![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
66 Cards in this Set
- Front
- Back
|
bacteria |
smallest living things and lack mitochondria, nucleus, Golgi, ER, lysosomes; therefore prokaryotic; their shapes include: diplococci(pairs), coccobacilli, vibrio, bacilli (rods), spirillium + spirochete (spiral); bacterial aggregates: diplococci(pairs), streptococci (chains), staphylococci (irregular); structure can be divided into envelope and interior, grow via binary fission growth: lag, log(exponential), stationary (only so much space nutrients), death (used up nutrient) |
|
|
envelope |
protects bacteria against chemical and biological threats, carries out many bacterial processes, contains appendages that make it possible for bacteria to colonize surfaces
|
|
|
bacterial cell wall |
essential to bacterial life, almost all bacteria have a rigid peptidoglycan (murein) layer that surrounds the cytoplasmic membrane; cell wall used to distinguish between G(+) and G(-)is called gram stain |
|
|
beta-lactams |
prevent bacteria from the final stages of constructing a cell wall (cross-linking of the peptide subunits) creating an osmotically imbalanced bacteria, mostly used against G(+) bacteria |
|
|
amoxicillin |
is a synthetic derivative of penicillin, and has a greater activity against G(-) due to the added free amino group; side chains may contribute to allergic reaction |
|
|
G(+) bacteria |
thick, multilayered cell wall; consists of NAG (N-acetylglucosamine) + NAM (N-acetylmuramic acid), crosslinked into sheets by amino acids, embedded with teichoic acid which consists of polymers of glycol phosphate or ribitol phosphate with extra moieties such as amino acids; lipoteichoic acid, has a fatty acid that anchors it into the cytosolic membrane, promote bacterial adhesion to host |
|
|
G(-) bacteria |
have an outer membrane and inner membrane, as a result the periplasmic space is created; which contains metabolic enzymes, virulence factors and the non-extensively linked peptidoglycan wall
outer membrane contains endotoxin (LPS, lipopolysaccharide), which is composed of Lipid A, core polysaccharide, and O antigen; and porins which allows of active transport and diffusion |
|
|
bacterial cell membrane |
electrons transport system of the cell, vital for cell growth, similar to eukaryotic cells except that it has many more proteins and no sterols (except Mycoplasma), bacterial chromosome is attached to cell membrane, has proteins controlling entrance and exit of solutes and proteins |
|
|
bacterial capsule |
capsules are found on both G+ and G-, polysaccharide (slime layer) is a major virulence factor but non essential for survival, protect against phagocytosis and resist complement binding |
|
|
flagella |
responsible for locomotion, found on G+ and G- bacteria; the bacterium may have one none or many; made of helically coiled proteins that are anchored into bacterial inner membrane; proteins are called flagellin and have many different structures depending on the strain (used for differentiation) |
|
|
bacterial cytosol |
contains many ribosomes made of (5 S, 16 S, 23 S rRNA and one 50S and one 30S protein subunit), there is little structural but considerable functional homology between prokaryotic and eukaryotic ribosomes, most ribosomes at any given time are involved in the translation of mRNA |
|
|
nucleoid
|
bacterial cells lack a membrane defined nucleus, however a discrete region in the bacterial cytoplasm seems to contain the genetic material and this cleoid region can often be distinguished on EMS of cells, most cells have only one main chromosome which consists of a single circle of DNA |
|
|
plasmids |
bacterial extrachromosomal small circular pieces of DNA which are capable of autonomous replication |
|
|
bacterial replication of DNA |
starts at replication forks and proceeds bidirectionally similar to eukaryotic DNA, similar to mammalian DNA replication, involves RNA primer and Okazaki fragments, helicase, and primase, since bacterial chromosome is circular, replication introduces a lot of torsion in the strands, relieved by enzyme gyrase |
