Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
|
Name 2 common bacteria that cause encephalitis.
|
Streptococcus and staphylococcus
|
|
|
How does encephalitis look different form metastatic carcinoma histologically?
|
They both have single or multiple lesions in the brain but encephalitis has more necrosis.
|
|
|
What is observed outside the fibrous layer of the brain abscess, histologically?
What is in the cavity of the brain abscess? |
Outside the fibrous layer - edema and some reactive gliosis
Inside the cavity - free-floating foamy macrophages, lymphocytes and few neutrophils |
|
|
is the causative oragnism bacterial, viral, or fungal if the following are observed histologically:
Perivascular inflammation with lymphocytes, plasma cells, macrophages, but NO netrophils. A few microglia nodules. |
Viral
|
|
|
A pt has flaccid paralysis and muscle atrophy in the lower extreimities.
Histology reveals: 1. perivascular MNCs in anterior horn 2. gliosis 3. microglial nodules. What type of CNS infection is this? cause? |
Polymyelitis caused by RNA virus or enterovirus
|
|
|
What do vitamin B12 deficiency and vaculolar myelopathy have in common?
What is the cause of vacuolar myelopathy? |
they both have degeneration of posterior and lateral columns of the spinal cord.
Direct infection of HIV |
|
|
An AIDS pt comes in with no somatic sensation (proprioception, touch, vibration) in both legs and they are also paralyzed.
What is the first Tx option? |
Infusion of vitamin B12.
Vitamin B12 deficiency ca cause degeneration of posterior and lateral columns in the spinal cord. |
|
|
The autopsy of an AIDS pt reveals:
Multiple gray necrotic lesions in white matter Demyelination and inclusions in oligodendrocytes. What is the causative organism? what is this disorder called? |
Caused by JC polyoma virus (papovavirus)
Progressive multifocal leukoencephalopathy (PML) |
|
|
What is the most common fungus that causes CNS infection in AIDS patients.
What is the most common organism that causes CNS infection in AIDS patients. |
Most common fungal - cryptococcus
Most common - Toxoplasmosis |
|
|
What 2 fungi are angioinvasive?
How are they different structurally? |
Aspergillosis - septae hyphae and branching at acute angle
Mucor (zygomycosis) - nonseptae hyphae and braching at wide 90 degree angle |
|
|
What CNS structure does cryptococcus most commonly infect?
|
Meninges.
|
|
|
With candidiasis encephalitis, what histological features do you expect to find?
|
Yeast forms and pseudohyphae (from budding)
Microabscesses or granulomas |
|
|
What are 2 forms of toxoplamosis?
Describe them. |
Bradyzoite - encysted
Tachyzoite - free |
|
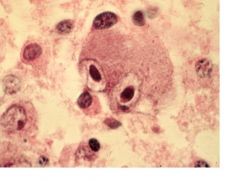
An autopsy of an AIDS pt revealed hemorrhagic, necrotizing encephalitis grossly.
The above section was obtained. What is the causative organism? |
Cytomegalovirus
Enlarged cell with intranuclear and intracytoplasmic inclusions (Owl eyes appearance) |
|
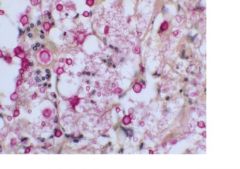
This section was obtained from meninges.
What is the causative organism? How do you know? |
Cryptococcus (most common fungus to infect meninges)
Round pink structures are yeasts that are budding. |
|
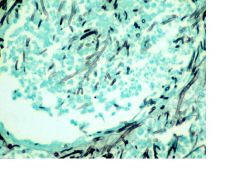
This is a section of a blood vessel in the brain with encephalitis.
What is the causative organism? how do you know? (list 2 histological features observed) |
Aspergillus
Branching at acute angles. septae hyphae |
|

This is a section of spinal cord stained with myelin stain.
What is the disorder called? List 2 causes. |
vacuolar myelopathy.
Direct HIV infection of the spinal cord. B12 deficiency |
|
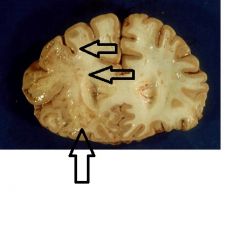
this is a section of brain with encephalitis.
