![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
39 Cards in this Set
- Front
- Back
|
Parts of the neuron |

Dendrites Soma Axon hillock Node of Ranvier Presynaptic terminal |
|
|
Neuron's Function |
Special type of cell that sends, receives and stores electrical and chemical information Able to hold and control an electrical charge by controlling the concentration and the flow of ions across it's membrane TWO MECHANISMS 1. Diffusional forces 2. Electrical forces |
|
|
Membrane Potential |
Charges line up along membrane Electrostatic attraction Bulk of intracellular and extracellular fluid is electrically neutral thebraingeek.blogspot.com |
|
|
Equilibrium |
No net force driving ions to move Diffusional and electrical forces are balanced Equilibrium potential – the membrane voltage that balances the concentration gradient force No action potential will be made!! |
|
|
Resting Membrane Potential |
*Neuron is not active but can be if stimulated *Charge is due to unequal concentrations of ions inside and outside the cell *Controlled by permeability * RMP = -70mV |
|
|
Depolarization |
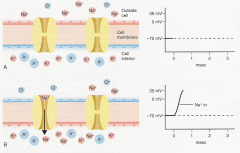
Brief change Inside of cell becomes much less negative More excitable Na+ is pumped into axon Increases charge toward threshold (-55 mV) |
|
|
Repolarization/ Hyperpolarization |
Inside of the cell become more negative as K+ is pumped out of the cell The charge of the cell actually become more negative than resting potential (hyperpolarization) Hyperpolarization: Inhibitory |
|
|
Two ways in which changes in polarization occur |
Local Potentials -Graded in size and duration -Additive/always happening -Smaller than an action potential Spread only a small distance Most information coming from soma is local ------------------------------------------------------------------- Action Potentials ALWAYS SAME SIZE AND DURATION All or nothing Can be repeatedly regenerated along a long distance |
|
|
Local Potentials |
* Initial change in a RMP at a receiving site? *May be a depolarization or a hyperpolarization? How does a local potential hyperpolarize? *Spreads passively only a short distance before degrading -Larger one can spread farther than a smaller one |
|
|
Synaptic Potential |
*One neuron stimulates the next one *Depolarizing or hyperpolarizing * The more neurotransmitter released into the synapse,the greater the synaptic potential |
|
|
Spatial vs Temporal Summation |
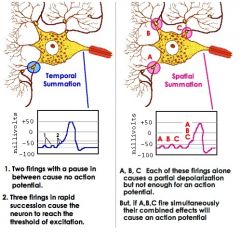
Spatial *Several nerves firing at one time * Leads to action potential Temporal * One nerve firing rapidly * Leads to an action potential |
|
|
Action Potentials |
*Rapid reversal in membrane potential *Caused by depolarization from local potential that reaches threshold (-55mV) *Propagated along the axon to synapse *Voltage-gated ion channels -Ion channels that open in response to depolarization that reaches threshold -Located in the axon |
|
|
Clinical Significance of Action potential production dysfunction |
*Constant depolarization: high tone
*Cannot reach 30-->parkison’s patient, takes more to get it firing |
|
|
Propagation along the axon |
The action potential at the very beginning of the axon begins a chain reaction, opening voltage-gated channels in the next section--> leading to another AP |
|
|
Speed of Propagation affected by |
Increased Diameter of axon *Decreases axoplasmic resistance that allows a faster flow Myelination *Increase membrane resistance which decreases leaking of charges across membrane *Heavier myelination- faster conduction/ insulation Nodes of Ranvier-Breaks in myelin covering with high concentration of NA+ and K+ channels. allows for generation of new action potential to next node known as saltatory conduction |
|
|
Causes of Decreased Synaptic Transmission
