![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
102 Cards in this Set
- Front
- Back
|
**Segmental level of nervous system |
8 Cervical 12 thoracic 5 lumbar 5 sacral 1 cocygeal |
|
|
**number of pairs of spinal nerves |
31 pairs |
|
|
Number of vertebra |
26 |
|
|
Where does the spinal cord start and end? |
From the foramen magnus to the level of L1-L2 vertebra |
|
|
names of the loginituninal "furrows" on the surface of the spinal cord |
Posterior or dorsal median sulcus posterior median septum anterior/ventral median fissure dorolateral sulcus ventrolateral sulcus |
|
|
Brachial plexus: which PN? |
C4-T1 |
|
|
Lumbosacrial plexus: which PN? |
L2-S3 |
|
|
**Internal Oranization: Gray Matter |
* H or butterfly shaped and divided into horn - Anterior/ventral horns: contain cell bodies of motor (efferent) neurons -Posterior/Dorsal horns: contain afferent (sensory) nerve fibers - Lateral horns (only in the thoracic and upper lumbar segments): contain cell bodies of preganglionic sympathetic neurons * Routes sensory and motor stimulus to interneurons of the CNS in order to create a response to the stimulus through chemical synapses |
|
|
**Gray matter: anterior/ventral horns |
Contain cell bodies of motor (efferent) neurons |
|
|
**Gray matter: posterior/dorsal horns |
Contain afferent (sensory) nerve fibers |
|
|
**Gray Matter: Lateral horns |
* only found in the thoracic and upper lumbar segments *contain cell bodies of preganglionic sympathetic neurons |
|
|
**Internal Organization: White Matter |
Densely packed, longitudinally running myelinated fibers * Myelin is found around almost all long nerve fibers: Acts as an electrical insulation, allows messages to pass quickly from place to place *3 zones of white matter in the spinal cord known as funiculi: Dorsal, Lateral and ventral. Specific ascending and descending tracts run in the 3 funiculi |
|
|
**3 zones of white matter in the spinal cords are known as what? |
Funiculi: Dorsal, lateral and ventral * specific ascending and descending tracts run in the 3 funiculi |
|
|
Internal Organization: Commissures |
Commissures: 1 gray and 2 white * intermediate gray: between the dorsal and ventral horns; contains interneurons and fxns to link sensory and motor activity Ventral white: contains axons and decussate from 1 side of the spinal cord to the other - location where the spinothalamic tract (pain and temp. cross) |
|
|
Spinothalamic tract location |
Ventral white commissures |
|
|
Commissures: intermediate gray |
between the dorsal and ventral horns; contains interneurons and fxns to link sensory and motor activities |
|
|
Commissures: ventral white |
contains axons that decussate from one side of the spinal cord to the other * spinothalamic tract located here |
|
|
Level variation in spinal cord structure |
Internal and external size and shape of cord vary at different levels * more rostral the tract, the more white matter bc it contains all the ascending fibers from caudal regions and the descending fibers have not yet terminated in more caudal segments |
|
|
Ascending tracts |
**conduct impoulses to the brain Nerve tracts w/in the spinal cord together with the spinal nerves provide two way communication system btw the brain and body parts outside the nervous systems * composed of axons |
|
|
Ascending tracts: names |
*Fasciculus gracilis *Faciculus cuneatus *anterior spinothalamic *lateral spinothalamic *anterior spinocerebellar *posterior spinocerebellar |
|
|
Ascending tracts: types of impulses |
Carry sensory impulses for * pain *temperature (thermal) *touch(tactile) *muscle and joint receptors (proprioception) |
|
|
