![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
103 Cards in this Set
- Front
- Back
|
What is 0.9% normal saline ? |
Sodium chloride sodium ions (154mmol/L) chloride ions (154 mmol/L) water |
|
|
Complications of Normal saline use? |
Excessive administration of sodium chloride causes hypernatraemia, resultingin dehydration of internal organs, fluid overload, hypokalaemia and acidosis hyperchloraemic acidosis |
|
|
How much KCl can be given before checking the levels again? |
60mmol |
|
|
Fastest rate of KCl replacement |
10 mmol in 100ml NaCl over 1 hr central lines - 20mmol in 100ml |
|
|
Daily K requirement |
WHO recommends 90mmol/day but 40-60 is generally excepted 0.5mmol/kg - requirements |
|
|
Amount of K in PO replacement? |
Chlorvescent Effervescent tablets (each contains 14mmol of potassium) Slow K sustained release tablets (each contains 8mmol of potassium) |
|
|
Make up of Hartmanns? |
sodium131 mmol potassium 5 mmol chloride 112 mmol calcium 2 mmol bicarbonate (as lactate) 28 mmol. The osmolality is approximately 255mOsm/kg water |
|
|
Normal serum osmolality? |
275–295 mosm/kg (mmol/kg) |
|
|
Hartmanns osmolality |
255 mOsm/kg hypo-osmolar |
|
|
NaCl 0.9% osmolality |
285 - when done with a freezing point depression test in an osmometer some sources say 300 - depending on how it is calculated Hyper-osmolar |
|
|
Make up of 4% dextrose and 1/5th NaCl? |
1000ml bag contains Na - 30mmol Cl - 30mmol Glucose - 40g Osmolality 282 |
|
|
Daily Na requirement? |
1-2mmol/kg |
|
|
What proportion of Dextrose infusion will stay intravascularly? |
<5% |
|
|
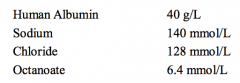
Which of the following are correct/incorrect regarding IVF: 1. Albumin is a blood product collected from plasma donations via the red cross service 2. Albumin osmolality is 260 mOsm/kg 3. Pasteurisation (heating at 60°C for 10 hours) and incubationat low pH to inactivate viruses of albumin is to reduce the risk of virus transmission 4. <10% of albumin leaves the intravascular space within 2 hrs of infusion 5. The SAFE trial looked at albumin vs normal saline resuscitation and found albumin to be inferior |
5. incorrect SAFE trial - icu - no difference in mortality, icu stay etc |
|
|
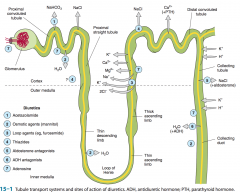
Define diuretic, naturetic, aquaretic. |
Diuretic - anything that increases urine volume.
Natiuretic - drug that increases Na excretion which also leads to volume increase
Aquaretic - increases excretion of solute free water |
|
|
Define diuretic, naturetic, aquaretic. |
Diuretic - anything that increases urine volume.
Natiuretic - drug that increases Na excretion which also leads to volume increase
Aquaretic - increases excretion of solute free water |
|
|
Cardiac output to the kidneys? |
25% |
|
|
Normal GFR |
120ml/min |
|
|
Normal filtrate volume |
7 L / hr |
|
|
Location of action of thiazides? |
Proximal tubule Sodium glucose and sodium bicarbonate cotransporters |
|
|
Na reabsorption in the parts of the tubules? |
65% proximal tubule 25% loop of henle 6% early distal 2-3% late distal/ cortical collecting duct |
|
|
Describe the blood supply to the kidney. |
Aorta -- renal artery -- segmental -- interlobar -- arcuate -- interlobular -- afferent arteriole -- glomerulus -- efferent arteriole -- vasa recta (about loops) --
same order veins out from interlobular |
|
|
Which of the following are correct / incorrect about the renal system? 1. Descending vasa recta have a non-fenestrated endothelium containing a transporter for urea 2. the ascending vasa recta have fenestrated endothelium for concerning solutes 3. Volume of blood in the renal capillaries at anyone time 100ml 4. Renal lymphatics drain via the thoracic duct 5. The renal capsule limits swelling and can raising interstitial pressure |
3. Volume of blood in the renal capillaries at anyone time 100ml - incorrect
30-40ml |
|
|
Diuretic that works at the proximal tubule? |
Carbonic anhydrase inhibitors |
|
|
MOA of acetazolamide.
