Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back
|
Describe Bacterial Meningitis
|
-Most common form of CNS infection
-Reliable to make diagnosis clinically -Symptoms are fever, headache, stiff neck, photophobia -Bacteria get to brain through blood or direct extension of places like sinuses or inner ear -Associated with acute inflammatory infiltrate, neutrophils -CSF low in sugar, high in protein, cloudy, many neutrophils -Primarily infects <5yo (70%) and >70yo (20%) |
|
|
Describe Viral meningitis
|
-Primarily lymphocytic infiltrate
|
|
|
What is the primary cause of bacterial meningitis in neonates?
|
-Group B streptococcus
-(E. coli) |
|
|
What is the primary cause of bacterial meningitis in infants/children?
|
-H. influenzae
|
|
|
What is the primary cause of bacterial meningitis in adolescents and young adults?
|
-Neisseria meningitidis
|
|
|
What is the primary cause of bacterial meningitis in the elderly?
|
-Streptococcus pneumoniae
|
|
|
Describe brain abscesses
|
-Second most common infection of the CNS following bacterial meningitis
-Bacteria get into the substance of the brain -Bacteria get in through blood or direct extension -Lesions go from focal abscess to encapsulated lesion -Early cerebritis (1-3 days)- Inflamed lesion with neutrophils -Late cerebritis (4-9 days) -Early capsule formation (10-13 days) -Late capsule formation (14+ days) |
|

|
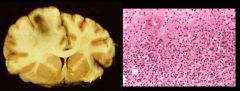
Bacterial meningitis - Treatable
Green discoloration is pus on the leptomeninges |
|
|
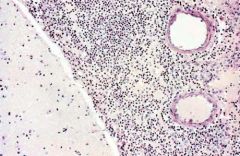
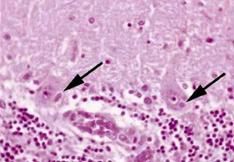
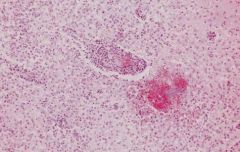
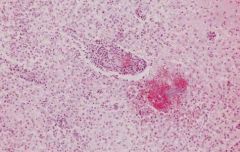
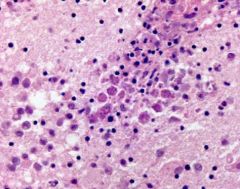
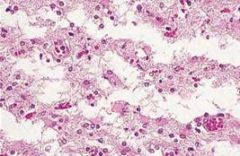
Bacterial meningitis
You can tell it is the meninges from the large vessels. The meninges is abnormally cellular and the black dots are all neutrophils |
|

|
Ring enhancing lesion on CT
The enhancement is where you have new vessels without BBB Dye leaks out of these vessels when given contrast |
|
|
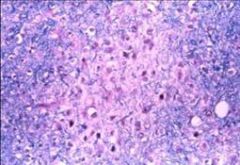
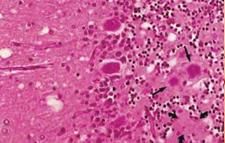
Early cerebritis
Grossly there is a hemorrhagic lesion at the grey-white junction. Brain is inflamed and soft. Microscopically there are many neutrophils and dying cells |
|
|
Late cerebritis
Macrophages have come to clean up the debris. There is inflammatory infiltrate with monocytes and macrophages. |
|
|
Early Capsule Formation
This involves proliferation of endothelial cells and the perivascular cells. There starts to be collagen deposits. |
|

|
Late capsule formation
As capsule evolves it becomes a well formed dense collagenous capsule. This is an abnormal response. Normally the brain responds to injury with a gliotic capsule. |
|