**1st order neurons |
Primary afferent neurons * enters the spinal cord thorugh the dorsal root ganglion, terminates in either the spinal gray matter or medulla on the ipsilateal side |
|
|
**2nd order neuron |
Cell body in the spinal cord or medulLa, axon crosses over to the contralateral side |
|
|
**3rd order neuron |
Cell body terminates in either the brainstem, cerebellum or diencephalon |
|
|
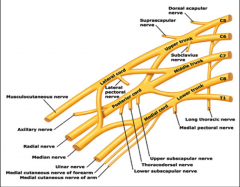
**Brachial plexus |
|
|
|
Brachial plexus: Origin- From Rami of the plexus : nerves/mm |
Nerves: dorsal scapular, long thoracic Muscles: rhomboids, lavator scapulae |
|
|
Brachial plexus: Origin- From trunks of the plexus: nerves/mm |
N- Nerves of subclavious, suprascapular MM- subclavius, infraspinatus, supraspinatus |
|
|
Brachial plexus: Origin- Fromlateral cord to the plexus: nerves/mm |
N: lateral pectoral, musculocutaenous, lateral root of the median nerve MM- pectoralis major-clavicular head, biceps brachii, brachialis |
|
|
Brachial plexus: Origin- From medial cord to the plexus: nerves/mm |
N: Medial pectral, ulnar, medial root of the median MM: pectoralis major/minor, flexor digitoram profundus, most of the mm of the hand, flexor mm of forearm( except FCU; the 5 muscle of the hand |
|
|
Brachial plexus: Origin- From the posteiror cord of the plexus : nerves/mm |
N: upper scapular, thoracodorsal, lower subsacpular, axillary, radial M: subscapularis, lat, teres minor, deltoid, teres major, brachioradialis, triceps, supinator, anconeus mm. |
|
|
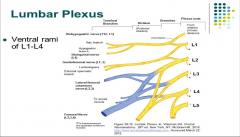
**Lumbar plexus |
|
|
|
**Dermatomes |
Area of skin supplied by somatosensory fibers of the dorsal root ganglion overlap w/ the dorsal root above and below each segment, therefore loss of one dermatomes results in virtually no loss of cutaneous sensation |
|
|
Peripheral nerves |
Spinal nerve lesion that can lead to extensive sensory loss * comprised of the dorsal & ventral nerve roots after the exit the intervertebral foramen *spinal nerves and mixed. They contain both afferent/efferent neorons |
|
|
**Myotomes |
* Groups of mm innervated via the ventral roots by a segment of the spinal cord *most mm innervated by motor axons arising from multiple segments *certain mm whose weakness or atrophy may indicated damage to a single nerve root |
|
|
**Myotome scan: C1 &2 |
Neck flexors (SCM) |
|
|
**Myotome scan: C3 |
Lateral neck flexors |
|
|
**Myotome scan: C4 |
Trapezius, lavator scapula and diaphram |
|
|
**Myotome scan: C5 |
Supraspinatus, intraspinatus, deltoid, biceps |
|
|
**Myotome scan: C6 |
Biceps, supinator, wrist extensors |
|
|
**Myotome scan C7 |
Triceps and finger flexors |
|
|
**Myotome scan: C8 |
FInger flexors, thumb extensors and adductors |
|
|
**Myotome scan: T1 |
Finger abduction and adduction |
|
|
**Myotome scan: upper body |
C1 and 2: Neck Flexors (SCM) C3: Lateral Neck Flexors C4: Trapezius, Levator Scapula and Diaphram C5: Supraspinatus, Infraspinatus, Deltoid, Biceps C6: Biceps, supinator, wrist extensors C7: Tricep and Finger flexors C8: Finger flexors, thumb extensors and adductors T1: Finger Abduction and Adduction |
|
|
**Myotome: Respiration |
MM: diaphragm Root: C3, C4, C5 |
|
|
**Myotome: abduction of arm |
MM: Deltoid Root: C5 |
|
|
**Myotome: flexion of forearm |
MM: Biceps Root: C5 MM: Brachioradialis, root: C6 |
|
|
**Myotome: Extension of forearm |
MM: Triceps Root: C7 |
|
|
**Myotome: Extension of Knee |
MM: quadriceps root: L3, L4 |
|
|
**Myotome: Dorsiflexion of great toe |
MM: extensor hallucis longus Root: L5 |
|
|
**Myotome: plantar fexion |
MM: gastrocnemius Root: S1 |
|
|
**Myotome Scan: L1-L3 |
Iliopsoas |
|
|
**Myotome Scan : L2 |
Psoas, Hip adductors |
|
|
**Myotome scan: L3 |
Psoas, Quads |
|
|
**Myotome scan: L4 |
Tibialis anterior, extensor hallucis |
|
