![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
131 Cards in this Set
- Front
- Back
|
What are the prokaryote paramycoses? |
Actinomyces Actinomadure Dermatophilus Streptomyces Nocardia |
|
|
What are the eukaryote paramycoses? |
Prototheca (algae) Chlorella (algae) Rhinosporidium "Mesomycetozoae" Pythium "Oomycete Straminipila" (looks like a fungus but genes indicate plant) |
|
|
All actinomycetes "bacteria" appear Gram ___ |
positive |
|
|
What are the human and animal species of actinomyces? |
actinomyces israelii = human actinomyces bovis = animal |
|
|
What are the species of Nocardia and what do they infect? |
Nocardia asteroides Nocardia brasiliensis Nocardia cavie All infect human and animals |
|
|
Describe the general appearance of mycobacterium |
Mostly rod shaped but may branch |
|
|
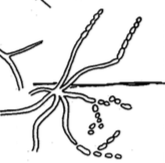
Describe the appearance of dermatophilus |

cocci in chains that form filaments produce motile zoospores in water |
|
|
Describe the appearance of geodermatophilus |
saprophytic (small, about 1micro in diameter) |
|
|
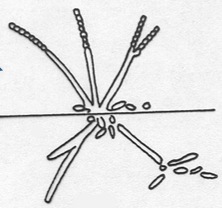
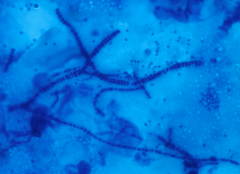
Describe the appearance of nocardia |
In culture, diphtheroid fragments and filaments. Aerial mycelium with spore units |
|
|
Describe the appearance of rodococcus |
rods animal and human pathogen |
|
|
appearance of Saccharopolyspora |
saprophytic
|
|
|
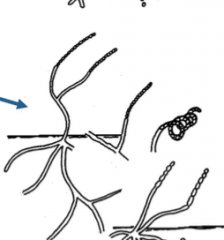
appearance of Actinomadura |
Short chains of spores in culture. also fragments forming rods and cocci like cells |
|
|
Appearance of Nocardiopsis |

saprophytic |
|
|
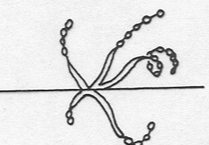
appearance of streptomyces |
extensive aerial mycelium. abundant spores, normal branches and coiled branches |
|
|
appearance of Nocardioides |
saprophytic |
|
|
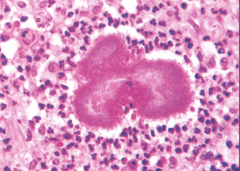
What clinical symptoms are normally associated with actinomycosis? |
-chronic granulomatous infection -sinus tracts discharging purulent material with small compact masses termed "grains" |
|
|
What are the etiologies for actinomycosis (and 3 species found in hosts)? |
-Actinomyces israelii -Actinomyces bovis in host = A. Odontolyticus, A. naeslundi, A. viscosus |
|
|
State some facts about actinomycosis |
-ANAEROBIC -normal flora in human and animals -often will see it disseminate in the face -Common trauma includes tooth extraction -they love bones |
|
|
Describe the general laboratory procedure to diagnose actinomycosis? |
-Pus, biopsy, aspirates -10% KOH Culture in thioglycolate broth (grows in the lower part of the tube because it is ANAEROBIC), blood agar + anaerobiosis -histopathology |
|
|
What is the treatment for actinomycosis? |
antibiotics |
|
|
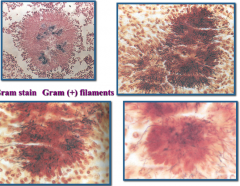
appearance of actinomycosis gram stain? |
|
|
|
What two diseases does Nocardia cause? |
-Nocardiosis -Actinomycetoma -both of these look identical clinically, so need to culture |
|
|
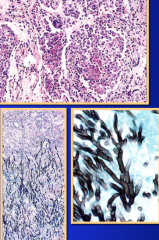
Describe the symptoms of nocardiosis and actinomycetoma |
-Nocardiosis = acute or chronic infection involving the lungs or other organs. Looks like tuberculosis or lung cancer (on x-ray and losing weight). Branched filaments in infected tissue with no grains -Actinomycetoma = chronic subcutaneous infection with sinus tracts containing grains of different colors depend on etiologic agent. Formation of tumoral-like masses with grains |
|
|
Describe how Nocardiosis and Actinomycetomas are acquired |
-Nocardiosis = inhalation of nocardia elements -actinomycetoma = trauma to the skin so that nocardia elements can enter |
|
|
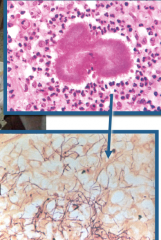
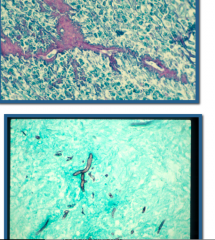
