Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
51 Cards in this Set
- Front
- Back
|
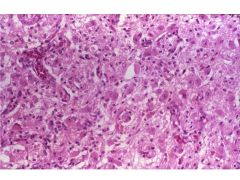
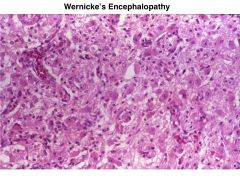
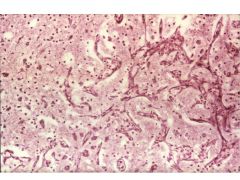
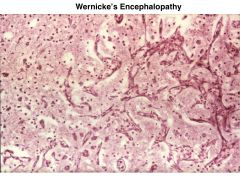
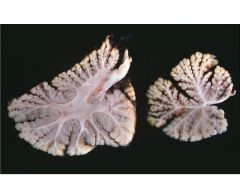
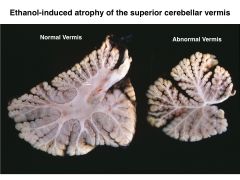
Wernicke's encephalopathy:
6 |
-Thiamine deficiency
-Lesions that appear hemorrhagic, but are actually proliferation of small vessels. -These are dispersed throughout the MBs and hypothalamus. -Involvement of the DM thalamus leads to confabulation; condition gets called WKS at this point. -Neuronal loss and gliosis of affected areas is also present. -Atrophy of cerebellum |
|
|
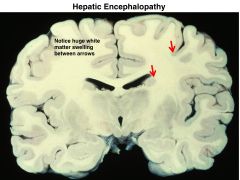
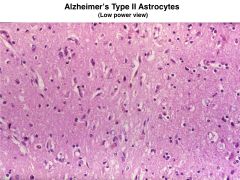
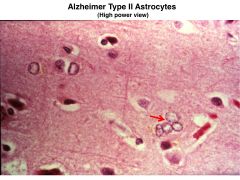
Hepatic Encephalopathy:
|
-Damage to the brain resulting from hepatic encephalopathy occurs because of elevated ammonia levels that impair oxidative metabolism.
-The brain shows diffuse edema, as well as proliferation of so-called ALZHEIMER TYPE II ASTROCYTES. These cells are characterized by a central clearing of their nucleus and a red, spotty nucleolus. *common with etoh abuse, but can be caused by other things. |
|
|
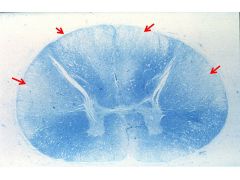
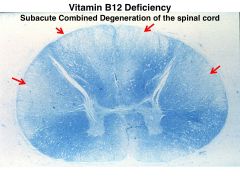
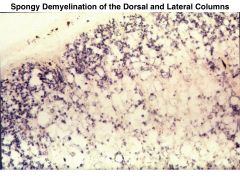
Vit B12 deficiency:
|
-Nutritional deficiency of cobalamin leads to degeneration of axons and demyelination of the
DORSOLATERAL regions of the spinal cord. -Characteristically spares the anterior columns. |
|
|
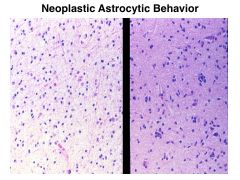
-histologically malignant
-biologically malignant |
(1) histologically malignant: dysplastic and/or anaplastic biopsy features.
(2) biologically malignant – benign tumors that are not resectable but because of mass effects could be fatal. |
|
|
1˚ intracranial tumors:
1˚ brain tumors: |
Primary intracranial tumors: primary tumors in the cranial cavity
Primary brain tumors: arise from constituents cells of brain not including non-brain intracranial tissue (i.e. meningiomas) and metastatic tumors |
|
|
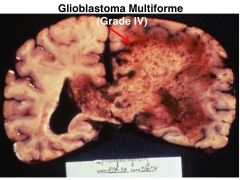
Astrocytoma and Glioblastoma Multiforme:
prevalance age at presentation |
80% of adult primary brain tumors
most common in late middle age divisible into 4 grades |
|
|
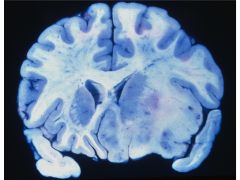
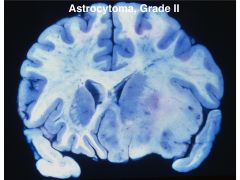
Describe Astrocytoma Grade II: 4
|
-poorly defined; hard to see where it starts/ends.
-infiltrative; µscopic spread very common, aggressive. -uniform population of cells containing a variety of astrocytic conformation (protoplasmic, fibrillary or gemistocytic) -marked tendency to become more anaplastic with time |
|
|
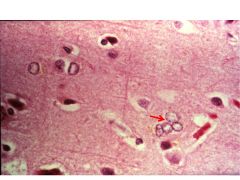
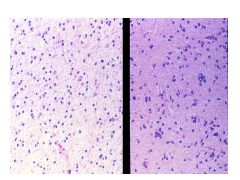
Satellitosis:
|
