![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
108 Cards in this Set
- Front
- Back
|
Define ARF |
Rapid rise in BUN or creatinine Hours, days, weeks |
|
|
What are some causes of ARF that occur over a few days? (3 points) Hint: What causes acute rise in K+/Pigment. What may be injected during an imaging study Few days post infection |
Rhabdomyolysis IgA nephropathy Contrast induced |
|
|
What are some causes of ARF that occur over a few weeks? (3 points) Hint: One antibiotic, others related to infection and sequalae |
Poststreptococcal Glomerulonephritis Aminoglycosides |
|
|
What is the timeframe for ARF in 1. Post infection 2. IgA 3. Aminoglycosides |
1. 1-2 weeks 2. Only days 3. 5-10 days as it takes time to build up? |
|
|
What causes acute tubular necrosis? (4 points) |
1. Hypotension 2. Rhabdomyolysis 3. Blood transfusion reactions 4. Septic shock |
|
|
How can you reduce the risk of aminoglycoside kidney injury? Reduce dose or reduce increase timing between doses? |
Decrease timing intervals |
|
|
What are the symptoms of uraemia? (8 points) What is the definition? Hint: Think of normal functions of the kidney and also prevention of degranulation |
Defined as severe renal failure requiring dialysis 1. Acidosis - you produce organic acids that can't be cleared 2. Hypocalcaemia - no activation of VitD 3. Infection - uraemia prevents degranulation 4. Bleeding - prevents degranulation of platelets 5. Anaemia - no EPO 6. Hyperkalaemia - not clearing K+ 7. Pericarditis 8. Altered mental state |
|
|
What can you give for uraemia causing bleeding? |
Desmopressin - temporary increase in vWF and factor VIII |
|
|
What is the best drug to prevent renal injury?
|
ACEi This dilates the efferent arteriole - so reduces pressure in the glomeruli. Even though it causes a decrease in GFR initially, it reduces injury in the long term |
|
|
What is the rise in creatinine with total renal failure? Why is this important to know? |
45-90 umol/L So an an increase by 90 in a day, even if the total creatinine is relatively low (150) then it is still an indication of total renal failure |
|
|
What is the BUN:Creatinine ratio in pre-renal failure? What is the urine Na+? What is urine osm? |
20:1 This is because slow flow through the kidney allows more urea to be reaborbed Urine sodium is LOW - body is trying to retain as much salt as possible Uosm is HIGH - even though Na+ is reabsorbed, other things are concentrated (e.g. urea) |
|
|
What are the causes of post renal renal failure? (4 causes) |
1. Bladder cancer 2. Prostate hypertrophy or cancer 3. Bilateral obstruction/stricture 4. Bilateral ureteral disease - Retroperitoneal fibrosis (bleomycin, methotrexate) - Neurogenic bladder (most commonly - diabetes and MS) |
|
|
Treatment of post-renal renal failure |
Drain the bladder |
|
|
What are the cases of acute tubular necrosis? (5 points) |
Overall causes related to - decreased perfusion, direct injury, decreased drainage, or a combination 2. Allergens (allergic interstitial nephritis) 3. Pigments (e.g. RBC breakdown 4. Crystals (e.g. urate, oxylate) 5. Ca2+ |
|
|
What is the urine Osm in renal - renal failure? Why? What else would you find in urine |
Same as plasma because the tubular cells cannot concentrate or dilate the urine. You will also find casts (brown granular casts) and epithelial cells. |
|
|
What are the treatment principles of ATN? (3 points) What doesn't work to fix ATN (which medications you would think of intuitively) |
1. Correct underlying cause 2. Hydration 3. Supportive care Doesn't work: Diuretics Low dose dopamine |
|
|
What are the common medications associated with allergic interstitial nephritis? (5 points) 70% of all causes of allergic interstitial nephritis are caused by medications.