|
|
bacterial transcription |
bacterial DNA-dependent-RNA polymerase is composed of several subunits, sigma factor recognizes a particular sequence of nucleotides in the DNA promoters in order to initiate transcription, alpha and beta subunits carry out polymerization |
|
|
differences between eukaryotic + prokaryotic transcription |
in bacteria a single RNA polymerase makes all RNA in humans there different RNA polymerases for mRNA, tRNA, and rRNA, bacterial mRNA has a much shorter half life than eukaryotic mRNA, organization of genes in bacteria multicistronic operons |
|
|
operon
|
a unit of transcription containing several genes (cistrons) that are transcribed as a single mRNA; the operon usually consists of a promoter, operator, and terminator |
|
|
sources of energy
|
all bacteria (aerobic + anaerobic) use Embden-Meyerhof-Parnas (EMP) glycolytic pathway to make pyruvate from glucose, fermentation aerobic respiration anaerobic respiration |
|
|
fermentation |
large amount of organic acids and alcohols are produced from pyruvate which receives electrons from NADH, has low ATP generating efficiency because ATP only comes from EMP pathway
|
|
|
aerobic respiration
|
in the presence of oxygen, pyruvate is complete oxidized tow water and CO2 via TCA cycle, electrons from NADH + FADH are transferred through a chain of carriers to an ultimate acceptor (usually oxygen), efficient at generating ATP especially when combined to EMP pathway, bacteria that grow aerobically and thus utilize respiration must protect themselves from toxic radicals |
|
|
anaerobic respiration |
electron-transport chain requiring biological process which couples the oxidation of NADH (electron donor) to the reduction of an exogenous electron acceptors other than molecular oxygen |
|
|
obligate anaerobes |
makes ATP via fermentation or anaerobic respiration, lack enzymes needed to break superoxide ions no catalase, no superoxide dismutase and no peroxidase
|
|
|
obligate aerobes
|
makes ATP via aerobic respiration, cannot grow without O2, contain superoxide dismutase and catalase, but not peroxidase |
|
|
Facultative anaerobes
|
makes ATP via fermentation or anaerobic + aerobic respiration, can grow without oxygen, contain superoxide dismutase and catalase, but not peroxidase |
|
|
oxygen tolerant anaerobes |
make ATP via fermentation but can grow in the presence of oxygen, contain superoxide dismutase and peroxidase, but not catalase
|
|
|
gram staining |
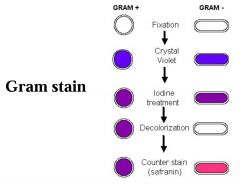
in order: crystal, violet, iodine, alcohol, & safranin
G(-) bacteria would appear red under microscope IF you forgot to add crystal violet; and would appear purple if alcohol was omitted |
|
|
biochemical test for catalase |
differential for these organism that can convert hydrogen peroxide to water and oxygen gas, identifies the presence of obligate aerobes or facultative anaerobes |
|
|
nutrient media |
contains all the ingredients necessary to support the growth of most bacteria, usually made of digests of animal or plant products sucks as milk or beans, may also contain vitamins and salts depending on the bacteria isolated |
|
|
selective media |
inhibits growth of unwanted organisms from the normal flora, usually contains chemical additives such as antimicrobial agents contaminating flora but not the pathogen of interest |
|
|
differential/indicator media |
demonstrates biochemical features of organisms, most often a carbohydrate and a pH indicator are added to see whether the organism can ferment that carbohydrate to produce acid which then changes the color of the pH indicator and therefore the color of the colony |
|
|
bacterial identification techniques |
bacteria are cultured to create a specimen and grown on an agar plate, the shape of the colony can be used, as well as light microscopy, gram staining, acid fast stains, fluorescent microscopy and NAT(nucleic acid amplification test) |
|
|
endotoxin |