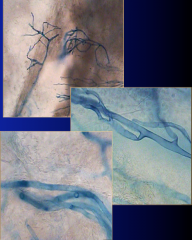
Describe how you would diagnose nocardiosis in the laboratory |
-samples: sputum and biopsy -tests: Gram stain and partial acid fast stain (THIS IS PARTIAL ACID FAST) -for the biopsy, use modified ziehl-neelsen culture, Lowenstein-jensen with blood agar (should produce yellow colony) |
|
|
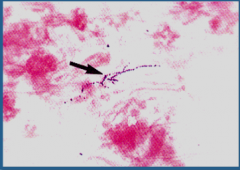
gram stain results for nocardiosis |
|
|
acid fast stain results for nocardiosis |
|
|
modified ziehl nielson biopsy reslts for nocardiosis |
|
|
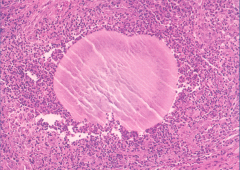
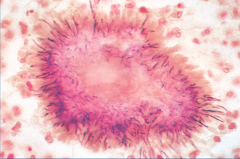
What is the main clinical feature of actinomycetomas? |
the formation of tumoral-like masses with “grains” |
|
|
What are the etiological agents of actinomycetomas? |
actinoadurae madurae actinomadurae pelletieri streptomyces somaliensis nocardia brasiliensis nocardia cavaie nocardia asteroides |
|
|
Actinomycetomas love to infect ____ |
bones |
|
|
Describe how you would diagnose an actinomycetoma in the laboratory |
samples: pus and biopsytests: 10% KOH, partial acid fast stain should see hard nodules and small gram positive filaments |
|
|
Streptomyces somaliensis |
|
|
Actinomadura madurae |
|
|
Actinomadura pelletieri |
|
|
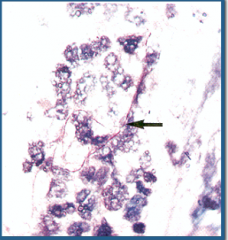
Nocardia brasiliensis H&E |
|
|
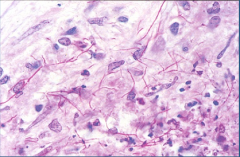
Nocardia brasiliensis gram stain |
|
|
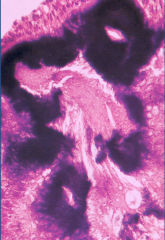
What are the clinical symptoms of dermatophilosis? |
-scales and crust skin formation -pustular and exudative skin infection -HIGHLY CONTAGIOUS -normally seen around water or wet areas |
|
|
Describe how you would diagnose dermatophilosis in the laboratory |
-samples: skin scrapings -tests: gram and giema stain -culture (Haalstra method) |
|
|
Haalstra method of staining dermatiphilosis |
|
|
Describe the clinical symptoms for chlorella and prototheca |
erythematous plagues in the skin, common in immunocompromised |
|
|
What are the etiologies for prototheca and chlorella? |
-prototheca wickerhamii -prototheca zopfii -chlorella protothecoides known as the "aquatic fungi" |
|
|
What is the main virulence factor for prototheca and chlorella? |
1 cell makes thousands (!!) |
|
|
How does prototheca and chlorella cause infection? |
trauma to the skin and exposure to humidity and soil |
|
|
What is one of the difficulties with treating prototheca and chlorella infections? |
antiobiotics and antifungal drugs do not work well |
|
|
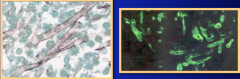
Describe how you would diagnose prototheca and chlorella in the lab |
-samples: biopsy -tests: histopathology (should see spherules, almost look like sclerotic bodies) -culture: in Sabouraud, tube culture (waxy green colonies) |
|
|
spherules seen in protheca and chlorella |
|
|
Describe the clinical symptoms of rhinosporidiosis |
-polyps in mucous membranes (eyes, nose, vagina) -polyps are soft and they easily bleed -CANNOT BE CULTURED -approximately 450micro in diameter -belongs to mesomycetazoae -only the nuclei multiply |
|
|
Describe the clinical symptoms of pythosis |
-blood vessel diseaese -subcutaneous and systemic infections -huge inflammatory response that can go to bones = disseminated -normally IMMUNOCOMPROMISED |
|
|
How is pythosis normally acquired? |
-wet environments -zoospores -aquatic fungi -in animals and humans -oomycetes |
|
|
How does the pythosis organism spread? |
bud breaks off of hyphae and grows a flagellum |
|
|
What is the normal treatment of pythosis? |
antibiotics, surgery |
|
|
How would you diagnose pythosis in the laboratory? |
