![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
Interpret client history and case study |
Make sure you know who the client is, what their diagnosis is, and why they're in hospital. Why are you doing their assessment today? IDENTIFY appropriate history, and indication |
|
|
Perform hand hygiene |
.
|
|
|
Demonstrate problem solving abilities |
Understand the need to modify questions due to: age, culture, physical/cognitive conditions KNOW: decorticate and decerebrate warning postures |
|
|
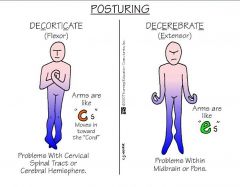
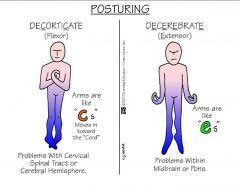
Decorticate warning posture
|
Arms are adducted and flexed, clenched fists, legs held out straight, and plantar flexed feet. The arms are bent in toward the body and the wrists and fingers are bent and held on the chest. Feet point inwards.
Caused by: bleeding, head injury, increased pressure. Damage to the cervical spinal tract, or between brain and spinal cord |
|
|
Decerebrate warning posture |
Arms are adducted and extended, wrists pronated, fingers flexed, legs stiffly extended, plantar flexion of feet, which fall outwards. Caused by: damage to the upper brain stem, midbrain, pons |
|
|
Assess for readiness |
WHS awareness: raise bed height, provides privacy with curtains, etc. |
|
|
Perform a pain assessment |
P: What provokes the pain? Q: What is the quality of your pain? Describe it R: Does it radiate anywhere? S: On a scale of 1-10, what would you rate pain? T: When did the pain start? |
|
|
Give the patient a clear explanation of the procedure |
Layman's terms: gain consent, or handle refusal |
|
|
Perform hand hygiene |
Upon leaving the room |
|
|
Gather equipment |
Penlight torch Pen Neurological observation sheet |
|
|
Perform hand hygiene |
Before touching the patient or their surroundings (5 moments of hand hygiene) |
|
|
Assess the level of consciousness |
Are they alert when you enter the room? Do eyes open spontaneously? Verbal stimuli? Or are they struggling to rouse? |
|
|
Assess orientation of client |
3 W's: who, what, where Give time to respond. Simple questions you would know the answer to. |
|
|
Assess motor response |
Give simple commands such as "wriggle your fingers" or "move your arm". Allow time to respond. |
|
|
Assess muscle strength and tone |
Limb movement: move arm laterally, against gravity, against resistance. Repeat for the legs. |
|
|
Assess pupillary activity |
Compare with pupil size chart. Ask to open eyes or hold eyelid open, shine light quickly, record reaction |
|
|
Document vital signs and neurological assessment on appropriate charts |
. |
|
|
Clean, replace, and dispose of appropriate equipment |
. |
|
|
Perform hand hygiene |
. |
|
|
Demonstrates the ability to link theory to practice |
. |
|
|
5 moments of hand hygiene!! |
. |
|
|
|
|
|
Which pain medications would we use with caution or maybe contraindicated in aclient with suspected head injury? |
Opioids: decrease level of cognition Anti-inflammatories: not to be used because the brain is in an enclosed space, and cannot handle swelling or bleeding |
|
|
At what point would the GCS indicate the need for review or medical intervention? |
A score equal to or below 8 A score that is declining (from 14 to 13, etc.) Any response that is concerning to the assessor |
|
|
What happens to a patient’s LOC when they receive drugs such as pethidine and morphine? |
It is depressed; they become tired and less-responsive. This has the potential to result in cardiac or respiratory arrest, as it slows all the symptoms down, which is not good with a pre-existing head injury. |
|
|
Can concussion progress to an unstable head injury, and if so, what might be the signs and symptoms of this progression? |
Yes; signs and symptoms may include blurred vision, slurred speech, inability to maintain consciousness, decreasing GCS score, vomiting, nausea, etc. |