|
Fibrotic capsule
Capsule is so dense that surgeons can remove it pretty easily |
|
|
Describe cerebral fungal infections
|
-Often seen as an opportunistic infection in immunocompromised patients
-Typically reaches CNS through blood -May produce meningitis, vasculitis, granulomas, or cerebral abscess |
|
|
What are the common fungal CNS infections?
|
-Aspergillus (septate hyphae)
-Mucomycosis (Nonseptate hyphae) -Candida (Budding yeast, pseudohyphae) -Cryptococcus (Budding yeast, encapsulated) |
|
|
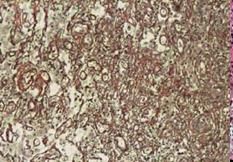
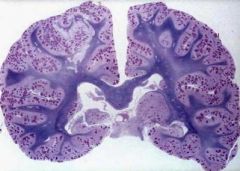
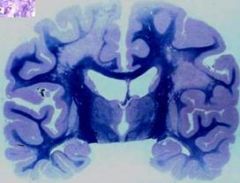
Candida albicans
Tissue has been stained for LFB (stains for myelin) and PAS (for candida). This girl has 1000s of microabscesses. Often candida is more focal and limited. Each spot is a microabscess. |
|
|
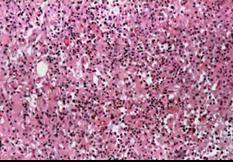
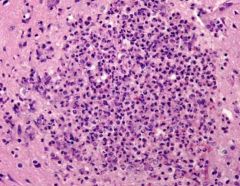
Candida albicans
This is on high magnification. These are neutrophils. This could be a bacterial or fungal abscess. |
|

|
Candida albicans
|
|
|
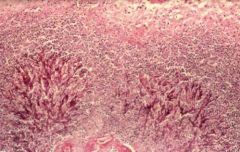
Aspergillus
These abscesses tend to be more hemorrhagic and necrotic |
|
|
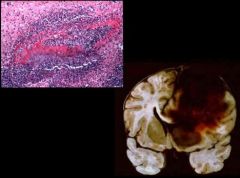
Aspergillus
Tends to invade blood vessels. It destroys the vessels and causes hemorrhage |
|
|
What are the manifestations of CNS viral infections?
|
-Aseptic meningitis
-Encephalitis -Meningoencephalitis -Myelitis |
|
|
Describe CNS viral infections
|
-Viruses have tropism for certain cell types
-Tend to see lymphocytic infiltrates surrounding blood vessels -Microgliosis also occurs -Microglial cells react to viruses by activating, becoming plump, and forming nodules. -Reactive astrocytosis (most common, non-specific reaction to injury. Astrocytes form intracellular inclusions) |
|
|
What are the stereotypical tissue reactions to viral infections?
|
-Inflammatory cell infiltrates
-Microgliosis -Neuronophagia -Microglial nodules -Astrocytosis -Intracellular inclusion bodies -Neuronal cell degeneration -Cellular and tissue necrosis |
|
|
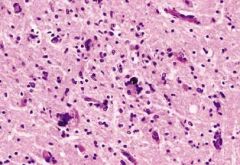
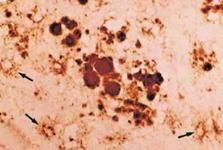
-Negri bodies
-Intracellular inclusions from rabies |
|
|
-Negri bodies
-Intracellular inclusions from rabies |
|
|
-Negri bodies
-Intracellular inclusions from rabies |
|
|
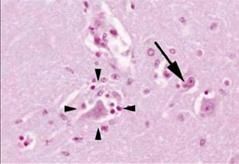
Describe Rabies
|
-Viral infection
-Transmitted by animal bite -There is a dormant stage and then you develop a CNS syndrome -Histologically there are intracellular cytoplasmic inclusions called Negri bodies in Purkinje cells in cerebellum and Pyramidal cells in the hippocampus -Relatively little inflammatory infiltrate - |
|
|
Describe Herpes virus
|
-Neurotropic
-Tendency to infect neurons in the temporal lobe |
|