|
1. Penicillin 2. Cephalosporin 3. Sulfa drugs 4. Allopurinol 5. Rifampin 6. Quinolone |
|
|
Of all the causes of ATN, what are the features unique to allergic nephritis? (4 points) |
Rash Fever Eosinophilia Joint pain |
|
|
What is the best initial tests for suspected allergic nephritis? (3 points) Hint: One is specific, the other 2 are general to kidney injury |
Check for 1. Eosinophiurea - Urinanalysis 2. Haematurea 3. Proteinurea ( <2g/24 hours) Urinanalysis cannot distinguish between WBC and eosinophils. You need to specifically do Hansel's test |
|
|
What is the most accurate test for allergic nephritis? What is the treatment? |
1. Biopsy - however it is not necessary (even if most accurate) because of the clinical features of fever, rash, joint pain, and eosinophilia) Treatment: Stop offending agent +/- corticosteroids |
|
|
What are possible causes of pigmented related ATN? (2 points) |
1. Myoglobinuria (e.g. crush injuries, seizures) 2. Haemoglobinuria (ABO transfusion reaction) Note: A serious crush injury, kidney is not the main concern. You will die of hyperkalaemia. So check for K+ first Tx: Calcium chloride, calcium gluconate |
|
|
What is the best initial test for a person with crush injury and suspected ATN? |
1. Blood for K+. Need to protect the heart from arrhythmias, check ECG 2. Dipstick for blood (it can't tell the diff between haemoglobin, myoglobin, or RBCs) 3. Check to see if there are blood cells in urine. No blood cells but positive on dipstick = crush ATN |
|
|
What is the management for rhabdomyolysis? (3 points) |
Aim: Prevent precipitation of pigment in tubules through hydration and diuretics and bicarbonate 1. Hydrate 2. Mannitol 3. Bicarbonate All these decrease the contact time in the tubules |
|
|
Diagnosis of pigment related ATN? (suspected crush injury) |
1. Blood K+ and ECG --> check heart first. Tx with IV calcium chloride or IV calcium gluconate (only if ECG changes). Aggressive rehydration + manitol 2. Not life threatening - urinalysis, no blood but + on dipstick 3. Confirm test with serum CPK - 10,000-100,000 (normal <500) Other findings: metabolic acidosis, decreased serum Bicarb, hyperphosphate |
|
|
Protein associated ATN, what is the main causes? Does it cause a nephritic or nephrotic syndrome? |
Multiple myeloma It causes a nephritic syndrome - the light chains cause inflammation! |
|
|
Crystal related ATN When should you suspect it? |
Typical features of ATN Increased Cr Uosm similar to blood (350) May see sediment Suspect it in a patient trying to commit suicide with ethylene glycol (anti-freeze) |
|
|
What are the possible causes of crystal related ATN? (3 causes) |
1. Ethylene glycol (oxylate crystals) 2. Methanol - also causes blindness 3. Metabolic anion gap acidosis |
|
|
What do you see on urinalysis for crystal related ATN? |
Envelop shaped crystals |
|
|
What is the treatment for crystal ATN? (2 points) |
1. IV fomepizole (antidote for methanol or ethylene glycol overdose) 2. Dialysis (in severe) |
|
|
Why does Crohn's disease cause oxylate crystals? |
Crohn's causes a fat malabsorption. Calcium binds to fat to form soap. Calcium also binds to oxalate. So more fat in GI displaces oxalate which is then absorbed. Normally Calcium-oxalate is excreted in faeces. So results in a chronic hyperoxaluria |
|
|
What is the aetiology of urate crystals causing ATN? How can this be prevented? |
1. Tumour lysis syndrome (most common). The lysis of tumour through chemotherapy releases lots of purines and pyrimidines. Esp leukaemia and lymphoma All chemo patients should have vigorous hydration and allopurinol. Urinanalysis to check/diagnose |
|
|
What effect does hypercalcaemia have on the kidneys? (3 points) |
1. Stones 2. Distal tubular necrosis 3. Nephrogenic diabetes incipitus Most common cause is primary parathyroidism |
|
|
Define renal tubular acidosis |
Systemic acidosis caused by renal impairment of the ability to maintain acid base balance |
|
|
Which type of RTA is most common? What are its features? |
Type 4 "Hyporeninaemia hypoaldosteronism"