|
Anoxia- lack of oxygen-->cell death Paralysis Due to Poisoning -Snake venom Ach allows nerves to fire--> snake venom blocks Ach? -block what? how? Spasm Due to Cholinergic Drugs -Simulates Ach -Lip smacking Synaptic Fatigue -Addiction -Need more and more to get same neurotransmitter reaction |
|
|
Types of Synapses |

To another neuron *Axon to dendrite *Axon to soma *axon to axon To muscle To gland |
|
|
Parts of the Synapse |
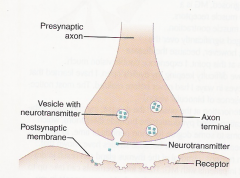
Presynaptic terminal Vesicles (released as the action potential reaches axon terminal/synapse) Postsynaptic terminal Receptors *Key in Lock specificity (Neurotransmitters) --> open ion channels (Ligand-gated) --> activity in postsynaptic cell Synaptic cleft |
|
|
Functioning of the Synapse |
1) Action Potential arrives 2) Voltage-gated Ca+ channels open 3) Movement of synaptic vesicles and release of neurotransmitters into synaptic cleft (Exocytosis) 4) Neurotransmitter binds to receptor and changes it shape 5) Opens ion channel |
|
|
Clearing of the Cleft |
Endocytosis - Reuptake into the presynaptic terminal Enzymes- break down neurotransmitters Diffusion- spread out into extracellular fluid |
|
|
Local Postsynaptic Potentials |
Graded, not "all or nothing" Excitatory Postsynaptic Potential (EPSP) *Sodium (Na+) or calcium (Ca++) *depolarization of membrane *summation of EPSP--> Action potential *Epsp cause muscle contraction * Acetylcholine--> influx of sodium into muscle * Norepinephrine Acetylcholine and norepinephrine sit outside CNS and PNS |
|
|
Inhibitory Postsynaptic Potentials |
Neurotransmitter opens chloride (Cl-) or potassium (K+) channels -->Small hyperpolarization decreases possibility of an action potential when they start to summate, their purpose is meant to stop the action |
|
|
Acetylcholine |
Excitatory Antagonist *Botchulinum toxin *Clinical use: High tone patient given Botox Action *produce muscle action, used for memory in brain Dysfunction Too Much:, (but GABA still works) Huntington’s chorea, whole body movement (hyperkinetic movement) Not enough: paralysis, caused by snake venom (starts with PNS--> CNS) Alzheimer's Disease -Too little: associated with increased cerebral plaque build up. -----> Aricept, a cholinenase inhibitor blocks the enzyme that breaks down Ach. Myasthenia Gravis Effects PNS, weakening in local area |
|
|
Norepinephrine |
Excitatory Antagonist *Betablockers *Clinical use: Significant in Migraine and glaucoma Action * noradrenaline, alertness, arousal and attention level, stress hormones, fight or flight mechanism Clinical Dysfunction Too Much: : Implicated in fear, anxiety disorders and pains disorders |
|
|
GABA |
Inhibitory Found in Valium, Phenobarbital, and Baclofen Increase effects of body's own GABA Clinical Dysfunction WITHOUT GABA (too little), High tone. It stops Ach from firing constantly. In insomnia and anxiety, it puts on the brakes at certain point.--> too little--> both conditions can go out of control Too much: Locked-in syndrome (constant braking) |
|
|
Dopamine |
Excitatory/inhibitory Action *Motor system, cognition, motivation and reward system Clinical Dysfunction Not enough: Parkinson's disease--> motor and cognition issues along with impulsivity Too Much: Schizophrenia/addiction. Hallucinations are an over-working of the brain via dopamine. Paranoia--> overthinking L-Dopa: Cannot directly take dopamine due to blood-brain barrier--> L-Dopa convert to dopamine after it passes through barrier |
|
|
Serotonin |
Inhibitory Action Regulate sleep/circadian rhythms Emotional control Pain regulation Vomiting Feeding behaviors (ED) Too little Depression, suicidal, bulimia (self-hatred) Too Much OCD, anger, suicidal, anorexia (control) SSRIs |
|
|
Glutamate |