|
Herpes simplex encephalitis
|
|
|
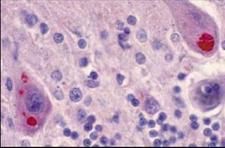
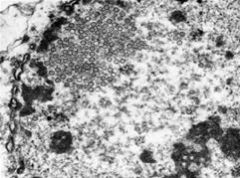
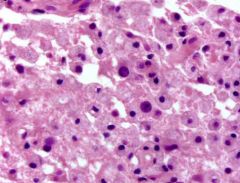
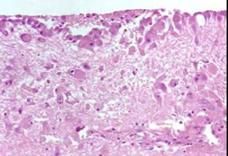
-Herpes simplex virus encephalitis
-Internuclear inclusions called Cowdry bodies -There is a nucleus with a big clearing and a little eosinophilic to basophilic amphomorphic inclusion in the middle of the nucleus -This is accumulation of the herpes virus |
|
|
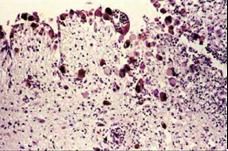
-Herpes simplex virus encephalitis
-Internuclear inclusions called Cowdry bodies -There is a nucleus with a big clearing and a little eosinophilic to basophilic amphomorphic inclusion in the middle of the nucleus -This is accumulation of the herpes virus |
|

|
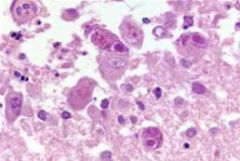
-Herpes simplex virus encephalitis
-Internuclear inclusions called Cowdry bodies -There is a nucleus with a big clearing and a little eosinophilic to basophilic amphomorphic inclusion in the middle of the nucleus -This is accumulation of the herpes virus |
|
|
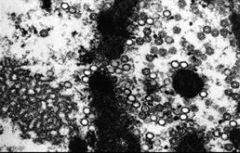
-Herpes simplex virus encephalitis
-There is perivascular lymphocytic infiltrate -You get macrophages and microglial nodules -Lots of macrophages, roaring inflamation and hemorrhage -Typical of end stage herpes encephalitis |
|
|
What are the primary complications of AIDS?
|
-HIV encephalitis or AIDS dementia complex
-HIV associated myelopathy (vacuolar myelopathy) -HIV-associated neuropathy (distal sensory neuropathy) -HIV associated myopathy |
|
|
What are the secondary complications of AIDS?
|
-Opportunistic infections
-Cryptococcosis -Toxoplasmosis -Progressive multifocal leukoencephalopathy -CMV -Primary CNS lymphoma |
|
|
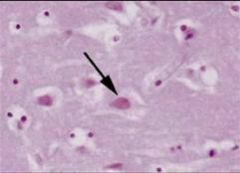
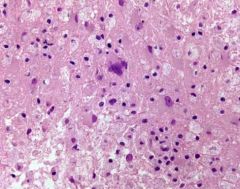
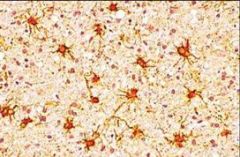
-HIV encephalopathy
-Microglial nodule with multinucleated giant cell - pathognomonic feature -HIV does not have a predilection for neurons |
|
|
How does HIV affect the brain?
|
-One idea is that microglial/macrophages and multinucleated giant cells can secrete things that are bad for neurons
-The viral particles themselves are bad for neurons |
|