ADRs
Indications. |
MOA - Carbonic anhydrase inhibitors. Blocks the formation of H2O and CO2 from H2CO3 - preventing movement into the cells and preventing reabsorption of NaHCO3 -- diuresis
ADRs - metabolic acidosis, respiratory stimulation, parasthesias, TIA in significant carotid stenosis, Stevens johnsons (HLA-B59)
Indications - glaucoma, stimulate respiration, altitude sickness |
|
|
Diuretic that works at the proximal tubule? |
Carbonic anhydrase inhibitors |
|
|
MOA of acetazolamide.
ADRs
Indications. |
MOA - Carbonic anhydrase inhibitors. Blocks the formation of H2O and CO2 from H2CO3 - preventing movement into the cells and preventing reabsorption of bicarbonate
ADRs - metabolic acidosis, respiratory stimulation, parasthesias, TIA in significant carotid stenosis, Stevens johnsons (HLA-B59)
Indications - glaucoma, stimulate respiration, altitude sickness |
|
|
MOA of carbonic anhydrase inhibitors |
Back (Definition) |
|
|
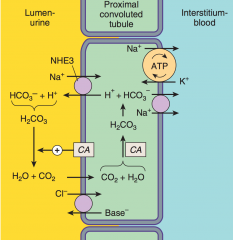
Transporters at the proximal convoluted tubule? |
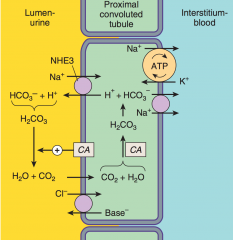
Lumen side - NHE3, Cl-/base- transporter, glucose/Na cotransporter
Interstitial side - Na/K ATPase, bicarbonate/Na cotransporter |
|
|
Example of an Aquaretic? |
Mannitol - osmotic diuretic
Prevents water reabsorption
Used for raised ICP
ADRs - initial volume expansion with hyponatraemia, then diuresis with H2O loss and hypernatraemia and volume depletion |
|
|
MOA loop diuretics.
Examples? |
MOA - inhibit luminal NKCC2 co-transporter (Na/K/2Cl) into lumen at the TAL
Blocks Na reabsorption and hence water
Examples - frusemide, bumetanide, ethacrynic acid, torsemide |
|
|
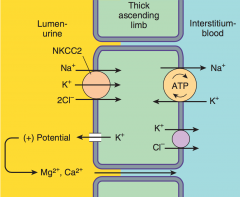
Transporters located at the TAL of the loop of henle? |
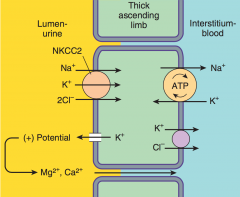
Na/K/2Cl = NKCC2 = NK2Cl K redistribution to the lumen creates a + gradient and helps the paracellular movement of Mg/Ca |
|
|
Indications for frusemide? |
Fluid overload Hyperkalaemia Hypercalcaemia |
|
|
ADRs frusemide? |
Hypokalaemia Hypomagnesaemia
Ototoxicity Hyperuricaemia |
|
|
Which is the most potent diuretic? |
Loop diuretics |
|
|
Diuretics that work at the distal convoluted tubule? |
Thiazides |
|
|
Thiazides - MOA, names, indications |
Hydrochlorothiazide + indapamide
MOA - inhibit NCC - Na/Cl cotransporter in the DCT
Indications - HTN, heart failure, nephrolithiasis due to idiopathic hypercalciuria, nephrogenic DI |
|
|
MOA of thiazides?
Transporters present at this site? |
Block Na/Cl cotransporter at the DCT |
|
|
ADRs of thiazides |
Hypokalaemic metabolic alkalosis Hyponatraemia Hypokalaemia (often not a problem due to co-administration with an ACEi)
Hypomagnesaemia
Hyperuricaemia Hyperlipidaemia Hyperglycaemia - impaired glucose tolerance Allergy - sulfa drugs |
|
|
Spironolactone
MOA Indications ADRs |
MOA - aldosterone antagonist, binds to intracellular receptor usually that stimulates ENaC (i.e. Block this effect and blocks Na reabsorption)
Indications - primary and secondary causes of hyperaldosteronism and heart failure
ADRs - Hyperkalaemia, gynecomastia (antagonism to testosterone) |
|
|
Diuretic working at the collecting duct?
