![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
47 Cards in this Set
- Front
- Back
|
What are the two components of anxiety? |
|
|
What is this? |
Mood |
|
What type of disorders? |
Anxiety disorders |
|
What are all these? |
Major anxiety disorders |
|
|
Recurrent panic attacks, occurring at over at least one month, involving anticipatory anxiety (the fear of having an attack) and avoidance of situations where panic is likely to occur or help is unavailable.
Which disorder? |
Panic disorder |
|
|
Palpitations, sweating, pounding heart, trembling, shaking, dyspnea, feeling smothered, etc. You've had one so you know the symptoms. |
Panic attack (at least four must develop abruptly and reach a peak within 10 minutes) |
|
|
Between what ages do panic attacks occur? Can they be chronic and relapsing? What is the prevalence and male to female ratio? |
Early teens => 40s Chronic, relapsing 1-3% community, 3-8% primary care Female to male = 2:1 |
|
|
What is fear (or panic), often with blushing, of anticipated humiliation or rejection by others in social situations. While the person desires social activities and relationships, the dread of embarrassment leads to avoidance. |
Social anxiety disorder (social phobia) |
|
|
Which disorder is bimodal in onset (age 5 or early adolescence), chronic but may remit with positive social experiences?
It has a prevalence of 3-4% but performance anxiety is more common and a female to male ratio of 3:2 where more males seek treatment? |
Social anxiety disorder (social phobia) |
|
|
Familial modeling Being bullied Humiliation as a form of discipline Disfiguring lesions (visible burns or deformities)
What are all of these? |
Developmental experiences contributing to social phobia/avoidant personality disorder |
|
|
What are phobias characterized by fear responses to specific cues?
When should they be treated? |
Simple phobia Treated only if they interfere with important activities |
|
|
What condition should you be mindful of if patient needs MRI?
What is the response some have to situations that involve blood, needles, and injury? |
|
|
|
Simple phobias:
Onset:
Animals? Blood? Situations? May remit with experience
Prevalence? Which is more common in males? |
Animals = 7 Blood = 9 Situations = 2-7 and early 20s
Prevalence = 11% (most common anxiety disorder) Blood, injury, injection phobias more common in males |
|
Diagnosis? |
Agoraphobia |
|
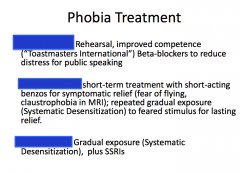
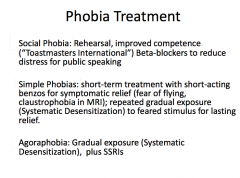
Identify what is being treated. |
|
|
|
Persistant (>6 months) pattern of uncontrollable worries about health, safety, access to resources, and threats to other people. Multiple signs of arousal and autonomic dysfunction.
What is the disease? Onset? Female:male? |
Generalized anxiety disorder Onset = Mid teens to mid 20s (may occur after onset of chronic illness) Duration > 6 months
Prevalance 5% (female:male 2:1) |
|
|
Characterized by intrusive, arousal, and avoidance symptoms. Onset males 6-15, females 20-29 (also post partum) Gradual onset, 5% episodic, 15% severely deteriorate, waxes and wanes with stress Prevalence 2%, males >females Adults (males = females) |
Obsessive-compulsive disorder |
|
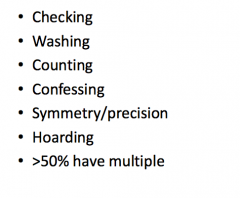
What are all of these? |
Common compulsions |
|
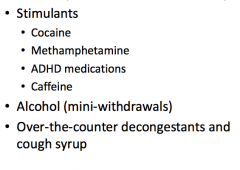
What can all of these cause? |
Substance/Medication-Induced Anxiety disorder
Panic attacks predominate |
|
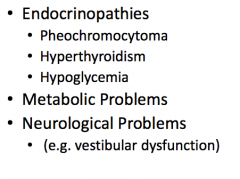
What can all of these medical conditions cause? |
Anxiety disorder |
|
|
|
|
What type of disorder? |
Mood disorder |
|
|
|
|
|
What does SIG-E-CAPS stand for? |
Sleep, loss of interest, guilt, energy, concentration difficulty, appetite disturbance, psychomotor retardation/agitation, suicidal thoughts
FIVE REQUIRED FOR A MAJOR DEPRESSIVE EPISODE |
|
|
Is bereavement abnormal? Can it turn into major depression? How is it treated? |
|
|
What does this describe? |
|
|
|
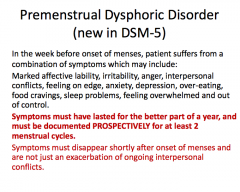
Marked affective lability, irritability, anger, interpersonal conflicts, feeling on edge, anxiety, depression, over-eating, food cravings, sleep problems, feeling overwhelmed and out of control. All of this in the week before onset of menses.