-sample: biopsy -serology: immunodiffusion, ELISA, immunoperoxidase, Western blot -Histopathology ( almost look like "worms" in tissue) -Culture (flagellated organism) |
|
|
Pythosis |
|
|
List 4 pathogenic fungi described in class |
1.coccidioisis 2. blastomycosis 3. paracoccidioisis 4. histoplasmosis |
|
|
Where is blastomycosis usually found? |
East of the Mississippi river, normally only in the United States |
|
|
How does blastomyces infect the host? |
1. conidia breaks off of hyphae and goes into lungs 2. in lungs, hyphae --> yeast form that is more difficult for macrophages to ingest 3. the quantity of cells infecting the host is related to how "infected" they are |
|
|
What are some clinical symptoms of blastomycosis? |
- weight loss -tired all of the time -small spot on skin if it has disseminated (normally this is when it is recognized) -will see fever -X-ray looks like TB or Nocardia -alveolar consolidation -lymphadenopathies -cough chest pain |
|
|
80% of blastomycosis cases are diagnosed by the ____ |
dermatologist |
|
|
Who normally gets blastomycosis? |
middle age men and pregnant women |
|
|
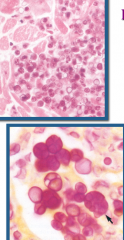
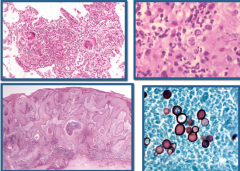
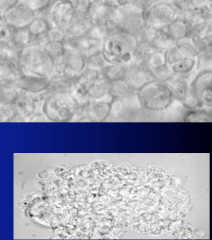
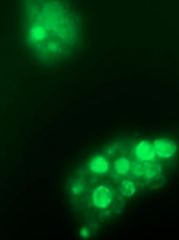
Describe how you diagnose blastomycosis in the laboratory |
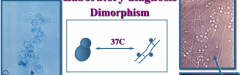
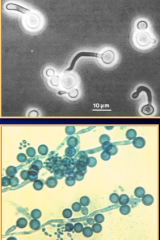
-samples: sputum, biopsy, scrapings, serum -serology: immunodiffusion, fluorescence assay, ELISA -histopathology: H&E, silver (yeast cells will look black), gram stain -wet mount: 10% KOH, silver or gram stain (most reliable) -Culture: sabouraud, mycosel (use DNA probes) -LOOK FOR BUDDING YEAST WITH WIDE NECK -LOOK FOR DIMORPHISM |
|
|
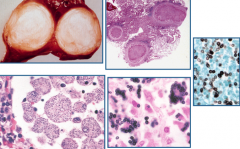
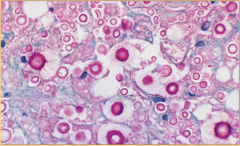
typical findings w/ blastomycosis |
The presence of single budding yeast cells with neutrophils epithelioid cells few giant cells and macrophages. Necrosis and fibrosis is typical |
|
|
pseudoepitheliomatous hyperplasia |
|
|
dimorphism w/ blastomycosis |
|
|
What are the treatments for blastomycosis? |
-Amphotericin B is the best (but toxic to eukaryotic cells) -Itraconazole -successful, some relapse -ketaconazole has partial success in immunecompromised patients |
|
|
What the other names for blastomycosis? |
Gilchrist's disease North America blastomycosis |
|
|
What are the common names for coccidioisis? |
valley fever posada's disease |
|
|
Where is coccidioimycosis normally found? |
in desert in North America and South America (spores can be carried on the wind!) |
|
|
What are the symptoms for coccidiomycosis? |
-upper respiratory infection that normally resolves itself -rarely fatal -can disseminate to bones, CNS, skin, -MOST OFTEN PULMONARY, RARELY CUTANEOUS |
|
|
In what form of conidia is coccidioimycosis spread? |
arthrospores |
|
|
What are the symptoms for coccidiomycosis? |
-cavities inside lungs -progressive or benign chronic pulmonary symptoms -immune system of individuals becomes overwhelmed and immune system becomes anergic -inflammatory response (granulamatous, purulent, arthrospores turn into spherules with endospores) |
|
|
Pathology of coccidiomycosis? |
3 types of inflammatory rxn: purulent,granulomatous, and a combination of both. In the lung tissues the arthrospores -->spherules with endospores cellular rxn is observed around the spherules (usually a granuloma) |
|
|
acute cocciodiodal pneumonia |
|
|
Describe how you would diagnose coccidioimycosis in the laboratory |
-samples: serum, sputum, biopsy -serology: ID, LA, ELISA10% KOH (spheres inside alveoli) -Culture the biopsy in tubes (DO NOT TOUCH), use DNA probes to identify -Look for dimorphism |
|

|