|
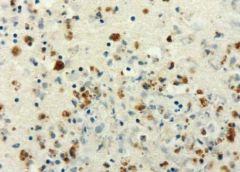
-Toxoplasmosis gondii
-Seen in immunocompromised patients -Show ring enhancing lesions -Lesions have necrotic centers with reaction around the edge |
|
|
-Toxoplasmosis gondii
-Biopsies contain lots of necrosis -Large organisms that form cysts (bradyzoite) -Break out to tachyzoite stage in immunocompromised individuals |
|
|
-Immunohistologic staining for toxoplasmosis gondii
|
|
|
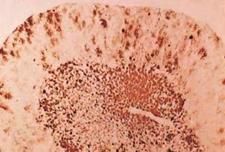
-Progressive multifocal leukoencephalopathy
|
|
|
Progressive multifocal leukoencephalopathy
|
|
|
Describe progressive multifocal leukoencephalopathy
|
-Caused by JC virus, a papavovirus
-Tropism for glial cells -Infects oligodendrocytes causing demyelination -Infects astrocytes -Radiographically and grossly you see small and growing demyelinating lesions -They start small and multifocal and grow to confluence |
|
|
-Progressive multifocal leukoencephalopathy
-Can see inclusions in glial cells -There are macrophages eating the myelin -Oligodendrocytes appear abnormal. They develop large, glassy, jelly-bean like appearance. -Nucleus is loaded with JC virus |
|
|
-Progessive multifocal leukoencephalopathy
-Can infect astrocytes and they become bizarre looking |
|
|
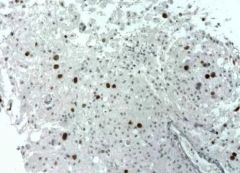
-Immunohistologic staining of JC virus
-Targets T antigen of SV40 virus (similar virus) -Nuclei stain strongly possitive |
|
|
-Cytomegalovirus encephalitis
|
|
|
Describe cytomegalovirus
|
-Most common opportunistic infection in HIV patients
-Relative of herpes virus -Gives Cowdry type inclusions -Gliotropic virus -Makes bizarre looking cells -Infects astrocytes and ependymal cells -Common gross finding is ependymitis -Can see giant cells with inclusions in the nucleus with some in the cytoplasm |
|
|
Cytomegalovirus encephalitis
|
|
|
Cytomegalovirus encephalitis
|
|
|
-Cytomegalovirus encephalitis
-Shows internuclear inclusions and giant cells -Clinical information is necessary for diagnosis (could be a weird metastatic tumor or something) |
|
|
-Cytomegalovirus encephalitis
-Shows internuclear inclusions and giant cells -Clinical information is necessary for diagnosis (could be a weird metastatic tumor or something) |
|
|
Describe transmissible spongiform encephalopathies
|
-Prion disease
-Worldwide incidence 1:1,000,000 -Peak incidence in 7th decade of live -Sporadic: 85% -Familial: 15% -Iastrogenic transmission: very rare -Rapid progressive dementia, myoclonus, ataxia, usually fatal in less than a year -As the disease progresses neurons die and it can get to the point where all you see are astrocytes and holes |
|
|
Describe the prion hypothesis
|
-Not inactivated like DNA, RNA or by formalin fixing or heat
-Protein can take 2 conformations: 1 that is soluble with many alpha helices, the other is insoluble and has many beta pleated sheets -Protein can transform between these 2 conformations -If a cell gets infected with the beta pleated sheet form it will induce the other proteins to switch conformation |
|
|
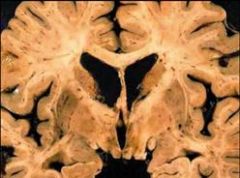
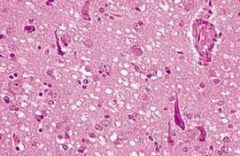
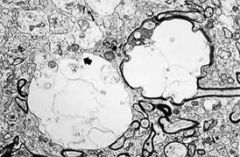
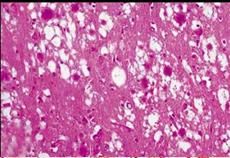
-Transmissible spongiform viral encephalopathy
-See lots of little holes in the brain -Holes can be focal or diffuse -Tissue processing holes are not intercellular like the spongiform ones are -Vacuoles are swellings of neuronal processes |
|
|
-Transmissible spongiform viral encephalopathy
-See lots of little holes in the brain -Holes can be focal or diffuse -Tissue processing holes are not intercellular like the spongiform ones are -Vacuoles are swellings of neuronal processes |
|
|
Transmissible spongiform encephalopathy
|
|
|
Transmissible spongiform encephalopathy
|
|
|
-New Variant CJD
-Has florid plaques -Pathologic proteins forms amyloid like material surrounded by vacuoles |
|
|
-New Variant CJD
-Has florid plaques -Pathologic proteins forms amyloid like material surrounded by vacuoles |
|
|
-New Variant CJD
-Has florid plaques -Pathologic proteins forms amyloid like material surrounded by vacuoles |
|
|
-New Variant CJD
-Has florid plaques -Pathologic proteins forms amyloid like material surrounded by vacuoles |