![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
128 Cards in this Set
- Front
- Back
|
Name the sensory tracts in the spinal cord. |
Dorsal column medial lemniscus system Gracile (LL) and Cuneate (UL) tracts |
|
|
Somatic spinal pathway? |
Lateral and anterior corticospinal tracts
White matter |
|
|
What are the extrapyramidal tracts in the spinal cord? |
Rubrospinal Reticulospinal Olivospinal Vestibulospinal |
|
|
Spinal cord pain pathway? |
Spinothalamic tracts - lateral and anterior |
|
|
Which of the following is incorrect regarding the CNS? 1. There are 100 billion neurons 2. Microglia as the scavenger cells - i.e. macrophages 3. Macroglia include oligodendrocytes, schwann cells and astrocytes 4. Astrocytes form the BBB and support neurons 5. Myelin is produced by oligodendrocytes solely |
5. Myelin is produced by oligodendrocytes solely - Incorrect Also produced by schwann cells in the Peripheral NS |
|

Name the parts of a neuron |

|
|
|
What are the different types of neurons? |
Unipolar (invertebrate neuron) Bipolar (Retina) Pseudo unipolar (Ganglion of dorsal root) Multipolar (motor neuron, parking of cerebellum) |
|
|
What happens to a neuron if it is cut? |
Wallerian degeneration |
|
|
Orthograde vs retrograde transport in an axon? |
Orthograde - down the axon away from the cell body via kinesin Retrograde - away from the cell body - via dynein - i.e. Nerve growth factor and some viruses (VZV, HSV) |
|
|
Regarding neurons which of the following is incorrect: 1. Action potential propagation is a passive process 2. The 3Na/2K ATPase pump maintains the resting membrane potential 3. Resting membrane potential is -70mV 4. The membrane is more permeable to K than Na 5. Decreasing the ECF Na concentration reduces the size of the AP but has little effect on resting membrane potential |
1. Action potential propagation is a passive process - INCORRECT - Active, self-propagating process, poor conductance |
|
|
What is required for a potential difference to exist? |
1. Unequal distribution of ions of one or more species across a membrane 2. The membrane must be permeable to one of more ions - via channels or pores @ Equilibrium the concentration forces = electrical force |
|
|
Describe the events in the development of an Action potential. |
1. Stimulus 2. Some voltage gated Na channels open --> membrane potential becomes less negative --> THRESHOLD POTENTIAL ~-55mV 3. VGNa Channels open rapidly --> massive influx of Na+ 4. Depolarisation of the cell in positive feedback fashion until membrane potential ~+30mV 5. NA influx slows as electrical forces change direction and K channels open 6. VGNa channels enter inactivated state 7. K efflux repolarises the cell in a slower manner 8. K channels slow to close --> hyper polarisation |
|
|
True / False? Hyperkalemia (ECF) moves the resting potential closer to the threshold for eliciting an AP and thus the neutron becomes more excitable Hypokalemia moves the resting potential closer to the threshold for eliciting an AP and thus the neutron becomes more excitable |
TRUE for HYPERKALAEMIA - hyper excitable Hypokaelaemia - the membrane potential is reduced and the neuron is hyper polarised i.e. when the K+ level is greater outside the cell the concentration gradient for K to move out is less pushing the resting membrane potential less negative |
|
|
What is the relative refractory period/absolute refractory period? |
Absolute - No AP possible - No VGNa channels in resting state Relative - Some channels still in inactivated state and are unable to be opened --> requires supernormal stimulus for AP |
|
|
What is the effect of Ca2+ levels on membranes and APs |
Hypercalcaemia --> increases membrane stability Hypocalacemia --> Hyperexcitable membrane |
|
|
Which of the following are correct/incorrect regarding nerves? 1. APs occur in an all-or-none fashion 2. Threshold potential is -55mV 3. The fastest nerve fibres are the C type fibres 4. Saltatory conduction involves the jumping of depolarisation from one node of Ranvier to the next 5. The smallest nerves are the C type fibres |