virulence factor, (LPS) lipopolysaccharide, only present in G(-) bacteria, component of the cell membrane, lipid A of LPS is toxic, only one type, heat stable, affects many cells and tissues, no toxoid vaccine. in the body presence leads to hypotensive shock, low iron, and hypoglycemia |
|
|
exotoxin |
virulence factors; enterotoxin cytotoxin, neurotoxin, may be contained by G(+) and G(-), many types, heat labile, bind specific receptors on specific cells, each toxin has a very specific effect, toxoid vaccines are available |
|
|
staphylococcus aureus
|
gram(+), cocci, have catalase, is a facultative anaerobe, coagulase + (converts fibrinogen to fibrin, which walls bacteria from immune response); carried in the normal flora of skin and mucosa, can enter the blood through any gap in the skin, bodily colonization sites nose (main one), axilla (armpit), rectum, perineum (just anterior to the anus), in the vagina (higher percentage in period blood) |
|
|
staphylococcus aureus colony in lab |
colonies are golden in color, grow best in mannitol salt agar (high salt concentrations, haloduric, produces a yellow color when mannitol, as a result phenol red indicators turns yellow) |
|
|
hemolysis of staph on blood agar |
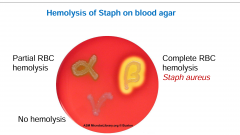
beta-hemolytic species: completely rupture the red blood cells (visible as a halo in culture) caused by hemolysins
alpha-hemolytic species: oxidize iron in the hemoglobin (turning it a dark green color in culture) caused by peroxidases gamma-hemolytic species: do not cause hemolysis and really cause illness |
|
|
staphylococcus aureus virulence factors |
Protein A binds to the Fc region of IgG and blocks Ab, Alpha-toxin makes pores in cells resulting in lysis, exfoliative toxins separate dermis and epidermis; superantigen-like toxins TSST1(toxic shock syndrome toxin1): activates T cells and APC without antigen specificity causing massive cytokine release, lysis and leakage; SEB (Staph enterotoxin B) causes gut-intestinal fluid loss with diarrhea + vomiting, not absorbed from GI to blood |
|
|
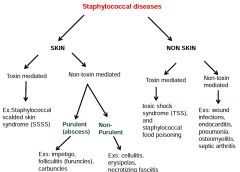
overview of staphylococcus aureus diseases |
|
|
|
impetigo |

superficial infection that causes the production of pus-filled vesicle; epidermal (cutaneous); non toxin mediated staph skin infection |
|
|
furuncles/folliculitis/boils |
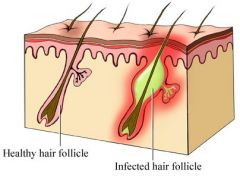
infects cells of dermis painful raised nodules that have an underlying collection of necrotic tissues/pus extends deeper than hair follicle; non toxin mediated staph skin infection |
|
|
carbuncles (fused boils)
|

infects cells of dermis , coalescence of furuncles with invasion of deeper subcutaneous tissue; patients have chills and fever which suggest a systemic infection; non toxin mediated skin staph infection; associated with pus and and green abscess, the abscess can grow under a large portion of the skin |
|
|
cellulitis (& Fasciitis) |
inflammation of the connective tissue below dermis as well as other subcutaneous tissue (warm + painful), cellulitis can result in fever and chills in addition to skin infection; non toxin mediated staph skin infection; |
|
|
erysipelas |
lesion with sharply demarcated raised edge, red swollen warm hardened and painful; no effect on subcutaneous tissues, no release of pus (sign of deep infection), only serum or serous fluid, rapid invasion and spread through lymphatic vessels, produces overlying skin "streaking" and regional lymph node swelling and tenderness; non toxin mediated staph skin infection |
|
|
Scalded skin syndrome (ritter's disease) |
usually in babies, results from exfoliative toxin production in lesions, blistering skin, few bacteria in lesions-caused by toxin, few leukocytes presents in lesions, slight pressure on the skin displaces it, disease symptoms look bad but no scarring, lack of syndrome in adults due to presence of antibodies specific exotoxins, improved renal clearance of toxins; toxin mediated staph skin infection |
|
|
non toxin mediated non cutaneous staph infection |