|
|
|
Which part of the nephron is type I RTA? What is the kidney unable to secrete |
Distal tubule Inability to secrete H+ |
|
|
What part of the nephron is affected in type 2 RTA? What is the kidney unable to do? |
Proximal tubule It is the area where sodium bicarb is reabsorbed. Inability to reabsorb bicarbonate results in 1. systemic acidosis 2. Hypokalaemia 3. Urine pH >5.5 4. Bicarb in urine Other findings 1. Glycosouria 2. Amino--aciduria |
|
|
What is the treatment for type 2 RTA? (1 point) |
Sodium bicarbonate (massive doses may be required Type 2 RTA - proximal tubular failure of reabsorption of bicarb leading to systemic acidosis |
|
|
What is the treatment for Type 1 RTA? (3 points) |
Type 1 RTA - Distal tubule unable to secrete H+ Tx with 1. Sodium bicarb 2. Potassium supplements 3. Citrate |
|
|
How is the diagnosis of type 2 RTA made? (2 general tests and 1 specific test) |
General signs of RTA: 1. Plasma HCO3- <21mmol/L 2. Urine pH >5.3 Specific tests 1. Acid load test - give 100 mg/kg ammonium chloride by mouth, check urine pH hourly and plasma HCO3- If urine pH remains >5.3 despite plasma HCO3- of 21 mmol/L then confirmed Type 1 RTA |
|
|
What are the aetiologies for Type 2 RTA? (proximal disease, loss of HCO3-) 9 points |
1. Vit D deficiency, secondary hyperparathyroid, chronic hypocalcemia 2. Chronic hepatitis 3. Autoimmune 4. Wilson's 5. Amyloid 6. Fanconi's 7. Acetazolamide (used in intracranial hypertension, glaucoma, cystinuria) 8. Heavy metals 9. Myeloma |
|
|
Why do you not get stones in type 2 RTA? (proximal tubule leak of HCO3) |
Initially the urine is basic as HCO3 is lost but once enough HCO3 is lost the urine becomes more acidic so stones don't form |
|
|
What are the causes of type 2 RTA? 3 points (I won't list rare causes) |
Wilson's disease Glycogen storage disease (type 1) Multiple myeloma |
|
|
Which type of RTA causes HYPERkalaemia? |
Type 4 Hypoaldosteronism Hyporeninism |
|
|
Can RTA cause an anion gap acidosis? What are the two conditions that cause a non-anion gap acidosis |
The intuitive answer is YES but that is INCORRECT All RTAs cause elevated Chloride which results in normal anion gap. NON ANION GAP ACIDOSIS 1. RTA's 2. Diarrhoeas
|
|
|
What is the treatment for type 4 RTA? |
Because it is a disease of Hypoaldosterone Hyporenin Tx is Fludrocortisone!!! Give them a FUDGING mineralocorticoid |
|
|
What type of RTA does a person have with? 1. Stones 2. High K+ 3. No stones |
1. Type 1 - Distal tubule. Cant SECRETE H+ so urine is BASIC. Basic urine forms stones 2. Type 4 - Hypoaldos, hyporenin - no aldos = can't secrete K+ so Hyperkalaemia 3. Type 2 - Proximal, initially basic urine but when HCO3 runs out, there is still enough H+ to prevent stone formation. NOTE: TYPE 2 (PROXIMAL) disease is RARE as FUDGE |
|
|
How is type 4 RTA diagnosed? 4 points Treatment? |
1. Hyperkalaemia 2. Low plasma bicarbonate and hyperchloraemia 3. Normal ACTH stimulation test 4. Low basal 24 hour urinary aldosterone Subnormal response to plasma renin and plasma aldosterone stimulation Tx Fludrocortisone 0.1mg daily |
|
|
What are the 3 main causes of Hypervolaemic hypernatraemia? |
Anything which causes the brain to believe there is IV volume depletion CHF (weak heart, low pressure) Cirrhosis (low oncotic pressure, loss of intravascular volume) Nephrosis (loss of oncotic pressure) |
|
|
A bipolar patient on lithium. What electrolyte balance issue is he likely to have? What else can it cause to the kidney? How could you differentiate? |
Psychogenic polydipsia - usually low plasma Na+ Nephrogenic diabetes incipitus - Usually plasma Na+ HIGH Nocturnal polyuria is +++ Nephronic DI |
|
|
Aetiology of organic causes of SIADH? (not drugs) |
CNS disease (stroke) Pulmonary disease Neoplastic disease |
|
|
What drugs can cause SIADH? Hint: 2 antidepressant categories 4 antipsychotics |
SSRIs TCA Haloperidol Cyclophosphamide Vincristine Carbamazepine Memory tool: 2 antidepressants, and 4 antipsychotics |
|
|
How do you diagnose SIADH? |