MOA? |
1. Aldosterone antagonists.
I.e. Spironolactone and eplerenone
MOA - binds to an intracellular receptor that usually stimulates ENaC (Na reabsorption) -- hence this effect is BLOCKED 2. Amiloride - blocks ENaC 3. vaptans - ADH antagonists |
|
|
MOA of spironolactone and transporters present at this location. |
Aldosterone antagonist |
|
|
Describe the effect of the PCT on the solutes in the filtrate. |
66% Na resorbed with 60% of water via passive reabsorption to maintain osmolality 65% K 85% bicarb All the glucose All amino acids |
|
|
Describe the locations and mechanisms via which different diuretics work. draw the tubule |
|
|
|
Describe in words the process of bicarbonate reabsorption in the PCT. |
Na enters the cells via H/Na exchanger. Na is then pumped into the interstitium by Na/K ATPase. The H in the lumen combines with HCO3 (bicarb) to form Carbonic acid (H2CO3) --> this is rapidly dehydrated to CO2 + H2O via carbonic anhydrase --> the CO2 passively diffuses into the cell. In the cell the CO2 is rapidly rehydrated to H2CO3 by carbonic anhydrase and dissociates into H+ and HCO3- The H+ is ready to be pumped back into the lumen via H/Na exchanger and bicarbonate is transported to the interstitium via a transporter in the basolateral membrane. |
|
|
The affect of adenosine on tubular function? |
Created during hypoxia and ATP consumption Reduces GFR Increases Na reabsorption in the PCT via NHE3 activity A1 receptor antagonists significantly blunt both PCT NHE3 activity and NaCl reabsorption in the collecting duct. |
|
|
How is NaCl reabsorbed in the late PCT ? |
Due to most of the bicarb having been removed by this point the lumen becomes acidotic due to H secretion. This activates Cl/base exchanger. The net effect is NaCl reabsorption. |
|
|
How is water resorbed in the PCT? |
passive reabsorption to maintain osmotic levels in the tubule ie if an osmotic diuretic like mannitol (IVI) is present - more water stays in the lumen to maintain osmolality in the lumen |
|
|
Function of the straight proximal tubule? |
Organic acid secretion - Uric acid, NSAIDs, Diuretics, antibiotic - middle 3rd Organic base secretion - creatinine, choline |
|
|
Function of the Thin descending limb? |
Water reabsorption via osmotic forces of the hypertonic medullary interstitium |
|
|
Function of the TAL? |
Active reabsorption of NaCl from the lumen 25% but with minimal water movement Relatively impermeable to water Ie DILUTING SEGMENT |
|
|
Affect of TAL on lumenal osmolality? |
DILUTION hypo-osmolar due to salt reabsorption but not water movement |
|
|
How is Mg and Ca reabsorbed in the TAL? |
Na/K/2Cl is the main co-transport resulting in NaCl reabsorption the K is recirculated back into the lumen via RMOK2. This creates a + ionic charge and gradient to provide paracellular movement of Mg and Ca out of the lumen. |
|
|
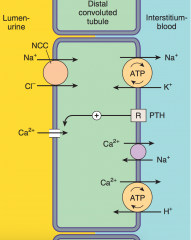
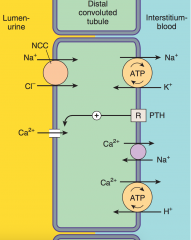
Movement of Na in the DCT? Water movement? Drug? |
Via Na/Cl cotransporter Active reabsorption of Ca (regulated by PTH) Relatively impermeable to water Thiazide diuretics |
|
|
Amount of NaCl reabsorption in the collecting duct? |
2-5% |
|
|
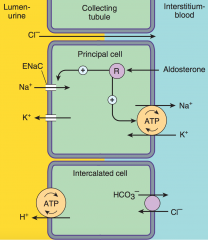
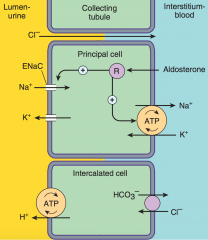
What is the function of the principal cells in the collecting duct? |
Na/K/ H2O transport Na in from lumen via ENaC (reabsorption) K out via channel (secretion) (less than Na reabsorption creating an electrical gradient driving paracellular Cl- reabsorption) |
|
|
Function of intercalated cells Alpha/Beta? |
Very similar H+ ATPase and Cl+/HCO3- exchanger are present in reversed locations for acid/bicarb secretion |
|
|
Why do diuretics increase K dumping? |
K dumping is usually occurring in the collecting ducts in exchange for Na via separate channels. Diuretics acting at earlier sites in the nephron = increased Na delivery to the collecting duct = increased Na reabsorption and the associate K dumping |
|
|
Function of aldosterone? |
Steroid hormone actions on gene transcription --> increases activity of both apical ENaC and basolateral Na/K ATPase |
