Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
Pupillary reflexes
|
light reflex
accommodation reflex blink (corneal) reflex |
|
|
Light reflex
(induced by, what happens to each eye) |
induced by bright light shown into pupil of one eye
constriction of the pupil (direct or ipsi response) small constriction of other pupil (consenual or contra response) |
|
|
Parasympathetic control of pupil constriction
(whole pathway) |

|
|
|
Constriction
PSNS or SNS? |
PSNS
|
|
|
Lesions of Ed-West nucleus or
oculomotor nerve |
mydriasis (abnormal dilation ipsi to lesion)
impaired direct constriction of ipsi pupil (when light shined in) but intact consensual constriction of contra pupil impaired consensual response of affected pupil (when light directed at unaffected pupil) |
|
|
Dilation
PSNS or SNS? |
SNS
|
|
|
Sympathetic control of dilation
|

|
|
|
Lesions involving SNS control of pupil dilation result in _
and _ |
ipsi miosis (abnormal constriction of pupil on side of lesion)
impaired dilation of ipsi pupil |
|
|
Coordinated eye movements
(name) |
saccades (vol or invol)
smooth pursuits (invol/reflexive) vestibulo-ocular movements (invol/reflex) optokinetic movements (invol/reflex) |
|
|
Role of invol eye movements
(3) |
compensate for disturbances to visual field (ex. moving head), allowing eyes to remain fixed on object of interest
compensate for adaptation by retina, so that the perception of objects does not actually disappear as a result of adaptation by photoreceptors scanning the features of an object, critical for object recognition |
|
|
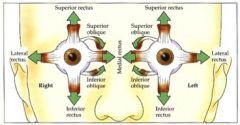
intorsion
|
movement of upper pole of eye inwards
|
|
|
extorsion
|
movement of upper pole of eye outwards
|
|
|
convergence
|
both eye adduct
medial rectus |
|
|
divergence
|
both eyes abduct
lateral rectus |
|
|
Motor Neuron Innervation of Extraocular Eye Muscles
|
|
|
|
Saccades
(what, function) |
rapid, ballistic movement that change point of fixation
function to direct eyes to object of interest only type of coordinated eye movement that can be performed easily voluntary |
|
|
Saccades
(two brainstem regions) |
horiz gaze center:
paramedian pontine reticular formation (PPRF) vert gaze center: upper (rostral) midbrain reticular formation Most saccade movements are combo of horiz and vert |
|
|
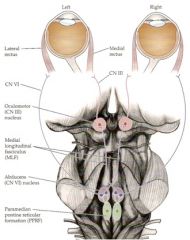
Pathway Involved in Generation of Horizontal Gaze/Saccade
|
|
|
|
Horizontal Saccades:
neurons of _ project to _ these innervate _ via _ and also innervate _ via _ neurons of the oculomotor nucleus innervate _ via _ |
PPRF to ipsi abducens nucleus in pons
abducens nucleus to ipsi LR via CNVI abducens nucleus to contra oculomotor nucleus via MLF oculomotor nucleus to ipsi medial rectus via CNIII |
|
|
Saccade to right side of binocular field (both eyes right)
activation of _ PPRF to _____ |
right PPRF to:
right abducens nucleus and nerve, causing contraction of LR of right eye, moving right eye to right (abduction) activate right abducens neurons, which activate left oculomotor nucleus and nerve, causing contraction of medial rectus of left eye, moving left eye to right (adduction) |
|
|
Gaze Deficits
dysconjugate gaze |
eyes in different position
lesions of neural circuitry underlying saccades/gaze causing diplopia |
|
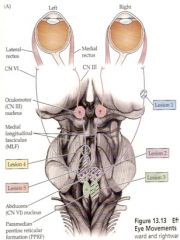
Deficits in Horizontal Eye Movements
|

|
|
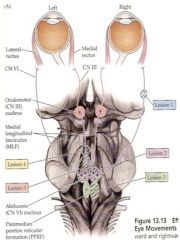
Lesions of abducens nerve (1)
|

impaired abduction ipsi eye (*abducens palsy*) causing
*horizontal diplopia*, but at rest gaze medial (*medial strabismus*) |
|
|
Deficits in Horizon Gaze
(due to _ _ _ _) |
stroke
diabetes head trauma myelin degen |
|
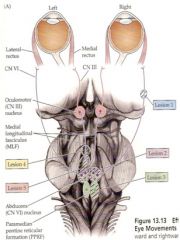
Lesions of abducens nucleus
(Lesion 2) |