Astrocytomas show a subtle increase in the number of astrocytes. These tend to surround
neurons – a finding called SATELLITOSIS. The proliferative astrocytes tend to crowd one another and show loss of contact inhibition. |
|
|
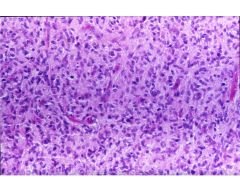
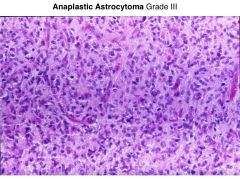
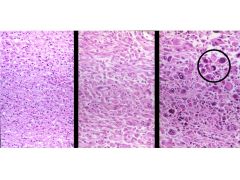
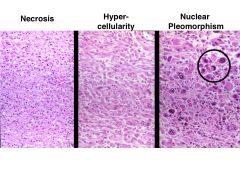
Anaplastic astrocytomas:
|
Show increases in pleomorphism and mitotic figures as well as a generalized hypercellular appearance.
|
|
|
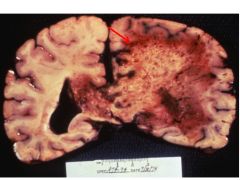
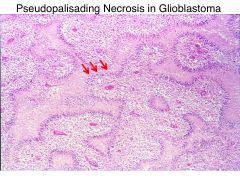
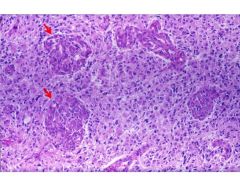
Glioblastoma:
|
Like an anaplastic astrocytoma with necrosis.
|
|
|
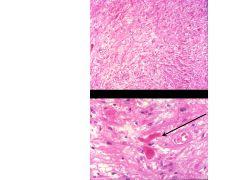
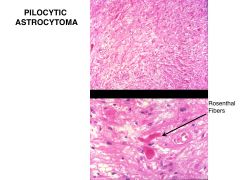
Pilocytic Astrocytoma:
histologic traits 4 behavior prognosis |
-often cystic
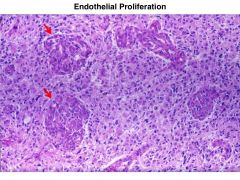
-protoplasmic astrocytes (bipolar cells with “hair-like” processes -Rosenthal fibers (eosinophilic bodies formed in astrocyte processes) -vascular endothelial proliferation- does not imply unfavorable prognosis -slow growing; act like hamartomas -prognosis pretty good. |
|
|
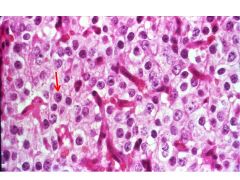
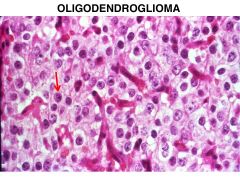
oligodendoglioma:
prevalance age at presentation locations in brain histologic traits 4 prognosis |
-5% of all gliomas
-middle age -cerebral hemispheres -well circumscribed -focally hemorrhagic -calcification -microscopic: sheets of cells with spherical nuclei surrounded by halo of cytoplasm -up to 50% contain areas of astrocytoma that determines prognosis -Can progress into a glioblastoma (same progenitor cells) and kill you |
|
|
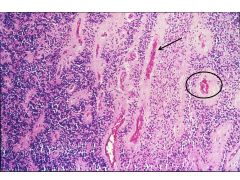
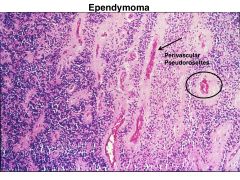
ependymomas
prevalance age at presentation locations in CNS histologic traits prognosis |
-typically fourth ventricle; usually present with hydrocephalus
-5-10% of primary brain tumors in first two decades of life -in middle age spinal cord is most common location -large percentage of primary intraspinal neoplasms of middle age -typically solid or papillary masses projecting from floor of ventricle -intraspinal tumors are sharply demarcated making total resection possible; not responsive to chemo/rad. |
|
|
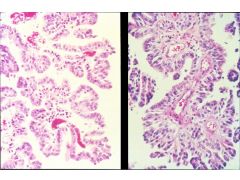
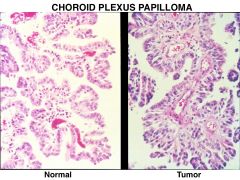
Choroid plexus papilloma:
|
most common in lateral ventricles of children
in adults frequently found in the fourth ventricle microscopic: recapitulate normal choroid plexus with marked papillary growth |
|
|
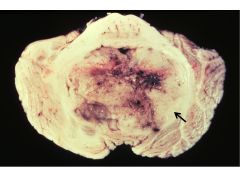
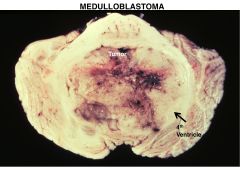
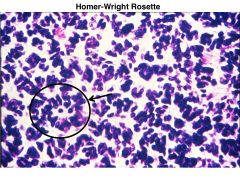
Medulloblastoma:
prevalance age at presentation locations in CNS histologic traits behavior prognosis |
-cerebellum