1. Increased Urine Osm and Sodium (osm >100 is suggestive) 2. Confirm with plasma ADH level |
|
|
Treatment of SIADH? 3 points |
1. Water restriction (esp for psychogenic, may be the only treatment used) 2. Demeclocycline 3. Lithium --> causes nephrogenic DI |
|
|
What will you see if you give desmopressin to someone with nephrogenic DI? What is the treatment for NDI |
Nothing. Kidney isn't responding to ADH Diuretics and NSAIDs |
|
|
What electrolyte disturbances CAUSE nephrogenic DI? |
HypoKalaemia HYPER Ca2+ These patients present with MASSIVE dehydration. Main treatment for hyper Ca2+ is HYDRATION!!!! |
|
|
What factors (non-GI loss) cause a Hypokalaemia? 5 points |
1. Insulin - this is taken into cells in conjunction with K+ so causes serum K+ to go down 2. Alkalosis - there is a H+/K+ exchanger on most cells. So if there is systemic alkalosis then body cells will release H+ and take in more serum K+ causing a systemic hypokalaemia 3. B12 and Folate replacement - rapid replacement will cause a rapid production of tissues (opposite of lysis syndromes) 4. CUSHING's Syndrome/Conn's syndrome 5. Beta AGONISTS |
|
|
What factors cause a hyperkalaemia? 5 points |
1. Low insulin 2. Acidosis - cells will not secrete out H+ (and therefore for take in K+) resulting in increasing serum K+ 3. Any lysis syndrome - Tumour lysis syndrome, haemolysis, rhabdomyolysis 4. Addison's Syndrome - Any cause of hypoaldosterone. Includes adrenal insufficiency, adrenalectomy 5. Blockade of 2Na/3K ATPase - DIGOXIN and B-blockers |
|
|
What is the clinical presentation of hypokalaemia? 3 points Hint: Muscle, heart, kidney |
Muscle weakness Cardiac - arrhythmias (flattened T and U waves) Nephrogenic DI |
|
|
What are the ECG changes in Hyperkalaemia? What is the treatment |
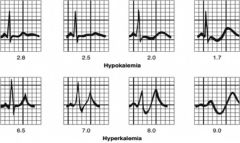
1. Peaked T wave 2. Short QT 3. As it gets more severe (>6.5) then loss of P waves 4. >7.5 - widened QRS Tx: Calcium chloride |
|
|
What is the treatment for hypokalaemia? |
1. Correct underlying cause 2. Replenish K+, oral or IV |
|
|
What is the maximum dose of oral K+ to treat hypokalaemia? What is the max IV rate? |
There is no maximum because GI intake is limited Dextrose increases GI intake of K+ Max IV rate is 10-20 mmol/hour or risk arrhythmia |
|
|
How much K+ do you need to replenish a single point drop in K+? |
4-5 mmol / kg to increase K+ mmol/L by one point I.e. 70kg person will need ~350 mmol to correct hypokalaemia from 2.5mmol/L to 3.5mmol/L |
|
|
Why is dextrose IV contraindicated in Hypokalaemia? |
Dextrose increases insulin which drives K+ intracellularly and causes even more severe hypokalaemia |
|
|
What electrolyte disturbance would you suspect in a person who has come in with a history of adrenectomy for a previous adenoma? |
Hyperkalaemia They will have hypoaldosteronism and so will not be able to remove K+ from body |
|
|
What is the treatment of hyperkalaemia of 6.5mmol/L? |
Calcium gluconate Calcium chloride |
|
|
What are the indications for administration of calcium gluconate? What does calcium gluconate do physiologically? |
1. Hyperkalaemia 2. Hypocalcaemia 3. Magnesium toxicity Calcium gluconate/chloride PROTECT THE HEART. Does not directly lower the K+ levels |
|
|
Why do patients with glomerulonephritis present sooner than those with tubular interstitial disease? |
It has nothing to do with the severity of the disease. Symptoms of brown urine and oedema will cause the patients to present sooner. In tubular interstitial disease, the symptoms of azotemia/uraemia will take longer to develop |
|
|
What should you suspect if you see red cells, haematuria, red cell casts, protein? |
Always suspect glomerulonephritis until proven otherwise. 24 hour urine required to distinguish between nephrotic vs nephritic Renal biopsy required for diagnosis |
|
|
During the workup of a suspected patient with glomerulonephritis, you should check for which of the following: Renal tests - UEC, urinanalysis, etc Systemic symptoms Complement levels Immunoglobulin levels |