What is observed grossly? What virus is cause such pathology? what is this called? |
Gray necrotic lesions in White matter.
JC polyoma virus Progressive multifocal leukoencephalopathy (PML) |
|
|
what is the difference b/t septic and aseptic meningitis?
|
Septic - purulent and caused by bacteria
Aseptic - non-purulent and caused by virus, mycobacterium, fungus, or amoeba. |
|
|
list and explain 3 signs of meningeal irritation.
|
1. Nuchal rigidity - stiff neck, resistance to passive flexion of the neck, cannot flex the neck
2. Kernig's sign - resistance to extension of the leg at the knee when the thigh and leg are flexed 3. Brudzinski's sign- passive flexion of the neck causes flexion of the hips and knees. |
|
|
What 2 cytokines in the CSF confirm the diagnosis of meningitis?
|
TNF-alpha and IL-1
|
|
|
Name the #1 organism that causes septic meningitis in the following age groups:
1. Neonates 2. 2-23 months 3. College students/young military personnel 4. 60+ |
1. Group B strep
2. Strep Pneumoniae 3. Neisseria Meningitidis 4. Strep Pneumoniae |
|
|
Name 2 vaccines that are targeted against Pneumococcal meningitis.
This is used against what organism? What is the indicated age group for each vaccine? Is it conjugated? |
Against S. Pneumoniae
Prevnar - conjugated and indicated for children under 2 Pneumovax - for >65 YO and for high risk individuals; not for children under 2 |
|
|
Name 2 vaccines used against N. meningitidis. Conjugated?
|
Menomune - non-conjugated
Menactra - conjugated |
|
|
Indicate normal CSF values.
Glucose, protein, cell number, appearance. |
Glucose - 50-80mg/dL
Protein - 15-40 mg/dL 0-5 lymphocytes but no PMN clear |
|
|
Indicate if the meningitis is viral, bacterial, or fungal?
glucose - 30 mg/dl protein - 500 mg/dl turbid presence of many PMN. |
Bacterial
|
|
|
Indicate if the meningitis is viral, bacterial, or fungal?
glucose - 70mg/dl protein - 90 mg/dl presence of MNCs about 400/ml clear |
viral
|
|
|
Is lumbar tap indicated in a pt with suspected meningitis with papilledema? why or why not?
|
NO
Papilledema indicates increased ICP. with LP, uncal or transtentorial herniation can occur and this will cause cardiorespiratory depression. |
|
|
If a pt has nuchal rigidity, positive Kernig sign, presence of PMN in the CSF AND petechial rash, What organism do you suspect?
|
Meningococcal meningitis due to N. meningitidis.
|
|
|
What new findings in the serum contrast bacterial from vial meningitis?
|
serum procalcitonin level above 0.5ng/mL indicated bacterial meningitis.
|
|
|
What immunological problems exist in the CNS that compromises eradication of bacteria? (3)
|
1. Phagocytes (microglia) cannot engulf encapsulated bacteria; phagocytes with decreased fxn and conc.
2. Lower conc of Igs in CSF 3. Exit pump/different diffusion properties of antibiotics |
|
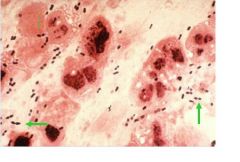
The green arrows indicate what kind of organism?
In what 2 age groups, is this organism the most common cause of meningitis? |
Gram + diplococci
S. pneumnoiae 2-23 months and 65 + |
|
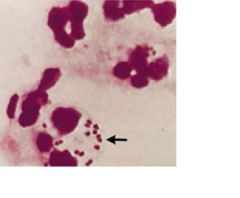
The black arrows indicate what organism?
In what age group do you suspect this organism to be the main cause of meningitis? |
N. meningitidis. (gram negative diplococci)
2 month -18 yr olds (infants, college students, and military personnels) |
|
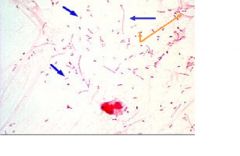
This is a sample from CSF. What organism is indicated by the blue arrows?
What would they look like in serum? |
Hemophilus influenza type B (gram negative rods)
Look more like cocci in serum |