The fastest nerve fibres are the C type fibres - Incorrect A - alpha fiber > A-beta > other A > B > C |
|
|
What are the different types of A fibre nerves? |
Alpha - proprioception, somatic MOTOR Beta - touch, pressure Gamma - Motor to muscle spindles Delta - pain/temp |
|
|
What are the different types of nerve fiber? |
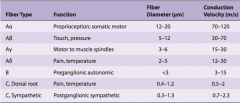
A, B, C |
|
|
Order the nerve fibre types by thickness. |
Thickest ----> Thinest alpha > beta > gamma > delta > B > C Same order for speed fast --> slow |
|
|
Which fibres are most sensitive to: hypoxia pressure Local aesthetics? |
Hypoxia B > A > C --> Autonomic Pressure A > B > C --> Motor / sensory LA C > B > A --> Autonomic / Pain |
|
|
Which of the following statements about glia is true? 1. Microglia arise from macrophages outside of the nervoussystem and are physiologically and embryologically similarto other neural cell types. 2. Glia do not undergo proliferation. 3. Protoplasmic astrocytes produce substances that are tropic to neurons to help maintain the appropriate concentrationof ions and neurotransmitters by taking up K+ and theneurotransmitters glutamate and GABA. 4. Oligodendrocytes and Schwann cells are involved in myelinformation around axons in the peripheral and centralnervous systems, respectively. 5. Macroglia are scavenger cells that resemble tissuemacrophages and remove debris resulting from injury,infection, and disease. |
Protoplasmic astrocytes produce substances that are tropic to neurons to help maintain the appropriate concentration of ions and neurotransmitters by taking up K+ and the neurotransmitters glutamate and GABA. |
|
|
A 13-year-old girl was being seen by her physician becauseof experiencing frequent episodes of red, painful, warmextremities. She was diagnosed with primary erythromelalgia,which may be due to a peripheral nerve sodium channelopathy.Which part of a neuron has the highest concentration of Na+channels per square micrometer of cell membrane? 1. dendrites 2. cell body near dendrites 3. initial segment 4. axonal membrane under myelin 5. node of Ranvier |
node of Ranvier |
|
|
Which one of the following nerves hasthe slowest conduction velocity? A. Aα fibers B. Aβfibers C. Aγ fibers D. B fibers E. C fibers |
E. C fibers |
|
|
Which of the following is not correctly paired? A. Synaptic transmission: Antidromic conduction B. Molecular motors: Dynein and kinesin C. Fast axonal transport: ~400 mm/day D. Slow axonal transport: 0.5–10 mm/day E. Nerve growth factor: Retrograde transport |
A. Synaptic transmission: Antidromic conduction |
|
|
Which of the following ionicchanges is correctly matched with a component of the actionpotential? 1. Opening of voltage-gated K+ channels: After-hyperpolarization 2. A decrease in extracellular Ca2+:Repolarization 3. Opening of voltage-gated Na+ channels: Depolarization 4. Rapid closure of voltage-gated Na+ channels: Resting membrane potential 5. Rapid closure of voltage-gated K+ channels: Relative refractory period |
3. Opening of voltage-gated Na+ channels: Depolarization |
|
|
Which of the following is incorrect (multiple) regarding muscle: 1. Striated muscle include skeletal and cardiac 2. Cardiac muscle acts as a functional syncytial unit 3. Skeletal mm has pacemaker capabilities 4. Smooth muscle has 2 types - unitary or multiunit 5. The type of SM found in hollow viscera acts like a multi unit with pacemakers that discharge regularly 6. Multiunit SM is found in the eye and has no pacemaker function |
3. Skeletal mm has pacemaker capabilities - incorrect - it is the only type that DOES NOT have this function 5. The type of SM found in hollow viscera acts like a multi unit with pacemakers that discharge regularly - Incorrect - Hollow viscera is unitary with pacemakers that discharge irregularly |
|
|
Which of the following is incorrect (multiple) regarding SKELETAL muscle: 1. Sarcolemma is the cell membrane of a muscle cell 2. On microscopy the region between two Z lines is a sarcomere 3. Thick filaments are made up of actin, tropomycin, troponin and thin filaments of myosin 4. Muscle end in tendons |