Check renal, systemic (many causes are systemic diseases), and complement So after determining whether its a renal only disease or a systemic disease. Check complement level
Diseases can be divided up into low or normal levels of complement. Especially C3 |
|
|
A patient presents with chronic sinusitis and progressive renal failure. UA shows microhaematuria Anaemia of chronic disease (normocytic) ESR is elevated What is the most likely diagnosis? What is the best initial test? What is the treatment? |
1. Granulomatosis with polyangiitis 2. c-ANCA + 3. Treated with steroids and cyclophosphamide |
|
|
Patient presents with signs of GPA (chronic sinusitis, unresponsive to treatment, with rash). Patient also has asthma What is the most likely diagnosis? What is the best initial test? What definitive test is required? What is the treatment? |
1. Churg-Strauss 2. p-ANCA 3. Renal biopsy showing eosinophilia 4. Steroids and cyclophosphomide |
|
|
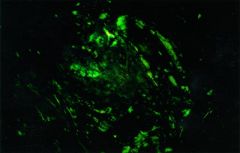
Patient presents with chronic cough streaked with blood, haemoptysis, there are no skin or GI symptoms. Urinanalysis shows microhaematuria What is the most likely diagnosis? What is the best initial test? What is the definitive test? What is the treatment? HINT: LUNG AND RENAL SYMPTOMS |
Goodpasture's syndrome anti-GBM levels Lung or renal biopsy - immunoflures Plasmapheresis + steroids and cyclophos |
|
|
30 yo with hepB, postprandial abdo pain, fatigue, LOW, livedo reticularis. No lung symptoms Labs show: Signs of inflammation: Raised CRP, ESR What is the most likely diagnosis? What is the best diagnostic test? What is the treatment Hint: Multisystem disease, younger patient, postprandial pain, with no lung symptoms associated with HepB |
Polyarteritis nodosa Biopsy (usually sural nerve) - usually not needed Tx with steroids and cyclophos |
|
|
Which two diseases are characterised by the triad of: 1. Haemolytic anaemia 2. Thrombocytopenia 3. Uraemia (raised urea/BUN) 2 points |
1. Thrombotic thrombocytic purpura - think about this in HIV patients 2. Haemolytic uraemic syndrome - always consider this in children with recent E. coli infections (0157:E7) |
|
|
HIV patient with fever, altered mental status, uraemia, thrombocytopenia, haemolytic anaemia. FBE shows low platelets and anaemia Smear shows schistocytes UA shows microhaematuria What is the most likely diagnosis? Hint: HIV + multisystem + triad of haemolytic anaemia/thrombocytopenia/uraemia. |
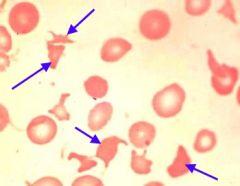
1. TTP Schistocytes are the result of erythrocytic membrane damage caused by sheering of red blood cells as they pass through a fibrin mesh of clot formation occurring in the blood vessels Difference from HUS - HIV patient, and also has fever and altered mental state |
|
|
Why is giving antibiotics or platelets contraindicated in TTP or HUS? |
HUS may be caused by E. coli (0157:E7) and ABs will make it worse The disease process in TTP is destruction of RBCs as they are damaged as they pass by the fibrin clots. So giving platelets will cause more clotting and more damage to passing RBCs Tx is supportive and monitoring |
|
|
Patient with longstanding diabetes and hypertension presents with microhaematuria and proteinuria What is the most likely diagnosis? What is the treatment? |
Diabetic nephropathy Strict glycaemic control + lifestyle + diet ACEi |
|
|
What is the most common cause of nephrotic syndrome in adults? Usually present with oedema UA shows >3.5g protein They usually also have hypercholesterolaemia, hypertension, and systemic disease |
Membranous glomerulonephropathy Treat with ACEi/ARBs Can add diuretics Low salt diet Self limiting disease. Will resolve |
|
|
A patient with malignant disease presents with progressive renal failure. Patient has macroglossia A renal biopsy was performed and with Congo Red stain showed Apple Green Birefingence What is the most likely diagnosis? What is the treatment? |
Buzzwords: Significant systemic disease - can be malignancy or inflammatory condition (IBD), congo-red stain Amyloidosis Tx - control underlying disease |