-first few decades of life -25% of all primary brain tumors in this age group -typically in vermis of cerebellum -frequently disseminate through the CSF -microscopic: densely cellular pleomorphic nuclei with little cytoplasm Homer Wright rosettes -capacity for both glial and neuronal differentiation -origin may be external granular layer of cerebellum -10 year 50% survival with surgery and radiotherapy |
|
|
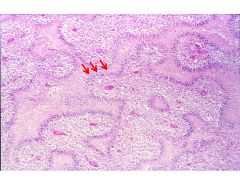
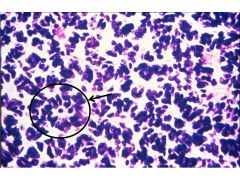
Pseudorosettes:
True rosettes: |
When cancer cells seem to cluster around a central vessel; often seen in EPENDYMOMA.
-AKA HOMER-WRIGHT rosettes; often seen in Medulloblastoma and Neuroblastoma; differentiated tumor cells surround the neuropil. |
|
|
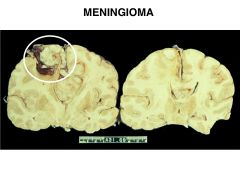
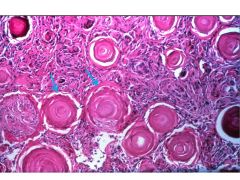
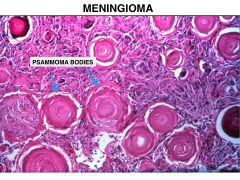
meningioma:
prevalance age at presentation locations in CNS 4 histologic traits behavior prognosis |
-arise from arachnoid cap cells
-20% of all primary intracranial tumors -locations: convexities falx cerebri lesser wing of sphenoid olfactory groove -middle and older aged -3:2 ratio of women to men -rapid growth during pregnancy -sex hormone receptors -Have a dural tail; distinguishes from a met. |
|
|
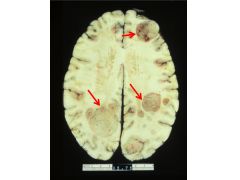
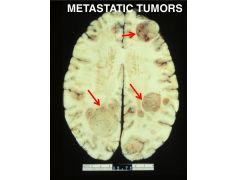
Metastatic Tumors:
prevalance origin 5 type of cancer they arise from histologic traits behavior prognosis |
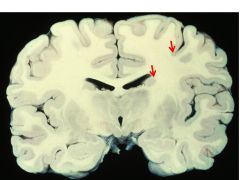
-25-30% of intracranial tumors
-majority are carcinomas lung breast skin (melanoma) kidney gastrointestinal -choriocarcinoma- rare, but frequently metastasizes to brain -gray-white junction, sharply demarcated -surrounding zone of edema -microscopic recapitulates primary (look the same) -surgery |
|
|
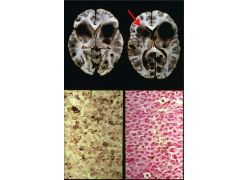
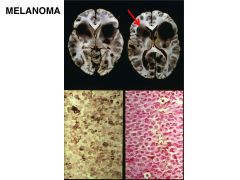
Metastatic neoplasms involving CNS:
-location in brain -what locations are rarely involved? -posterior fossa mets common from what cancers? -what blood distribution is commonly involved? -when is hemorrhage prominent? |
-take origin in well vascularized gray matter
-8:1 ratio of cerebrum to cerebellum -brainstem rarely involved -posterior fossa metastasis frequently from GI tract, bladder and uterus (via Batson's plexus) -brain supplied by middle cerebral artery preferentially involved (due to sheer volume) -hemorrhage is especially prominent in melanoma and choriocarcinoma |
|
|
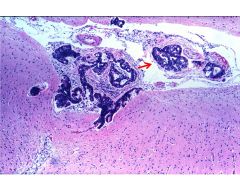
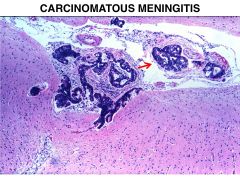
carcinomatous meningitis:
|
-Another disturbing feature of metastatic tumors is their ability to invade the CSF.
-If given access to the ventricular system, these tumors can irritate the meninges, producing CARCINOMATOUS MENINGITIS. |
|

|

|
|

|

|
|
|
|
|
|
|
|
|
|
|
|

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

|
|
|
|
|
|
|
|
|
|
|
|

|
|
|
|
|

|
|
|
|
|
|
|
|
|
|
|
|
|
|