3. Thick filaments are made up of actin, tropomycin, troponin and thin filaments of myosin Other way around --> THIN filaments are made up of actin, tropomycin, troponin and THICK filaments of myosin |
|
|
What are the main contractile elements of Skeletal muscle? |
Myosin II Actin Tropomyosin Troponin - three components I, T, C |
|
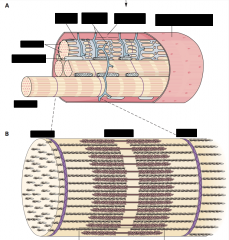
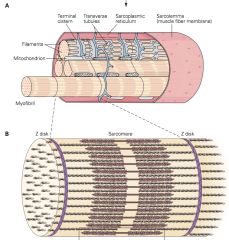
Name the components of skeletal muscle: |
|
|
|
Function of the T System? Location? |
System of transverse tubules which is continuous with the sarcolemma and hence contains ECF. It allows for rapid transmission of the AP to all myofibrils. In close connection to the sarcoplasmic reticulum at the terminal cisterns of the SR which is an important source of Ca for muscle contraction Location: A-I junction |
|
|
Function of Dystrophin ? |
Large protein - rod Connects actin filaments to the transmembrane protein beta-dystroglycan and provides scaffolding for the fibrils |
|
|
Equilibrium potential for Na K |
Na +65mV K -95mV |
|
|
Resting membrane potential for Skeletal muscle? Cardiac Muscle? |
Skeletal -90mV Cardiac -80mV |
|
|
Length of AP in Skeletal muscle? Compared to cardiac? |
2-4ms - but very short contraction period vs cardiac Cardiac - 2ms but PROLONGED plateau and depolarisation 200ms |
|
|
Which of the following is Incorrect regarding SKELETAL Muscle? 1. Fast muscle fibres are involved in strong gross sustained movements and have a twitch duration of 7.5ms 2. Slow muscle fibres are concerned with strong gross sustained movements and have a twitch duration of 100 ms 3. There is a 2ms delay from AP to contraction |
Fast muscle fibres are involved in strong gross sustained movements and have a twitch duration of 7.5ms - incorrect FAST fibers --> fine, rapid precise movements |
|
|
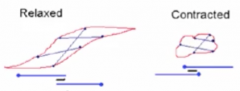
What happens on a molecular level during muscle contraction? |
AP via T system --> Ca2+ influx from SR Ca binding to Troponin C --> weakening the interaction of Troponin I with the actin binding site Binding of myosin (one) head to actin Release of ADP from myosin head on binding and movement at the junction of the head/neck - POWERSTROKE (due to stored energy in head cocked position from ATP hydrolysis) Head remains attached whilst the other head now attaches and has the power stroke - once attached the first head releases ATP binds and is hydrolysed and the head cocked ready for the next beat (repeats as long as Ca2+ present) |
|
|
Function of the dihydropyridine receptor? Ryanodine receptor? in skeletal and cardiac muscle |
dihydropyridine receptor - voltage gated Ca2+ channels - AP activates this channel allowing Ca efflux from the SR in SKELETAL muscle via a physical interaction with the ryanodine receptor on the SR In cardiac muscle the dihydropyridine receptor causes Ca influx from the ECF which then activates the ryanodine receptor |
|
|
Which of the following are incorrect/correct? 1. Isometric contractions involve a length decrease 2. Isotonic contraction is against a constant load 3. Contraction and relaxation are both energy dependent events 4. SERCA is a ATP dependent Ca pump on the SR to remove Ca2+ from the cytosol |
1. Isometric contractions involve a length decrease - incorrect - no length change in ISOMETRIC (SAME LENGTH) 2. Isotonic contraction is against a constant load - true - Same tension but decrease in length 3. Contraction and relaxation are both energy dependent events (SERCA on relaxation) 4. SERCA is a ATP dependent Ca pump on the SR to remove Ca2+ from the cytosol |
|
|
What is Summation of Contractions? What is the result of this? |
Multiple APs arrive prior to relaxation (contractile units do NOT have a refractory period) This results in tetanic contraction Frequency of the AP required depends on the twitch duration |
|
|
Mutation in the Ryanodine receptor can result in what condition? |
Malignant hyperthemia with certain anaesthetics or in rare cases exposure to high environmental heat or strenuous exercise |
|
|
At what muscle length can the maximal tension develop and the maximal velocity of contraction occur? |
