Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
48 Cards in this Set
- Front
- Back

|
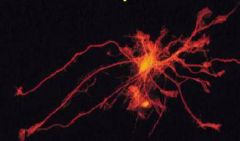
Neuron
|
|

|
Neuron
|
|
|
What are the domains of a neuron?
|
Soma (cell body)
Dendrites (input) Axon (output) |
|
|
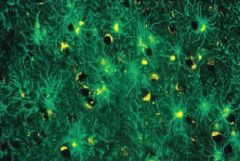
Astrocytes
|
|
|
Astrocytes
|
|
|
Describe astrocytes
|
-Major glial cell of the brain
-Stellate or star shaped -Attached to a number of other elements in the brain -Astrocyte processes overlay blood vessels in brain -Attach to pial surface of brain -Enfold synapses -Instruct epithelial cells to make tight junctions for BBB -Have transporters for many neurotransmitters -Control neurotransmitter and potassium levels in brain -Promote growth and facilitate synaptic conduction |
|
|
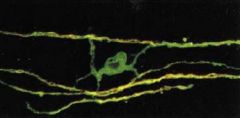
Describe oligodendrocytes
|
-Myelinating cells of the CNS
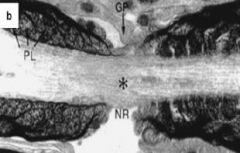
-One oligodendrocyte wraps many neurons -Nodes of Ranvier in neurons are areas between myelin with lots of Na channels -Oligodendrocytes and/or myelin are destroyed in many pathological processes |
|
|
Oligodendrocyte
|
|
|
Node of Ranvier
|
|
|
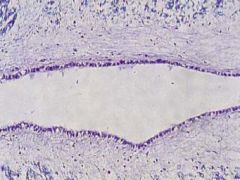
Describe ependymal cells
|
-Line the ventricular walls
-Ciliated single columnar or cuboidal epithelium -Cilia moves CSF -CSF is made by choroid plexus, it fills ventricles and bathes brain - |
|
|
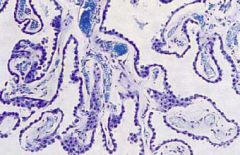
Describe the choroid plexus
|
-Produces CSF
-Where brain interfaces with mesenchymal elements -Has a core of fibrous tissue and blood vessels -Lined with choroid plexus epithelium that is contiguous with ependymal cells -CSF is an ultrafiltrate of plasma filtered by the choroid plexus |
|
|
Ependymal cells
|
|
|
Choroid plexus
|
|
|
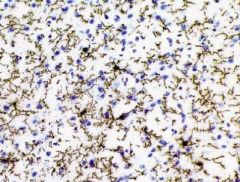
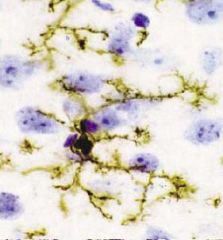
Describe microglia
|
-Hematopoetically derived
-Enter brain during embryonic life and stay there forever -From monocyte lineage -Cover most of the volume of the brain -APCs -Have phagocytic activity |
|
|
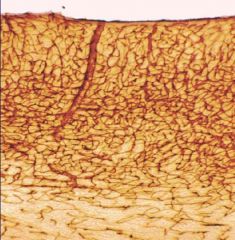
Describe the distribution of blood vessels in the brain
|
-Brain is highly vascularized
-Blood vessels come up over the surface of the brain and enter radially -Cortex (gray matter) has many more vessels than white matter |
|
|
How many choroid plexuses are there?
|
4
One in each lateral ventricle and 2 in the 4th ventricle |
|
|
What connects the 3rd and 4th ventricles?
|
Aqueduct of Silvius
|
|
|
What is the roof of the 4th ventricle? The base?
|
Roof: Cerebellum
Base: Brain stem |
|
|
What connects the 4th ventricle and the subarachnoid space?
|
Foramina
|
|
|
Where is CSF resorbed? How often is CSF resorbed?
|
Arachnoid granulations
Several times a day |
|
|
How much CSF is in the average adult?
|
150ml
|
|
|
Microglia
|
|
|
Microglia
|
|
|
Blood vessels in the brain
The cortex has more than the white matter |
|
|
What is hydrocephalus? What causes it?
|
An enlargement of one of more of the ventricles
It can be caused by: -An overproduction of CSF (rare) -A block of CSF through the ventricles -A block of CSF resorption |
|
|
When does overproduction of CSF occur?
|
With choroid plexus papillomas
|
|
|
What is an obstructive/non-communicating hydrocephalus?
|
Hydrocephalus caused by a block of CSF flow through ventricles.
This occurs with aqueductal stenosis, masses in the ventricle system and foramina, and with malformations (Arnold Chiari) |
|
|
What is a communicating hydrocephalus?
|
A hydrocephalus caused by a block in the resorption of CSF
This can be caused by meningitis, subarachnoid hemorrhage, or dural sinus thrombosis |
|
|
What is the relationship between intracranial pressure and brain volume?
|
-Volume inside skull is fixed
-With intracranial hemorrhage, blood leaks into brain -There are some thing in the brain, CSF in ventricles and subarachnoid space, that can be squeezed out -Eventually there is nothing left to squeeze -After that pressure increases dramatically |
|
|
Describe the BBB
|
-Endothelial cells form tight junctions
-Outside endothelial cells is basement membrane -Then there are foot processes of astrocytes -BBB restricts cells and macromolecules from the blood directly entering the brain |
|
|
What is often responsible for rapid expansion of the brain?
|
Edema
|
|
|
What is edema?
|
Increase in volume and weight due to accumulation of fluid.
Edema can accompany rapid or slow expansion of the brain. The rapid expansions are much more problematic. |
|
|
What is vasogenic edema?
|
-Edema due to increased cerebrovascular permeability.
-This occurs when the BBB is damaged and opens up. -It allows serum for the capillary systems to enter the brain. -Fluid can produce an increase in intracranial pressure -Duration of BBB incompetence varies with the type of pathology |
|
|
What does the progression and extent of vasogenic edema depend on?
|
1. Level of systolic blood pressure (when intracranial pressure equals systolic BP, no more fluid will enter brain)
2. Duration of BBB incompetance |
|
|
What can cause vasogenic edema?
|
(BBB breakdown)
Trauma Infarction Hemorrhage Neoplasms Infections Inflammation Tumors and metastatic cancers tend not to have BBB anymore. The blood vessels that feed most metastatic cancers don’t maintain a BBB. The blood vessels that feed malignant gliomas don’t maintain a BBB. |
|
|
Describe brain herniations
|
-Rapidy growing hemorrhage or tumor would increase pressure in one area and push brain in opposite direction
-Brain can move under free edges of dural folds -Cingulate gyrus can be pressed under the corpus callosum under the free edge of the falx cerebri -Uncus can be pushed over free edge of tentorium -Cerebellum can be pressed into the foramen magnum |
|
|
What is the big issue with brain herniations?
|
It is not the area doing the pushing, it is the area being pressed against
|
|
|
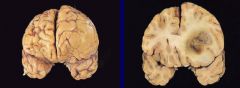
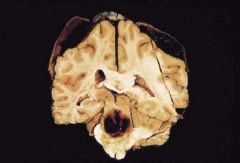
Patient with metastatic carcinoma - mass lesion/cerebral edema
Subfalcine herniation. Normal gyri and sulci are effaced. |
|