|
|
Function of vasopressin in the collecting duct? |
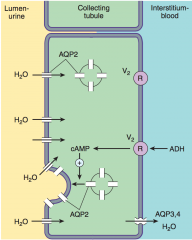
Vasopressin receptors - G protein coupled Inserts AQP2 = aquaporin 2 into the apical membrane and allows for H2O reabsorption |
|
|
Response of the kidney to hypoxia? |
Vasoconstriction --- as this reduces GFR and hence reduces tubular WORK /02 requirements unlike most organs which usually vasodilate |
|
|
Portion of the kidney at greatest risk of ischemia? |
medulla - only bloods from vasa recta |
|
|
Function of adenosine in the kidney ? |
afferent arteriole vasoconstriction - reduce GFR PCT - Biphasic effect, enhancement at low levels and inhibition at high levels of Na reabsorption TAL - CCT - unclear mechanism - reduced K dumping NET EFFECT IS ANTI-DIURETIC |
|
|
Main Prostaglandin involved in renal homeostasis that is currently understood ? |
PGE2 It blunts Na reabsorption in the TAL and ADH mediated water transport in the collecting tubules (aquaporin) |
|
|
In general what is the effect of ANP, BNP, urodilatin on the kidney? |
increase GFR diuretic effects |
|
|
Onset Duration of action excretion of acetazolamide? |
30min to onset 12 hr duration - 2 hr peak excretion - renal |
|
|
Tolerance develops to the diuretic effects of acetazolamide due to??? |
Because of early NaCl removal inhibition -- more Na to the later parts of the tubules and ovr a few days thy compensate by increasing reabsorption of NaCl |
|
|
Which diuretics cause acidosis vs alkalosis? |
Acidosis - carbonic anhydrase inhibitors, K sparing (spironolactone, amiloride) Alkalosis - loop and thiazides |
|
|
Main indications of carbonic anhydrase inhibitors? |
Glaucoma - prevent pumping of bicarb into the aqueous humour from the ciliary body = reduction in intra-ocular pressure Metabolic alkalosis - due to diuretics Acute altitude sickness - >3000m Urinary alkalinisation - in cystinuria to prevent stone formation - with po bicarb - needs to be monitored - if too alkaline causes Ca stones |
|
|
How do caffeine and theophylline produce diuretic effects? |
Weak non specific inhibition of adenosine receptors |
|
|
Benefit of Ethacrynic acid over frusemide??? |
It is NOT a SULFA drug !! |
|
|
Elimination of loop diuretics? |
Glomerular filtration and tubular secretion |
|
|
Absorption of frusemide? Duration of effect of frusemide? |
2-3 hrs Duration - 2-3 hrs |
|
|
Which drugs inhibit frusemide secretion in the straight proximal tubule? |
other weak acids ie NSAIDs, probenecid |
|
|
Indications for loop diuretics? |
1. Fluid overload/ pulmonary oedema 2. Acute hypercalcaemia 3. Hyperkalaemia 4. Acute renal failure - enhance K excretion and flush out pigements + casts causing renal failure (but worsening AKI due to Multiple Myeloma) 5. Anion overdose - bromide, fluoride, iodine - prevent reabsorption at the TAL |
|
|
ADRs Loop diuretics? |
1. Hypokalaemic metabolic alkalosis 2. Ototoxicity - dose related, potentiated by aminoglycosides 3. Hyperuricaemia - precipitate gout 4. Hypomagnesemia 5. Allergic reactions 6. Severe dehydration + hyponatraemia |
|
|
T/F all carbonic anhydrase inhibitors, loop diuretics and thiazides are sulfa drugs? |
False All except Ethacrynic acid |
|
|
Thiazides cause increased reabsorption of Ca but rarely cause hypercalcaemia - occasionally they can cause symptoms of hypercalcaemia - in what situations does this occur? |
Pre-existing hypercalcaemia ie due to hyperparathyroidism, sarcoidosis, carcinoma etc |
|
|
Which diuretics are best for states of mineralocorticoid excess? What diseases produce this state? |
Potassium staring diuretics as they work at the same location as aldosterone and blunt the wasting of K that occurs with aldosterone excess Diseases - Primary hyperaldosteronism = Conns, ectopic ACTH - Secondary hyperaldosteronism = heart failure, hepatic cirrhosis, nephrotic syndrome, states with diminished intravascular volume |
|
|
Spironolactone reduces mortality in heart failure in certain populations but caution needs to be taken when combined with what other routinely used cardiovascular medications? |