Resting length Shorter muscle - less distance to move Longer - less overlap between actin and myosin |
|
|
What are the 3 types of muscle fibres? Characteristics? |
Slow I - Oxidative - Red Fast IIA - Oxidative - Glycolytic - Red Fast IIB - Glycolytic - WHITE - Fatiguable |
|
|
Besides ATP what is another energy source for contraction? |
Phosphorylcreatine |
|
|
During light exercise what is the main macro source of energy? This changes to what during increasing intensity exercise? |
Lipids - free fatty acids Carbohydrates for more intense exercise - glucose / glycogen |
|
|
How much anaerobic energy production is required for : 100m sprint 20min run 60min race |
100m (10sec) sprint - 85% 20min run - 20% 60min race - 5% |
|
|
What is a motor unit? |
The motor neuron and all the muscle fibres it innervates. All muscle fibres must be of the SAME type Recruitment occurs in an ordered fashion - S (slow) fibres then FR (fast red) then FF (fast) - recruitment is asynchronous |
|
|
Describe the features of cardiac muscle that are different from skeletal muscle? |
Function syncytia Intercalated discs at Z lines Each myofibril - enclosed by membrane Gap junctions for AP propagation |
|
|
Describe the Action potential in a cardiac muscle cell. |
Phase 0 - Voltage gated Na channels open - rapid depolarisation + Overshoot Phase 1 - Initial rapid repolarisation - due to closure of Na channels and opening of K channels Phase 2 - Prolonged plateau opening Ca2+ voltage gated channels (L type) - INFLUX Phase 3 - Final/ late rapid depolarisation of the membrane due to closure of Ca channels and a delayed increase in K efflux Phase 4 - Resting membrane potential |
|
|
Tetany can occur in cardiac cells. T/F? |
False due to the prolonged absolute refractory period and relatively long AP |
|
|
Long QT syndrome is most commonly due to? |
Mutations in the voltage gated K channel 90% |
|
|
MOA of catecholamines on the heart? |
increase in cAMP which activated protein kinase A Which phosphorylates voltage gated Ca channels causing them to stay open longer |
|
|
In smooth muscle what does activation of calmodulin dependent myosin light chain kinase do? |
phosphorylation of myosin which allows for increased myosin ATPase activity and binding of myosin to actin |
|
|
ACh vs adrenalin effect on SM ? |
ACH - contraction via phospholipase C --> IP3 --> Ca influx Adrenalin - relaxation |
|
|
The contractile response in skeletal muscle: A. starts after the action potential is over. B. does not last as long as the action potential. C. produces more tension when the muscle contracts isometrically than when the muscle contracts isotonically. D. produces more work when the muscle contracts isometrically than when the muscle contracts isotonically. E. decreases in magnitude with repeated stimulation. |
C. produces more tension when the muscle contracts isometrically than when the muscle contracts isotonically. D - No work done if no change in length |
|
|
What are the 3 types of synaptic vesicles? |
There are three kinds of synaptic vesicles:small, clear synaptic vesicles that contain acetylcholine, gly-cine, GABA, or glutamate; small vesicles with a dense corethat contain catecholamines; and large vesicles with a densecore that contain neuropeptides. |
|
|
Which proteins are involved in the fusion-exocytosis complex? |
Vesicle - V-snare - synaptobrevin Membrane - T-snare - syntaxin interaction inhibited by toxins from clostridium tetani and clostridium botulinum |
|
|
Baclofen MOA? |
GABA b agonist Presynaptic inhibition via g protein coupled reaction resulting in increased K conductance used for spasticity |
|
|
Function of GABA a receptor? |
Increases Cl- conductance Inhibitory |
|
|
What is a Renshall cell? |
Inhibitory interneuron affecting spinal motor neurons Glycine is the Neurotransmitter |
|
|
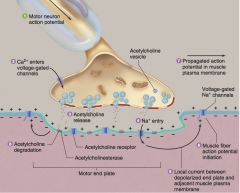
Describe the events at the NMJ |
|
|
|
T/F - Acetylcholinesterase is presentin high concentration at the neuromuscular junction |
TRUE |
|
|
Name the different types of nociceptors. |
