greater effect. - In the resting state (when there is not a ligand bound to the receptor) the equilibrium normally favors the resting state. - When a full agonist binds preferentially to the activated state, it shifts the equilibrium towards activation. An agonist initiates changes in cell function. Full agonists produce maximal effects, while partial agonists produce only submaximal effects - A partial agonist shows less selectivity and shifts the equilibrium to a smaller extent, even when receptors are fully occupied. - An antagonist shows no preference and does not shift the equilibrium, though it reduces the effect of an agonist by preventing the agonist from binding to the receptors. An antagonist binds to receptors without initiating changes in cell function. |
|
|
3. Describe the processes for coupling of drug, receptor, and second messenger systems and their pharmacologic response.
|
- The drug, receptor and second messenger help to enhance or inhibit a response
- A second messenger system is a method of cellular signaling where the signaling molecule does not enter the cell, but rather utilizes a cascade of events that transduces the signal into a cellular change. Second messenger systems utilize receptors on the surface of the plasma membrane which are generally coupled to a kinase on the interior surface of the membrane. The kinase then phosphorylates another molecule (frequently cAMP) which carries out a further action. |
|
|
4. Describe the rationale for the use of log dose-response (LDR) curves in pharmacology
|
The greater the dose of action ( increasing concentrations of the agonist) = the greater the response)
- The LDR curves enable: 1. estimation and comparison of maximal effect (efficacy) of agonists 2. estimation and comparison of potency of agonists 3. identification and comparison of full and partial agonists 4. interference about similar and different mechanism of drug action |
|
|
5. Define ED50, EC50, and Emax and give examples employing LDR curves
|
ED50 - The dose of a drug that is pharmacologically effective for 50% of the population exposed to the drug or a 50% response in a biological system that is exposed to the drug.
EC50 - The effective concentration of an agonist, which produces 50% of the maximum possible response for that agonist. Emax - The maximum observed effect in a concentration-response or time-response experiment. |
|
|
6. Relate ED50, EC50 and Emax to the concepts of intrinsic activity, efficacy and potency of a drug employing LDR curves.
|
Emax is the maximum effect (efficacy) of the drug; where efficacy is defined as the ability, once bound to the receptor, to initiate changes that lead to effects. Potency is a measure of the concentrations of a drug at which it is effective. The EC50 and ED50 are the concentration and dose, respectively, at which the drug has its most potent effect for either inhibition or effectiveness.
|
|
|
7. Describe the pharmacologic basis of characteristic LDR curves for full agonists and neutral (pure) antagonists.
|
These dose-effect curves can determine:
- pharmacokinetic antagonism – where one drug affects the absorption, metabolism, or excretion of the other drug. - competitive antagonism - where both drugs bind to the same receptors - non-competitive antagonism – the antagonist interrupts receptor-effector linkages - physiological antagonism – two drugs producing opposing physiological effects - chemical antagonism – interaction in solution |
|
|
8. Be able to estimate, compare, and contrast the potency and efficacy of drugs employing LDR curves.
|
**Review graphs on power point slides.
|
|
|
9. Define partial agonists with respect to full agonists and neutral antagonists.
|
A partial agonist is an agonist which, no matter how high a concentration is applied, is unable to produce maximal activation of the receptors.
Full agonists have a high efficacy and can produce their maximal response while occupying a relatively low proportion of receptors; partial agonists have a lower efficacy and cannot activate the receptors to the same degree and may not be able to produce the same maximal response even when they occupy the entire receptor population. An antagonist is a drug which attenuates the effect of an agonist. It binds to a region of the receptor in common with an agonist, but occupies the site without activating the effector mechanism. Therefore, an antagonist could make the partial agonist’s efficacy even lower. |
|
|
10. Define the utility of partial agonists in clinical practice.
|
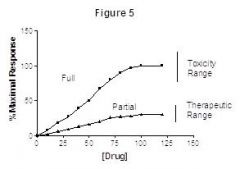
Partial agonists are used in clinical practice because the safe dose range can be greatly extended (the maximum response only reaches the sub-l00% efficacy value and stays there as a plateau). If you give the full agonist this could potentially become toxic to the patient, whereas the partial agonist will not. Partial agonists are able to increase receptor function without necessarily causing a 100% efficacy. See figure 5 below:
|
|
|
12. Relate the shape of LDR curves of drugs to their clinical actions
|
The slopes of the curves measure the affinity of the agonist or antagonist for the receptor. The steeper the slope the less of a dose it takes for the drug to have an effect on the receptors. (Slide 33). Also when two curves are parallel, it suggests that the two drugs act through the same receptor. If two drugs have non-parallel curves, they probably have different sites of action.
|
|
|
13. Illustrate and interpret the effects of reversible competitive and irreversible competitive antagonists on LDR curves
|
- Reversible competitive antagonism is the commonest and most important type of antagonism. It has two main characteristics:
1) in the presence of the antagonist, the agonist log concentration-effect curve is shifted to the right without change in slope or maximum, the extent of the shift being a measure of the dose ration 2) the dose ratio increases linearly with antagonist concentration; the slope of this line is a measure of the affinity of the antagonist for the receptor. - With the irreversible competitive antagonists, no amount of agonist can completely overcome the inhibition once it has been established. So, as you add more antagonist, the potency of the agonist decreases. The reaction between the antagonist and the receptor is NOT reversible, so with large amounts of antagonist, the agonist looses the competition and does not bind to or have a significant effect on the receptors. |