|
|
Young child with deafness and renal disease (UA shows microhaematuria) |
Buzzwords: Young, ear and renal problems Alport syndrome |
|
|
Renal disease with systemic symptoms of: joint pain, purpuric papules. Patient has hepatitis This should make you think of vasculitides. Besides UA to check renal manifestation. Next step is to measure complement level. This patient shows LOW complement What is the most likely diagnosis? What is the main DDx |
Cryoglobulinaemia Main DDx Henoch-Schonlein purpura Make diagnosis with serum cryoglobulins |
|
|
25yo female with malar rash, fever, joint pain. Labs show - ACD, increase CRP/ESR, ANA+, confirmed with anti-dsDNA/anti-Sm Abnormal UA/raised Cr with the above features suggests the need for renal biopsy Why is biopsy required? What is the treatment? |
Dx: Lupus nephritis Biopsy needed to see if it is sclerosis or proliferative nephritis No treatment for sclerosis Steroids/mycophenolate for proliferative |
|
|
Patient presents with mild to gross haematuria and hypertension. History reveals that he has had an URTI 1-2 days ago. What is the most likely diagnosis? Is a renal biopsy required? What is the treatment? Nephrotic or nephritic picture common? How does it differ from PIGN? |
1. IgA nephropathy
2. Yes, need to confirm as half these patients will go on to have ESRD 3. ARBs/ACEi to control hypertension, monitor renal function 4. Nephritic 5. PIGN occurs 2-4 weeks after |
|
|
Young patient presents with multiple red-violet purpura, fever, and abdominal pain. Prior to this they had headache and nausea. UA shows microhaematuria, RBC casts, some protein What is the most likely diagnosis? What other similar condition presents with abdo pain? What is the treatment? |
1. Henoch-Schonlein purpura 2. Polyarteritis nodosa 3. Supportive, it resolves spontaneously |
|
|
An otherwise healthy child presents with facial puffiness, generalised oedema, and fatigue. UA shows nephrotic range proteinuria. Need 24 hour collection What is the most likely diagnosis? Is a renal biopsy required? What is the treatment? |
1. Minimal change disease (buzz: child, nephrotic syndrome) 2. Yes need to confirm with electron microscopy which shows fusion of foot processes 3. Steroids (usually 6 weeks of prednisone) |
|
|
Patient with rapidly progressing renal failure with no discernible cause. Renal biopsy shows crescents What is the most likely diagnosis? What will an ANCA test show? What is the treatment? |
Idiopathic rapidly progressing glomerulonephritis - it is a diagnosis of exclusion ANCA negative Treatment - steroids, cyclophosphamide |
|
|
35yo with coca-cola/tea coloured urine, some oedema, had an untreated infection a few weeks ago that spontaneously resolved (most likely group A strep) What is the best initial test? Is a renal biopsy required? What is the treatment? |
1. Anti-streptolysin O titre will be high 2. No, based on history and ASO 3. Usually supportive. Amoxycillin or azithromycin if allergic to penicillins |
|
|
Buzzword question Nephrotic picture + history of either Hepatitis, Lupus/significant systemic disease, cryoglobulinemia UA shows microhaem, proteinurea (nephrotic range), and LOW complement Diagnosis? Management? |
Membranoproliferative glomerulonephritis Tx Dipyridamole or aspirin Check for secondary causes (HepB/C, ANA, cryoglobulins) |
|
|
Buzzword question Nephrotic syndrome HIV Black person Present with oedema and hypertension UA - Broad, waxy, casts What is the most likely diagnosis? What is the treatment? |
Focal segmental glomerulonephritis Tx: ACEi/ARB Diuretics if significant oedema Check for secondary causes: 1. HIV / CD4 count 2. Lupus |
|
|
What is the significance of the following findings in UA? 1. Hyaline 2. Dysmorphic red cells 3. Broad waxy casts 4. Granular 5. White cells |
1. Hyaline - everyone produces protein but if you're pre-renal then you don't wash it away as there is low perfusion so you get hyaline casts 2. Glomerulonephritis - change shape as they squeeze out 3. Chronic renal failure 4. Also known as dirty/muddy. Associated with ATN, these are epithelial cells 5. Pyelonephritis, interstitial nephritis |