Mechanical nociceptors respond to strong pressure (eg, froma sharp object). Thermal nociceptors are activated by skintemperatures above 42°C or by severe cold. Chemically sensitive nociceptors respond to various chemicals like bradykinin,histamine, high acidity, and environmental irritants. Polymodal nociceptors respond to combinations of these stimuli. |
|
|
Types of Pain fibres? Neurotransmitters? |
Thinly myelinated A delta (fast) - glutamate Unmyelinated C (slow) - glutamate + substance P - dull intense pain |
|
|
allodynia? |
is a sensation of pain in response to a normallyinnocuous stimulus |
|
|
Substances that can activate or sensitise nociceptors? |
Histamine, bradykinin, serotonin, prostaglandin, K+ |
|
|
Afferent fibers from visceral structures reach the CNS via? |
sympathetic and parasympathetic nerves including CNs |
|
|
Name the tracts in the spinal cord that carry: Pain/temp Touch Proprioception |
Pain/temp - Lateral spinothalamic tract --> Touch/Proprioception - Dorsal column to Medial lemniscal tract to the thalamus --> postcentral gyrus |
|
|
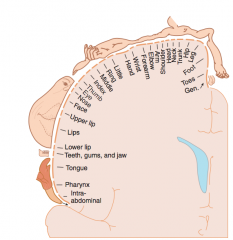
Describe Somatotopic organisation in the post central gyrus |
|
|
|
Pain signals activate which parts of the brain? |
Primary and secondary somatosensory cortex Cingulate gyrus amygdala frontal lobe insular cortex |
|
|
Describe the monosynaptic stretch reflex |
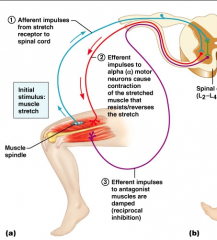
Ie muscle spindle receptor or golgi tendon organ Rapid reflex |
|
|
Describe the single twitch, tetanus and the Treppe effect |
Single twitch - Single AP i.e. at 1hz Tetanus - high frequency AP resulting in no relaxation period, maintaining maximal voluntary contraction (MVC) Treppe - means the increase in peak force as twitches are repeated at a high frequency (i.e. not enough time for all the Ca to be removed thus increased force) |
|
|
Describe muscle Fatigue |
REDUCED FORCE or SHORTEN velocity with repeat near maximal contractions at short intervals Fatigue is present in fast muscle but absent or small in slow muscleand cardiac muscle. The latter have high oxidative capacity capable of producingthe ATP needed for each contraction. In fast muscle phosphocreatine (PCr) is broken down and glycolysis acceleratedso that phosphate and creatine and lactate and protons (lactic acid) accumulate. Accumulation of phosphate appears to be one important cause of fatigue. Lactic acid accumulation appears to be unimportant• Fatigue is also associated with reduced Ca release |
|
|
How can the cortex increase force produced by skeletal muscle? |
Increase frequency of firing Increase the number and size of motor units recruited |
|
|
Describe the structure of SM |
Long, thin, spindle, fusiform cells Connected by gap junctions Actin + myosin but not organised (no striations) - allowing for greater fractional shortening --> they attach to the membrane by dense bodies |
|
|
Define Latch State and its functional role in SM |
Latch State --> Specialised function of SM that allows contraction to be maintained for long periods with minimal energy consumption - Ca and energy consumption decline but force is preserved - Remain in attached/latched state (Do not cycle) - (in isometric Skeletal muscle contraction cross bridge cycles and ATP is consumed) |
|
|
Describe the innervation and excitation of SM |
Supply: SNS (NA) or PSNS (ACh) mainly but some voluntary and enteric NT: many ; released from axon varicosities - no specific synaptic region Receptors - usually G protein coupled --> depolarisation --> opening of voltage gated Ca channels --> Ca influx --> contraction |
|
|
Indicate the intracellular pathway by which contraction is activated in SM |
Ca influx --> binds to Calmodulin which activates (dephosphorylation) myosin light chain kinase MLCK phosphorylates MLC to it's phosphorylated/active form --> Myosin and actin for XBs Slow excitation-contraction coupling due to slow diffusion of Ca and enzymatic processes are slow. Relaxation is partly dependent on endogenous phosphatases |
|
|
How does NO/cGMP/phosphodiesterase inhibitors affect contraction in SM? |