impaired abduction in ipsi eye and
impaired adduction in contra eye so gaze towards the side of lesion impaired called *lateral gaze palsy* gaze preference at rest away from lesion |
|
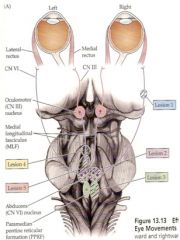
Lesion of PPRF
(Lesion 3) |

impaired abduction in ipsi eye and
impaired adduction in contra eye so gaze towards the side of lesion impaired called *lateral gaze palsy* gaze preference at rest away from lesion |
|
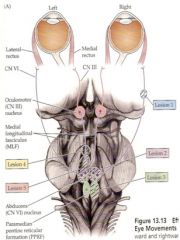
Lesion of MLF
(lesion 4) |

internuclear ophthalmoplegia (INO)
impaired adduction of ipsi eye nystagmus in contra eye |
|
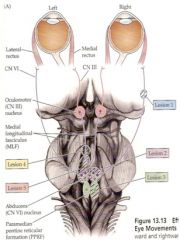
Large lesions that encompass:
MLF, abducens nucleus, and/or PPRF (lesion 5) |

ipsi INO
lateral gaze palsy, so ipsi eye can not abduct or adduct contra eye eye can't adduct, termed *one-and-a-half syndrome* |
|
|
nystagmus
|
rhythmic form of eye movement comprised of slow movements in one direction and rapid movements in other direction
|
|
|
bilateral lesions of the PPRF or abducens nucleus
|
gaze paralysis
(total loss of horizontal gaze) |
|
|
lesions of oculomotor nerve
|
impaired adduction ipsi during gaze (oculomotor palsy)
at rest: lateral strabismus down and out diagonal diplopia pupil on side of lesion unresponsive to light mydriasis |
|
|
oculomotor dysfunction useful diagnostic tool for _ aneurysm
|
posterior communicating artery
|
|
|
trochlear nucleus lesions
|
contra trochlear palsy:
extorsion of eye vertical diplopia when eye looks nasally and looks down |
|
|
trochlear nerve lesions
|
ipsi trochlear palsy:
extorsion of eye vertical diplopia when eye looks nasally and looks down |
|
|
Higher control of Gaze and Saccades
PPRF receives input from _ |
contra superior colliculus
|
|
|
Higher control of Gaze and Saccades
Superior Colliculus |
PPRF receives input from Sup Colliculus
sup colliculus receives direct visual input from optic tract to facilitate reflexive saccades in direction of visual stimuli SC receives auditory and somatosen input, which facilitates reflexive saccades in the direction of touch or noise |
|
|
lesions of superior colliculus
|
deficits in involuntary saccades
|
|
|
for voluntary saccades, PPRF receives input from
|
contra FEF
|
|
|
lesions of FEF
|
deficits in voluntary gaze
|
|
|
Lesions to FEF
|
deficits in voluntary gaze contra to lesion
at rest: towards side of lesion |
|
|
Right way eyes
|
gaze at rest *away* from side of weakness
lesion must be oppo side of brain to weakness thus eye gaze toward side of lesion indicating *frontal cortex* lesion |
|
|
Wrong way eyes
|
gaze preference towards (ipsi) the side of weakness
lesion oppo side of body to weakness eye gaze contra to lesion lesion of pons (PPRF or abducens nucleus) |
|
|
Vestibulo-ocular reflexes (VOR)
|
compensate for disturbances to visual field during head and body movements, allow eyes to remain fixed on object of interest:
head rotation causes eye movement in oppo direction Projections from *vestibular nuclei* innervate contra abducens nucleus via MLF |
|
|
Pathways controlling VOR
|

if head moves horiz to left, left vestibular nuclei activated which:
activate right abducens nucleus to cause abduction of right eye (right eye to right) activate left oculomotor nucleus to cause adduction of left eye (left eye moves right) |
|
|
Lesion in MLF in pons
|
bilateral VOR deficits directed towards side of lesion
(the lesion would be on the opposite side to the direction of head turn that elicited VOR deficit) right lesion results in loss of right horiz VOR when patient moves head to left |
|
|
Lesion of MLF in midbrain
|
loss of horiz VOR in eye ipsi to lesion in the direction away from the lesion
(the lesion would be on same side as the direction of head turn that elicited the VOR deficit) left lesion will result in loss of right horiz VOR in left eye when the patient moves their head to the left b/c left eye no longer adducts |