dimorphism of coccidiomycosis |
|
|
What are the available treatments for coccidioimycosis? |
-amphotericin B -fluconazole -itraconazole -ketoconazole -miconazole |
|
|
What are the common names for histoplasmosis? |
darling's disease reticuloendoteliosis = infection of organs with large immune cell count (liver, spleen, lymph nodes, bone marrow) |
|
|
Where is histoplasmosis normally found? |
-soil -bat guano -chicken houses -Argentina and around the Mississippi river in the US |
|
|
True or False: histoplasmosis affects healthy people as well as immunocompromised people |
True (animals are very susceptible to it because they are sniffing the ground) |
|
|
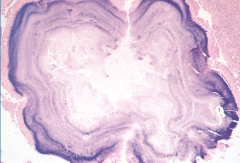
Describe the symptoms for acute, chronic disseminated, progressive disseminated histo. |
-acute = in children, high fever, nausea, vomiting, moving on to cough and dyspnea, neutropenia, thrombocytopenia, hepatomegaly, splenomegaly, lymphoadenopathychronic -disseminated = usually healthy individuals, fever, weight loss, fatigue -progressive disseminated = immunocompromised, hepatomegaly, fever, lung involvement |
|

|
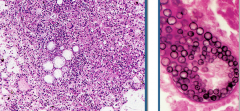
Fibrocaseous nodulewith concentric layers found in histoplasmosis |
|
|
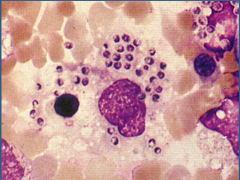
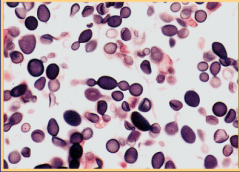
histoplasmosis |
|
|
How would you diagnose histoplasmosis in the laboratory? |
-samples: sputum, biopsy, serum -Serology: ID, H&M, FA, antigen detection -Giemsa stain the sputum (cells inside macrophage DO NOT have kinetoplast like Leishmania) -Culture: use DNA probes, mciro and macrocondida (look for dimorphism) |
|
|
giemsa stain of histoplasmosis |
|
|
What treatment options are available for histoplasmosis? |
-acute = amphotericin B, itraconazole -chronic = amphotericin B, itraconazole, ketaconazole -progressive = amphotericin B, itraconazole for AIDS patients |
|
|
What are common names for paracoccidioidomycosis? |
South America Blastomycosis Lutz-Splendore-Almeida’s Disease |
|
|
paracoccidioidomycosis is: |
Chronic, progressive granulomatous infection that disseminated to the skin, mucous membranes, lymph nodes, GI, and other organs. The disease is primary pulmonary |
|
|
clinical features of paracoccidioidomycosis |
Generalized dissemination. Adolescent and immunocompromised patients. Progressive and culminant |
|
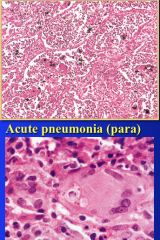
image only |
. |
|
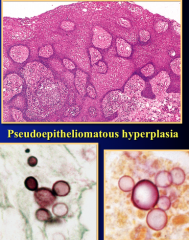
image only |
. |
|
|
How would you diagnose paracoccidioidomycosis in the laboratory? |
-samples: serum, sputum (10%KOH), biopsy -Serology: ID, ELISA, FA -Culture |
|
|
What treatment options are available for paracoccidioidomycosis? |
amphotercin B to prevent relapse: ketoconazole and itraconazole |
|

|
paracoccidioidomycosis sputum in 10% KOH |
|
|
Common names for cryptococcosis |
Busse-Buschke’s disease |
|
|
cryptococcosis is: |
chronic, sub-acute,pulmonary, systemicinfection. predilection for theCNS causing meningitis. -immunocompromised =YEAST WITH CAPSULE |
|
|
pulmonary cryptococcosis |
Low fever, cough,weight loss. CanDisseminated toother organs initial treatment = amphotericin B, fluc and itran to avoid relapse |
|

|
pulmonary cryptococcosis in KOH |
|

what is this? in what media? |
cryptococcosis in the spinal fluid - india ink most common initial treatment = amphotericin B, fluc and itran to avoid relapse |
|
|
Cutaneous and mucocutaneous cryptococcosis |
Upon dissemination = Papules, pustules,and abscesses withulcers. initial treatment = amphotericin B, fluc and itran to avoid relapse |
|
what is this? in what media? |
Cryptococcal pneumonitis in Mayer’s mucicarmin |
|
what is this? in what media?