|
**Myotome scan: L5 |
Extensor Halluces, Peroneals, Glut Med |
|
|
**Myotome scan: S1 |
Calf, Hamstring, Gluteals, Peroneals, Plantarflexors |
|
|
**Myotome Scan: S2 |
Calf, Hamstring, Gluteals, Plantarflexors |
|
|
Action- Flexion of shoulder: MM, PN, NR, Plexus |
MM: Deltoid, coracobrachialis PN: Axillary, Musculocutaneus
NR: C5-C6, C6-C7 Plexus: Brachial |
|
|
Action- Extension of shoulder: MM, PN, NR, Plexus |
MM PN NR Lat's Thoracodorsal C6-C8 Teres Major Subscapular C5-C6 Deltoid (post) Axillary C5-C6 Plexus: Brachial |
|
|
Action- Abduction Arm: MM, PN, NR, Plexus |
MM PN NR Supraspinatus Suprascapular C4-C6 Deltoid Axillary C5-C6 Plexus: Brachial |
|
|
Action- Elbow Flexion: MM, PN, NR, Plexus |
MM PN NR Biceps Brachii Musculocutaneous C5-C6 Brachialis Musculocutaneous C5-C6 Brachioradialis Radial C5-C6 Plexus: Brachial |
|
|
Action- Elbow Extension: MM, PN, NR, Plexus |
MM: Triceps Brachii
Plexus: Brachial |
|
|
Action- Wrist Flexion: MM, PN, NR, Plexus |
M PN NR F. Carpi Radialis Median C6-C7 F. Carpi Ulnaris Radial C8-T1 Plexus: Brachial |
|
|
Action- Wrist Extension: MM, PN, NR, Plexus |
M/PN/ NR E. Carpi Radialis Longus/ Radial/C6-C7 E. Carpi Radialis Brevis/ Radial / C6-C7(C8) Extensor Carpi Ulnaris/ Radial/ C6-C8 Plexus: Brachial |
|
|
**Major Peripheral Nerves- UE: Axillary |
MM & skin of ant., lat & post region of arm |
|
|
**Major Peripheral Nerves- UE: Musculocutaneous |
MM of arm on the ant. side & skin of forearm |
|
|
**Major Peripheral Nerves- UE: Median |
MM of forearms and MMs & skin of hands |
|
|
**Major Peripheral Nerves- UE: Radial |
MM of arms on the post. sides/ skin forearms & hand |
|
|
**Major Peripheral Nerves- UE: Ulnar |
MM of forearms & hands and skin of the hands |
|
|
Median Nerve: Injury |
Result in server disability (IE. Carpal tunnel Syndrome) |
|
|
High Median Nerve injury: causes
|
Proximal forearm or above: Loss of: *Wrist flexion strength, ulnar deviation of wrist, thumb opposition, finger flexion of thumb, index and long finger IP joints *When making a fist the ring &small fingers flex while the long & index tend to stay straight |
|
|
Low Median Nerve Injuries: causes |
Fingers are still able to flex, but thumb opposition is often lost |
|
|
Radial Nerve Injury: Results in |
* Loss of extension of the wrist, fingers and thumb (difficulty in grasping objects leads to significant disability_) |
|
|
Ulnar Nerve Injury: results in |
* hand and finger pain * Weakness of hand *Numbness, burning and decreased sensation *Pain and tingling in the 4th and 5th fingers |
|
|
Action: Hip Flexion: MM/PN/NR/P |
MM/PN/NR Psoas Major/femoral/ L1-L3 Iliacus/ Femoral / L2-L3 Plexus: Lumbar |
|
|
Action: hip Extention MM/PN/NR/P |
MM/Pn/NR Gluteus Max/ inferior gluteal/ L5-S2 Semitendinosus/ Sciatic (tibial) L5-S2 (L4) Plexus: Lumbosacral |
|
|
Action: hip abduction MM/PN/NR/P |
MM/PN/NR Gluteas Medius/ Superior gluteal/ L40S1 Plexus: Lumbosacral |
|
|
Action: Knee Flexion MM/PN/NR/P |
Biceps femoris (long head)/ Sciatic (tibial)/ S1-S3 Biceps femoris (short head)/ Sciatic (common peroneal)/ L4- S2 Semitendinosis/ Sciatic (tibial)/ L4-S2 Plexus: Sacrial (LH), Lumbosacral (SH, SemiT) |
|
|
Action: knee extension MM/PN/NR/P |
Quadriceps Femoris/ femoral/ L2-L4 Plexus: Lumbar |
|
|
Action: Ankle plantar flexion MM/PN/NR/P |
MM: Gastrocnemius, soleus PN: Tibia NR: S1-S2 Plexus: sacral |
|
|
Action: ankle Dorsiflexion |
MM: tibialis anterior PN: deep peroneal NR: L4-S1 P: Lumbosacral |
|
|
**Major PN of LE: Obturator |
Supplies the adductor mm of the thigh **hernia surgery can cause injury** |
|
|
**Major PN of LE: Femoral |
Divides into many branches: Supplies motor impulses to mm of the anterior thigh receives sensory impulses from the skin of the thighs& legs |