|
|
What are granular casts in UA? What are they made of? |
These are also called dirty/muddy casts Made of epithelial cells |
|
|
Why is measuring protein in urine in isolation not useful? What is a better test besides 24 hour urine? |
Protein excretion varies throughout the day so protein at a certain point of measurement can vary A spot Albumin to creatinine ratio is a better test to account for the daily variation. ACR can be as useful as a 24 hour urine collection |
|
|
Define end stage renal disease |
Renal disease that require dialysis to live |
|
|
What are some examples of phosphate binders? Who are they used for? |
Calcium carbonate Used for those with chronic kidney disease |
|
|
Of the following complications of CKD which ones can be corrected without dialysis and which require dialysis? High phosphate, anaemia, vitD deficiency, low Ca2+, pericarditis, hyperkalaemia, encephalopathy, acidosis |
Phosphate binders, EPO for anaemia, VitD and Ca2+ Dialysis REQUIRED FOR 1. Severe hyperkalaemia 2. Pericarditis 3. Encephalopathy 4. Severe acidosis |
|
|
What are the most common causes of CKD? 4 points |
Most common - diabetes Others Glomerulonephritis Cystic disease Interstitial nephritis |
|
|
What are the indications for dialysis? 5 points |
1. Fluid overload - diuretics won't work because kidneys have failed 2. Severe acidosis 3. Pericarditis - die of arrhythmias and tamponade 4. Encephalopathy and severe neurologic impairment 5. Severe hyperkalaemia |
|
|
What is Cinacalcet? |
It is a calcium-memetic. It goes to the parathyroid gland and turns off PTH secretion by making the parathyroid gland think Ca2+ plasma levels are high |
|
|
What is the most common form of kidney stone? What factors will increase stone formation (of this type)? |
Calcium oxalate - 70% Increased calcium Decreased oxalate dietary intake (without oxalate to bind calcium in the GI tract, more Ca in blood) Crohn's disease |
|
|
Who gets Mg/Aluminium/phosphate stones? |
Infections!! Klebseila, Proteus infections |
|
|
What is unique about uric acid stones in terms of imaging? |
Radiolucent! |
|
|
What types of stones are associated with fat malabsorption (pancreatic insufficiency)? |
Oxalate crystals Increased FFA in GI tract binds with Ca2+. This allows more free oxalate to be absorbed. Normally oxalate or citrate binds with Ca2+ and is excreted but with increased absorption of oxalate this leads to oxalate crystals |
|
|
What shape are oxalate crystals in urine analysis? |
Enveloped shaped This is also seen in suicide attempts with ethylene glycol (this also causes an anion gap metabolic acidosis). Treat this with IV ethanol or fomepizole |
|
|
What are the GOLDMARK aetiologies for anion gap metabolic acidosis? |
G — glycols (ethylene glycol & propylene glycol) O — oxoproline, a metabolite of paracetamol L — L-lactate, the chemical responsible for lactic acidosis D — D-lactate M — methanol A — aspirin R — renal failure K — ketoacidosis, ketones generated from starvation, alcohol, and diabetic ketoacidosis |
|
|
What is the main cause of nephrotic syndrome in adults? What are the most common other (primary causes)? 1 + 3 points |
Membranous GN Other primary GNs presenting as nephrotic syndrome are: 1. Minimal change 2. FSGS 3. Membranoproliferative GN |
|
|
An obese women aged 20-40 with nephrotic syndrome? What type of GN does she likely have? |
Most common cause of adult nephrotic GN is membranous GN however... FSGS is strongly associated with obesity. It is also known as Obesity-Related Glomerulopathy (ORG). If the question specifically states obesity then select FSGS |
|
|
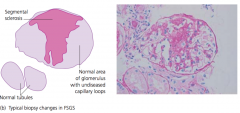
What is the typical histopath changes seen in FSGS? Answer is a picture but be able to describe it |
|
|
|
What are 3 secondary causes of nephrotic syndrome GNs? |
1. SLE - check ANA, anti-dsDNA, C3/C4 levels 2. Plasma cell dyscrasias 3. Infections with Hep B, C, HIV |