Nitrates/NO activate Guanylate cyclase --> Increases cGMP --> activates Protein Kinase A --> Inactivates MLCK and prevents activation of MLC --> hence relaxation Phosphodiesterase inhibitors block the breakdown of cGMP |
|
|
Describe the characteristics of the BBB |
Capillary - Not leaky like elsewhere (tight junction) - anatomical block Exchange is through the cell only - physiological restriction Lipid soluble molecules easily pass through Surrounded by astrocytes Barrier between the blood and CNS |
|
|
Identify sources of energy utilised in the brain. |
GLUCOSE (90%) - via GLUT 1 tranport (not insulin dependent) |
|
|
Describe the effect of hypoxia, hypoglycaemia and temperature on the brain |
Hypoglycaemia --> Mood change, trembling, sweating, blurred vision, headaches, dizziness, hungry, tiredness --> 2 minutes to unconsciousness Hypoxia --> 10 sec to unconsciousness, cortex most sensitive Temperature --> Hypothermia - reduces cerebral 02 consumption --> EEG isoelectric @ 20C Hyperthermia - Increased o2 consumption - over 42C enzymatic function disrupted |
|
|
Function of astrocytes? |
1. Induce endothelium to have tight junctions 2. Produce substances which affect which carrier proteins are present in the endothelium 3. Participate in the cross cellular transport i.e. K+ |
|
|
Function of BBB? |
Provide constant environment for the CNS - i.e. electrolytes Protect brain from endogenous and exogenous toxins in the blood Prevention of the escape of NTs into the general circulation |
|
|
What happens to the BBB near infection or tumours? Other things that affect it? |
Infection - Breakdown Tumours - rapid angioneogenesis without surround astrocytes Hypertonic fluid, +++ HTN, newborns (immature BBB) |
|
|
What are the circumventricular organs? Function? |
Posterior pituitary (endocrine) Median eminence of the hypothalamus Area postrema (Vomiting) Organum vasculosum of the lamina terminalis - OVLT (osmolarity - Vasopressin) Subfornical organ - SFO Here the capillaries have fenestrations with increased permeability Function as chemoreceptor zones |
|
|
Which of the following are incorrect/correct regarding the CNS: 1.The main source of energy for the brain is FFA 2. The brain uses 20% of the the body's 02 as rest 3. The cortex is the most sensitive part of the brain to hypoxia 4. Cerebral glucose utilisation is insulin dependent 5. Cerebral 02 consumption is 49ml/min |
1.The main source of energy for the brain is FFA - incorrect (Glucose) 4. Cerebral glucose utilisation is insulin dependent - Incorrect (insulin independent |
|
|
How does the brain remove ammonia? |
Glutamate + Ammonia --> Glutamine --> removal from CNS |
|
|
Describe the physiology of sleep |
Sleep is an essential, readily reversible physiologicalstate characterised by unconsciousness, reduced muscletone, analgesia, amnesia, respiratory and autonomicdisturbances and dreaming 2 types REM (eye movements) + NREM (slow wave - deep) |
|
|
Describe the primary rhythms of the EEG |
EEG - Recording of spontaneous electrical activity of the brain Alpha - 7.5-13Hz - normal relaxed state, occipital Beta - >14 Hz - fast, symmetrically, frontal, alert, anxious, eyes open Theta - 3.5-7.5 - normal in children and sleep, not in adults Delta - <3 Hz, highest amplitude, normal in infants and sleep, NOT adults |
|
|
Describe EMG. |
Electromyography (EMG) is an electro-diagnostic technique used for evaluating andrecording the electrical activity produced byskeletal muscles. Electrodes measure electricity over a muscle |
|
|
Describe the characteristics of NREM sleep. |

4 stages 1. low voltage, mixed frequency pattern on EEG 2. Appearance of sleep spindles + K complexes 3. High amplitude delta rhythm 4. Slow wave sleep, synchronisation may be MSK movement but no eye movement |
|
|
Normal level of REM sleep in adult? |
25% 20% elderly 50% infants |
|
|
Clinical Uses of EEG? |
› Has value in localizing pathologic processes withinthe brain › Detecting seizure activity, monitoring seizureactivity. › Used in anesthesia to assess levels of sedation - entropy › Diagnosis of generalized encephalopathies of metabolic or infective origin › To prognosticate at times in coma |