Excitatory Most common neurotransmitter Action Main role in learning and memory, preps brain to take in new information Clinical Dysfunction Too Little: Alzheimers, cognitive issues with short term memory |
|
|
Substance P |
Excitatory Action Implicated in pain Neuromodulator (Maintaining a state) Regulation of mood, anxiety and stress Role in neurogenesis respiratory rhythm, nausea and pain perception Clinical Dysfunction Too Much : Fibromyalgia--> pain triggering |
|
|
Endorphins |
Excitatory Action Natural Painkillers OVERRIDES SUBSTANCE P Opioids produced by body Runner's high: Endorphins override pain from leg |
|
|
Spinal Versus Cranial Nerves |
Spinal afferent and efferent nerve lines Less specialization 1st 2nd and 3rd neuron Cranial Can be afferent or efferent (or both) Special sensory and motor Just upper and lower neuron |
|
|
Parts of Eye |
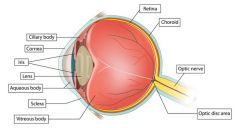
Iris-Constricts and dilates eye Lens-reflects light to the back Retina-photoreceptor for optic nerve, starts action potential down optic nerve Optic Disk- blind spot |
|
|
Oculomotor control |
Cranial Nerves (III)Oculomotor (IV)Trochlear (VI) Abducens Purpose: to change/maintain visual fixation Medial Longitudinal Fasciculus: connects ocular motor nerves with vestibular-cochlear nerve and accessory to create balance and equilibrium Reflexive Types of Movement Conjugate- eyes are moving in same direction (working together) Vergent- converging, come to together in center to focus or Averge moving away Pursuit/Tracking- focus and follow Saccade- shift position, jump fast Reflexes Pupillary- Direct reflex, light shined in one eye--> constriction Consensual- (indirect) other eye. oculomotor parasympathetic chain constricted. Both eyes need to be constricted Accommodation- allows us to focus eyes. Lens is shifted to accommodate for near vision |
|
|
Types of Nystagmus |
Repetitive, uncontrolled movements End range- one or twice normal, if it keeps going, abnormal Post-rotary- going to turn causes it, difficulty w/ balance Optokinetic- jumping to things, as lamp posts pass you by when driving |
|
|
Other Oculomotor Dysfunction |
Strabismus- eyes are not symmetrical, not aligned
Diplopia- double vision Ptosis- drooping eyelid Dilation of pupil and decreased accommodation Due to high pressure on brain |
|
|
Taste |
FACIAL NERVE Taste buds located on tongue Most found on walls of papillae of tongue Opens to a pore and sensory cell Chemoreceptor cause AP in nerves--> PARIETAL LOBE AND INSULA ------------------------------------------------------ Sweet-tip of the tongue Salty - sides of the tongue Bitter and sour - back of the tongue --------------------------------------------------------- Influenced by food texture, aroma, temp, and appearance Hot pepper stimulates free nerve endings (pain) CONNECTIONS WITH Hypothalamus-controls hunger Amygdala- emotion and memory |
|
|
Process of Hearing and Dysfunction |
Ossicles - sit at 90 degrees to each other, allow for hearing at all angles Cochlear- hairs on sensory receptors, vibrates Eustachian tube- how we equalize pressure ex- children have more of a horizontal tube--> more problems with ear popping and ear infections DYSFUNCTIONS Conductive deafness: *Wax in ear *Louder in affected ear when humming Sensorineural deafness *Nerve somewhere around cochlear *Louder in unaffected ear |
|
|
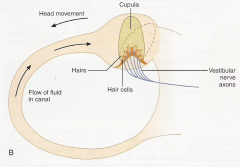
Vestibular Process |
|
|
|
Pharynx |
Cranial Nerves (concerning pharynx): Facial (somatic sensory) Glossopharyngeal (somatic sensory) Vagus (somatic motor/sensory and visceral motor) Functions Passage way Swallowing *Voluntary phase *involuntary (reflexive) Epiglottis- controlled by vagus nerve *soft palate closes off nasal passages *epiglottis covers the opening to trachea--> aspiration- pneumonia is affected |