|
|
**Major PN of LE: Sciatic |
* Largest and longest nerve in the body *passes downward into the buttock &descends into the thigh *divides into Tibial and common fibular N. *supplies mm and skin in the thighs, legs and feet ** tibial nerve caused by ankle immobilization** |
|
|
Patents with obturator nerve injury have: |
Possible numbness and pain radiating into their inner thigh adduction thigh weakness can occur, which causes gait and posture instability |
|
|
Femoral nerve injury: results in |
*loss of knee extension *loss of cutaneous sensation on the medial side of the leg and foot * pain felt over the femoral nerve distribution due to compression of L2-4 N. roots by an intervertebral disc |
|
|
Sciatic Nerve injury results in: |
*Sensation changes of the back of the calf or the sole of the foot - Numbness, decr. sensation, tingling, burning sensation, pain (severe), abnormal sensations * weakness of the knee or foot - Difficulty walking, inability to move the foot, inability to bend the knee (in sever cases) |
|
|
**Neuropathies |
Disease of the PN system: Segmental demyelination Axonal degeneration wallerian degeneration |
|
|
**Neuropathies: cause |
variety of diseases: *Herpes zoster (shingles) *Infection (GBS) *malnutrition, vit. deficiency, toxic to meds, metabolic complication from DM, liver & kidney failure, hypothyroidism, hereditary *Mechanical forces/trauma: cut or scratched, edema/ inflammation, compression |
|
|
Segmental demyelination |
Myelin degenerates by the axon is spared |
|
|
Axonal degeneration |
Distal degeneration of the axon |
|
|
Wallerian degeneration |
Both the distal axon and surrounding myelin degenerate |
|
|
Polyneuropathies |
*usually involve both sensory and motor impairments *Sensory impairments are usually bilateral & in a grove like or stocking distribution * affects the distal extremities first (dying back effect) *affecting primary somatosensory neurons can cause sensory ataxia **entire foot/hand vs. certain section |
|
|
Diabetic Neuropathy: etiology |
Prolonged exposure to high blood glucose levels * involves sensory, motor and autonomic nerve fibers |
|
|
Diabetic neuropathy (polyneuropathies): Symptoms |
can be wide spread based on the diverse presentation: include weakness &sensory disturbances (numbness, tingling, or pain * wasting of m. in feet/hands "stocking glove" sensory and distribution impairments, orthostatic hypotension, urinary impairment and significant pain * usually involve decr. sensation in the distal LE |
|
|
Diabetic neuropathy (polyneuropathies): PT intervention |
Pain management, foot care and overall fitness |
|
|
Guillian-Barre syndrome: etiology |
Involves demyelination of PN resulting in axonal degeneration |
|
|
Guilian-Barre syndrome: symptoms |
*usually the legs are affected 1st & weakness ascending to the trunk. usually symmetrically *motor loss is more predominant than sensory loss; absent DTR's *progresses rapidly, can lead to total paralysis and death (2-5%) * neurological signs totally or partially solves over weeks or months (peaks w/in 2-4 wks) |
|
|
Guillian-barre' syndrome: PT intervention |
Strengthening, mobility, WC or orthotic Rx, and/or assisted device training |
|
|
Charcot-marie-tooth disease |
*genetic PN disorder affecting both sensory and motor fibers *presents w/ distal weakness and sensory loss * onset in the teens or twenties and progresses gradually over a lifetime |
|
|
what type of roots are dorsal and ventral horns? |
Sensory roots: dorsal Motor roots: ventral |
|
|
3 causes or brachial plexus injuries |
Erbs-palsy - causes paralysis in arm Stinger- quick stretch to brachial plexus anterior shoulder dislocation |