|
|
Describe the factors that control ICP |
BRAIN TISSUE, CSF, CEREBRAL BLOOD 1. Increased volume of any of the components = increased pressure 2. CSF translocation or increased absorption (linear 10-30mmH2O - or drainage via EVD 3. Decrease interstitial H2O 4. Blood flow - affected by MAP, CO2, temp, O2, metabolic rate (all increase except O2) 5. Sedation 6. Coughing, straining - intermittent spikes in ICP 7. Intra-abodminal and intrathoracic pressure |
|
|
Define the monroe - kelpie doctrine |
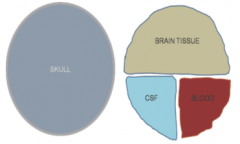
The CNS and its accompanying fluidsare enclosed in a rigidcontainer whose total volumetends to remain constant. Anincrease in volume of onecomponent (e.g., brain, blood,or cerebrospinal fluid) willelevate pressure anddecrease the volume of one ofthe other elements |
|
|
Identify factors that affect cerebral perfusion |
MAP CO2 (blunted by HTN) O2 Cerebral metabolism Temperature Cerebral flood flow - blood viscosity, medications (anaesthetics) |
|
|
Define auto regulation of CPP |
Auto regulation --> Ability of the cerebralcirculation to maintain cerebral blood flow (CBF) at arelatively constant level despite changes in cerebralperfusion pressure(CPP), by altering cerebrovascularresistance (CVR) |
|
|
Which of the following is incorrect/correct 1. A 100ml volume change in the skull always produces a equal predictable change in pressure 2. CCP = MAP - ICP 3. Cerebral blood flow ~ 54ml/100g/min 4. Brain wt 1400 grams 5. Normal ICP 5-15mmHg |
1. A 100ml volume change in the skull always produces a equal predictable change in pressure The volume change will cause different pressure changes depending on where the current ICP is on the P/V curve (high pressure - a small volume will cause a +++ increase in pressure) |
|
|
Result of raised ICP? |
Cushing Effect - ↑MAP with ↓HR & ↑RR Unconciousness ⟹ ↓CMRO2 (cerebral metabolic rateof O2) ↳ exhaustion of these ⟹ death via herniation |
|
|
Which of the following is correct/incorrect? 1. Autoregulation of CBF is limited to MAP between 50-150 2. Autoregulation is dependent on metabolic, myogenic (Stretch) and neurogenic (autonomic) mechanisms 3. Regarding cerebral blood flow - SNS causes vasoconstriction and PSNS cause vasodilation 4. ICP changes with coughing and straining are unimportant as the are non sustained 5. Temperature reduction causes a reduction in metabolic rate and reduces blood flow |
4. ICP changes with coughing and straining are unimportant as the are non sustained incorrect |
|
|
Function of CSF |
Buoyancy and cushioning for neural tissue Metabolic sink Electrolyte buffer Volume buffer (to SC) |
|
|
Production of CSF? Amount? |
Choroid plexus - 60% - plasma ultrafiltrate - active ionic transfer ventricular walls, perivascular cuffs, ependyma 90-150ml at anyone time ~550ml/day production |
|
|
Major differences between plasma and CSF? |
K ~ 2/3 Calcium 1/2 ~ 2.5 Glucose 2/3rds of plasma Protein --- Much much less |
|
|
CSF Circulation? |
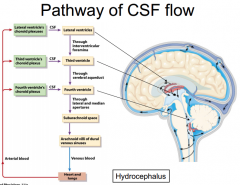
lateral ventricles - basal cisterns - over convex surface of the brain etc |
|
|
Removal of CSF? |
Arachnoid granulations projecting into venous sinuses- Active excretion process Across cribriform plate into cervical lymphatics Absorption is effectively zero for CSF pressure < 7 cm H20 and increases linearly with CSF pressure. Absorption and production balanced for CSF pressure11 cm H20 |
|
|
Describe the blood supply to the spinal cord. |
Paired Dorsal (Posterior) Spinal Arteries - Dorsal columns Single Ventral (Anterior) spinal artery Collaterals - Many for the dorsal. Limited to the Ventral. Ventral --> In the thoracolumbar area - limited collateral flow --> Artery of Adamkiewicz/great vertebral radicular artery (at risk for vascular insufficiency) |
|
|
Describe the regulation of spinal cord blood flow. |
Same as for CPP Spinal PP = MAP - Intraspinal pressure Intraspinal pressure is determined by CSF or venous pressure Autoregulation occurs at MAP 60-150 Affected by CO2 (20-80), Hypoxia (<60) |
|
|