Other medications that produce hyperkalaemia such as ACEI, BB, NSAIDs, ARBs |
|
|
Contraindications of spironolactone |
CKD -- at very high risk of hyperkalaemia Dose reduction in liver failure Strong inhibitors CYP3A4 can increase levels of eplerenone but not spiro |
|
|
Strong inhibitors of CYP3A4 ? |
Antibiotics - Erythromycin/azithromycin, Metronidazole Antifungals - fluconazole/ketoconazole/voriconazole HIV antivirals TB meds - Isoniazid Grapefruit juice Cardiac meds - amiodarone, diltiazem, verapamil Cannabinoids Disulfiram SSRIs - Fluoxetine, Paroxetine, Sertraline Cyclosporin Valproic acid |
|
|
Strong inducers of CYP3A4? |
Anti-epileptics - Carbamazepine, Ethosuximide, Phenytoin Progesterone Corticosteroids Antibiotics - Rifabutin, Rifampin St John’s wort |
|
|
MOA of Vaptans? |
Vasopressin antagonists Inhibits the effects of ADH Effective in the Rx of hyponatraemia and as an adjunt to standard diuretic therapy ie for SIADH Previously lithium or demeclocycline was used for similar effects |
|
|
Side effects of vaptans? |
Nephrogenic diabetes insipidus + severe hypernatraemia Hypotension |
|
|
If a patient is not responsive to a thiazide or loop as single therapies is there any point combining the two? why? |
Yes the combination of the 2 blocks Na reabsorption a multiple points which may have been up regulated with the use of a single agent Note hypokalaemia and hypotension is common and should not be used in outpatient setting |
|
|
What is the mechanism that diuretics help in heart failure? |
When the pump stops working effectively - the kidney senses the reduced perfusion as a low volume state and acts to increase Na and Water retention. This is a vicious cycle as the increased load on the heart, with increased stretch and reduced CO causing for Na and water retention. Diuretics reduce this volume load. Reduce preload and allow the heart to pump at a more effective starting fiber length. It also helps remove fluid from the lungs, improving oxygenation and improving myocardial function. Note that excessive diuresis can reduce filling pressures to cause reduced cardiac output - balancing act |
|
|
which diuretic can be used to treat hypercalcaemia ? |
Frusemide WITH saline infusion +/- KCl as required to prevent significant volume contraction Loops - significantly inhibit Ca reabsorption in the TAL |
|
|
Which diuretic can be used to help with nephrolithiasis due to Ca stones? |
Thiazides - increased Ca reabsorption - reducing the urinary concentration of Ca should be combined with NaCl restriction otherwise the effect is diminished + increased PO fluids |
|
|
Which diuretic may be used in Nephrogenic DI? |
Seem counterintuitive to use any diuretics but Thiazides work in this situation by minimising the maximal dilution of the urine via increase Na transporters in the DCT and CCT... and other mechanisms |
|
|
Contents of albumin 4% ? |
|
|
|
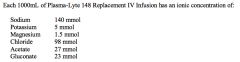
Contents of plasmalyte? |
|
|
|
Half life of most colloids? |
3-6 hrs |
|
|
Half life if crystalloids? |
20-40min |
|
|
Theoretical vs non-ideal osmolality of normal saline? |
308 - theoretical 285 - Non-ideal |
|
|
Composition of ringers lactate? |
Very similar to hartmanns Na 130 Cl 110 K 4 Ca 3 Lactate 28 |
|
|
Metabolism of lactate in hartmanns? |
70% - gluconeogenesis in the liver and kidney 30% - bicarbonate in the liver |
|
|
Benefits of hypertonic saline? |
Large volume expansion - 3-4x the infused volume Rapid response May improve myocardial function May vasodilate vascular beds Reduces ICP |
|
|
Problems with hypertonic saline |
Adverse effect on T cell function Increased vascular permeability Coagulopathies Long term use can lead to hypernatraemia and hypertonicity |
|
|
Name the commonly used colloids. |
Albumin Gelatins Dextrans Starchs - such a hydroxyethyl |
|
|
Albumin is a blood product - what measures have been taken to minimise risk of infection into the recipient? |
Pasteurised 10hrs at 60C |
|
|
Basic structure of a starch? |
Long glucose chain - polymer with hydroxyethyl groups Made from corn |
|
|
Source of gelatin? |
cattle bones |