|
Cryptococcal skin lesion in Silver |
|
|
How would you diagnose cryptococcosis in the laboratory? |
10% KOH india ink serology - Ag detection on capsule FA DNA probes and cultures |
|
|
Common names for candididasis? |
Moniliasis, thrush, yeast infection |
|
|
Candidiasis is ? |
opportunistic immuncompromisd can disseminate normal flora cutaneous and mucocutaneous |
|
what is this? |
candida |
|
|
mucocutaneous candidiasis treatment |
imidazole cream, itraconazole, ketoconazole systemic = amphotericin B |
|
|
C. parapsilosis causes |
oncomycosis endocarditis otitis endopthalmitis arthritis peritonitis |
|
|
C. tropicalis causes |
vaginitis intestinal infections pulmonary infections systemic infections |
|
|
C guilliermondii causes |
endocarditis cutaneous infections oncomycosis |
|
|
C krusei |
endocarditis vaginitis |
|
|
C zeylanoides causes |
oncomycosis
|
|
|
Trichosporan Beigelii |
white piedra |
|
|
Geotrichum candidum |
disseminated infections in acute leukemia pts |
|
|
Aspergillosis is: |
Infection of the lungs with dissemination to other organs. restricted to severely immunocompromised patients. Healthy individuals seemto be resistant to the infection. It is one of the increasing cause of nosocomial infection |
|
|
Common aspergillus etiologies |
Aspergillus fumigatus Aspergillus flavus Aspergillus niger |
|
|
How do you get infected w/ Aspergillus |
Worldwide, every where filamentous opportunistic fungi. Not dimorphic lungs --> hyphae |
|
|
Laboratory detection of Aspergillus |
culture, serology, DNA probes |
|
|
Aspergillosis |
|
|
Aspergillosis treatment |
Amphotericin B liposomal formulation (most diagnosed post mortem, has poor prognosis otherwise) |
|
|
Entomophthoramycota Systemic Mucormycosis is? |
- Acute infection of the respiratory tract --> thrombosis -infectious agent = Spores -defective phagocytic cells are unable to control the infection. -immunocompromised |
|
|
common causes of Entomophthoramycota Systemic Mucormycosis |
Rhizopus Absidia Mucor Saksenaea |
|
|
Entomophthoramycota Systemic Mucormycosis risk factors |
Diabetes, corticosteroid therapy, granulocytopenia |
|
|
Entomophthoramycota Systemic Mucormycosis |
|
|
dx of Entomophthoramycota Systemic Mucormycosis |
Serology ELISA ID usually post mortem poor prognosis treatment = amphotericin b |
|
|
Entomophthoramycota Systemic Mucormycosis |
|
|
Pneumocystis jiroveciiPneumocystis pneumonia (PCP) |
-can’t be isolated in pure culture. -Opportunistic -immunocompromissed hosts |
|
|
PCP clinical symptoms |
-Dyspnea, nonproductive cough,night sweats, fever, rare hemoptysis. children usually Involves cyanosis, mild Cough without fever |
|
|
Dx of PCP |
wet mount, FA, EM, silver stain, giemsa stain sputum or bronchoalveolar lavage |
|

|
EM of PCP |
|
|
wet mount of pcp |
|
|
FA of PCP |