Symptoms must last for most of year and be documents PROSPECTIVELY for at least 2 menstrual cycles. They must also disappear shortly after menses.
Diagnosis? |
|
|
Diagnosis? |
Cyclothymic disorder |
|
|
|
|
Bipolar 1 or 2? |
Bipolar 1 |
|
Bipolar 1 or 2? |
Bipolar 2 |
|
|
Overeating, oversleeping while depressed, preserved reactivity to reward. Which mood features? |
Atypical features |
|
|
Detachment from the environment while awake; negativism including immobility, mutism, refusal to eat or drink. May be life threatening. |
Catatonic features |
|
|
Dense anhedonia, lack of response to reward, terminal insomnia (early morning awakening), diurnal variation (morning worse).
|
Melancholic features |
|
|
Depressive episode within one month of childbirth by definition. Clinically this period of markedly increased risk may be >3 months. Often includes marked anxiety. |
Postpartum onset |
|
|
Marked congruent in depression: delusions of poverty, guilt, nihilism, illness, self-disgust; derogatory auditory hallucinations.
Mood congruent in mania: delusions of special powers or unlimited resources, paranoia, auditory hallucinations. |
Psychotic features |
|
|
Review table 47.1 |
Review table 47.1 |
|
|
Identify structure involved:
Short term memory
Cognitive inefficiency, recollection bias (depressed people cannot access happy memory; mania makes sad memory inaccessible) |
Hippocampus |
|
|
Identify structure involved:
Individual nuclei are part of three distinct circuits that link cortical areas with sensory cortices and subcortical structures. These regulate emotion, motivation, arousal, and attention.
Erratic arousal, subjective distress, compromised attention/concentration Loss of pleasure responses to sensation in depression Sometimes associated with hypersensitivity to sensory input in mania |
Thalamus |
|
|
Identify structure involved:
Conscious thought, executive functions (selection among alternatives, anticipation, inhibition of impulses, sequencing)
Helplessness, indecisiveness, hopelessness, distorted sense of time (slowed in depression, accelerated in mania) |
Dorsolateral prefrontal cortex |
|
|
Identify structure involved:
Assess risk in pursuit of reward, relate new information to context (memory and environment)
Overestimation of risk and reduced reward in depression; underestimation of risk in mania |
Orbitofrontal cortex |
|
|
Identify structure involved:
Integration of emotion and cognition
Abnormal motivation (apathy in depression) Dysregulation or arousal |
Anterior cingulate gyrus |
|
|
Identify structure involved:
Fear, rage, selective attention
Anxiety, irritability, vigilance, hypersensitivity to negative environmental cues |
Amygdala |
|
|
Identify structure involved:
Reward
Lack of pleasure (depression), decreased or increased motivation |
Nucleus accumbens |
|
|
Identify structure involved:
Sleep, appetite, sexual behavior, metabolic rate, adaptation to acute or chronic environmental or social stress
Insomnia/hypersomnia, lack of or increased sexual interest, hyperphagia or anorexia |
HPA axis |
|
|
|
|
|
|