|
Intracerebral hemorrhage
Probably on the basis of hypertension. Hypertensive hemorrhages usually come in under arterial pressure because the arterioles break. This produces a pressure gradient and forced the brain in a particular direction. |
|
|
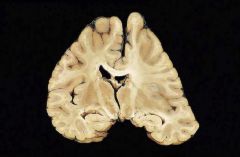
Herniations from subdural hematoma
You see the flattening side of the brain due to eh subdural hematoma. There is a shift tin the ventricles. This is easy to pick up on a CT or MRI. |
|
|
What occurs with uncal herniation at the midbrain level?
|
1. CNIII- pupil dilation on side of herniation
2. PCA/SCA - visual cortex/occipital lobe infarction 3. Cerebral peduncles compression -ipsi (if contralateral peduncle is compressed) or contralateral hemiparesis (if ispilateral peduncle is compressed) 4. AP compression - aqueductal compression hydrocephalus |
|
|
Uncal herniation
|
|

|
Medial occipital infarction (visual cortex) from PCA compression from uncal herniation
|
|
|
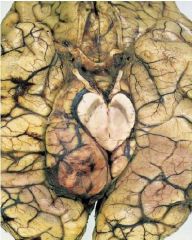
What is a duret hemorrhage? How do they occur?
|
Bleeding in the midbrain and pons
As the pressure and herniation start to now move down further it not only compresses the midbrain but also starts to compress the pons and medulla. It can force the pons and medulla caudally. The blood vessels that serve it come from the circle of Willis and are tehtered at the circle of Willis. If you put a lot of pressure down on those vessels they bleed and produce hemorrhages within the brain stem. These are fatal. |
|

|
Duret hemorrhage
|
|
|
Duret hemorrhage
|
|

|
Cerebellar tonsillary herniation
Compression of the medulla. What happens here is that the medulla gets compressed. The medulla is where your respiratory and cardiovascular synchronicity and automatic centers are. Patients who get this far end up with abnormalities in breathing and heart rate. This is fatal as well. |
|
|
What are the sequelae of rapidly expanding supratentorial lesions?
|
1. Uncal, hippocampal herniation
2. Compression of ipsilateral CN III 3. A-P compression of midbrain 4. Obstructive hydrocephalus 5. Cerebral peduncle compression (ipsi- or contralateral hemiparesis) 6. PCA compression (ischemica of visual cortex and thalamus) 7. Duret hemorrhages (central stem) 8. Tonsillar herniation - compression of medulla |