Which of the following is correct/incorrect regarding the anatomy relevant to accessing the spinal neuraxis: 1. Conus Medullaris @ L 2-3 level 2. Local anaesthetics block nerve conduction at the level of the spinal roots 3. The contents of the epidural space includes fat and vertebral venous plexus, spinal nerve roots pass through it 4. Skin --> Sub cut tissue --> supra spinal ligament --> Interspinous ligament --> Ligamentum Flavum --> Epidural space --> dura --> subarachnoid space 5. Blockage of finer order = Autonomic > C and A delta > A alpha > A beta 6. Autonomic > Pain and temp > Touch > Motor |
1. Conus Medullaris @ L 2-3 level - incorrect (L1-2 ) 5. Blockage of finer order = Autonomic > C and A delta > A alpha > A beta - incorrect ( A beta > A alpha - last) |
|
|
Describe the physiological effects of neuraxial blockade. |
LA blockade at the level of the SPINAL ROOTS Blockade order - Autonomic > Pain and temp - C/A delta > Touch - A beta > Motor - A alpha Vasodilation below the level, decrease SVR/VR/CO Above T5 - (block SNS outflow to the heart) - bradycardia GIT peristalsis unopposed No direct effect on the lungs - except muscle weakness Apnoea, nausea, vomiting - due to poor cerebral flow + hypotension Urinary retention |
|
|
Describe the features of spinal shock. |
Acute SCI (e.g. transection)
Loss of descending activation in the vestibulospinal and reticulospinal tracts Immediate loss of sympathetic outflow and reflexes - Bradycardia - Profound hypotension Loss of bladder and colon reflexes Gradual recovery of segmental reflexes - Abnormal flexion response - babinski - Autonomic dysreflexia |
|
|
Describe the key features of somatosensory receptors and pathways. |
Tactile - Dorsal columns - discrimination, joint position, vibratory detection |
|
|
Describe processes of nociception |
All nociceptors are free nerve endings Aδ fibers (high threshold mechanoreceptors) - Fast, small, myelinated, secrete L-glutamate - Mechanical or thermal stimuli C fibers (polymodal nociceptors) - Slow, small, unmyelinated , secrete L-glutamate andsubstance P, calcitonin gene-related peptide (CGRP) - Chemical, persisting mechanical and thermal stimuli |
|
|
Neurogenic Flare Response? |
Activation of pain nerves Antidromic propagation: release of neurotransmittersfrom the nerve ending at the site of injury - Bradykinin, substance P and other neuropeptides - Local vasodilatation, increased vascular permeability andinflammatory response |
|
|
Duration of a nerve action potential? |
30 milliseconds |
|
|
IPSP are caused by influx of what ion? |
Cl- |
|
|
Biosynthesis of Glutamate ? |
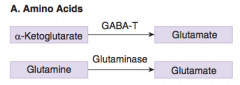
Glutamate is synthesized in the Krebs cycle bythe conversion of α-ketoglutarate to the amino acid via the enzyme GABA-T or in nerve terminals by the hydrolysis of glutamine by the enzyme glutaminase 2 methods. |
|
|
Biosynthesis of GABA? |

|
|
|
Biosynthesis of ACh? |
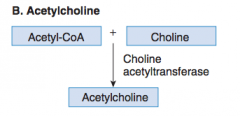
In the NERVE TERMINAL cytoplasm |
|
|
Biosynthesis of Serotonin ? |
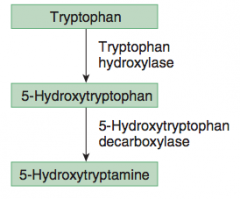
Synthesised from amino acid TRYPTOPHAN |
|
|
Biosynthesis of CATECHOLAMINES? |
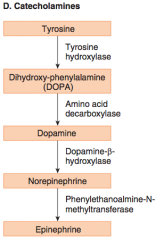
Synthesised from TYROSINE Dopamine is transported into synaptic vesicles where it is converted to NA / Adr |
|
|
Reuptake of NA at the synapse? |
NET - neorepinephrine transporter Then into vesicles via VMAT (vesicular monoamine transporter) |
|
|
Neuropeptides associated with Glutamate? |
Substance P |
|
|
Neuropeptides associated with GABA? |
Cholecystokinin, enkephalin, somatostatin, substance P, thyrotropin releasing hormone |
|
|
Neuropeptides associated with Glycine |
Neurotensin |
|
|
Effect of glutamate reuptake inhibition on nerves? |
Glutamate is an excitoxin that can kill cells by overstimulation During ischemia and anoxia - loss of neurons is increased due to inhibition of glutamate reuptake |
|
|
mAChR anatongist>? |
atropine |
|
|
Ca2+ source for Smooth muscle contraction? |
Extracellular |
|
|
The muscle spindle has a complex innervation. What specific parts of the muscle spindle do the γ neurons supply? |
Dynamic nuclear bag fibres and static nuclear bag and nuclear chain fibres |