bacteremia + endocarditis often hospital acquired and is associated with bacteria from the skin getting into the bloodstream; can result from surgical procedure or contaminated intravascular catheter, endocarditis needs to be treated promptly, otherwise the patient has poor prognosis osteomyelitis can result from trauma that spreads the bacterial infection to the bone, especially in children with growing vascular bones, the disease is characterized by localized pain, high fever and purulent discharge from the sinus tract overlying the infected bone pneumonia consolidation and abscess, high risk for elderly patients and in patients with underlying pulmonary disease |
|
|
toxin mediated non cutaneous staph infection |
Food Poisoning most common form of food poisoning in the US, food is contaminated by someone whose skin or nasopharyngeal fluid is infected with the enterotoxin-carrying S. aureus strain, food remains at room temperature bacteria can grow, bacteria release enterotoxin into the food, the toxin is ingested and is not readily destroyed by gut, while bacteria can be killed by reheating, toxin is heat resistant; induces vomiting with no fever; non infectious Toxic Shock Syndrome release of toxin (TSST-1 + SEB) into blood causes massive cytokine release, symptoms: fever hypotension, diffuse rash, sloughing of skin, multiple organ failure, no bacteria in the blood, post infection from the toxin |
|
|
enterotoxin mechanism |

non specific binding of T-cells to MHC of APC by superantigen CD3 is going to start signalling to the T cells to activate, and divide and thus secret cytokines in turn causes the low blood pressure and increased heart rate, fever, |
|
|
diagnosis of staph infection |

gram staining of the lesion illustrates G(+) cocci in clusters, lesions usually contain many neutrophils and bacteria that can be easily cultured overnight in aerobic environment in media containing blood agar, staph produces hemolysin which causes B (complete) hemolysis of RBC, to select the growth of staph aureus, the agar should be supplemented with 7.5 NaCl inhibits growth of most organisms), mannitol (fermented mainly by staph, not other organisms), colonies can be tested for coagulase and catalase
|
|
|
staph treatment
|
infections acquired outside hospital can usually be treated with penicillinase-resistant-B-lactams, hospital acquired infection is often caused by antibiotic resistant strains and can only be treated with vancomycin |
|
|
MRSA |
many staph infections have become resistant to penicillin, methicillin, and some are even resistant to the last resort vancomycin, most resistance genes are plasmid-encoded; HA-MRSA usually due to devices in hospitals; CA-MRSA usually due to immune suppression eg chemo
|
|
|
unique features of retroviridae |
enveloped with a capsid containing two copies of positive strand RNA genome, RTase & integrase enzymes are carried in the virion, replication proceeds through a DNA intermediate termed a provirus, the provirus integrates randomly into the host chromosome and becomes a cellular gene, tx of the genome is regulated by the interaction of the host Tx factors with promoter and enhancer elements in the LTR portion of the genome, HIV is easily inactivated and must be transmitted in bodily fluids |
|
|
simple vs complex retroviruses |
simple retroviruses encode gag, pol, and env genes complex retro viruses also encode accessory genes (HIV is a complex virus) |
|
|
HIV replication cycle |
entry of HIV into cells, reverse transcription, integration, transcription/replication, translation, assembly and budding |
|
|
entry of HIV into cells
|
gp120 binds to CD4 (on T cell; Mo/MØ) gp120 then change its shape and binds to chemokine gp41 becomes exposed and induces virual fusion at normal body pH |
|
|
HIV reverse transcription & integration |
RTase make DNA strand complementary to genomic RNA DdD polymerase and RNA-ase activities allow formation of double-stranded viral cDNA viral cDNA is integrated into host chromosome |
|
|
transcription/replication/translation of HIV genome |
usually in activated T cells, T cells are activated by HIV or by being primed for infection, viral mRNA and genomic RNA is made and transported to the cytoplasm, late proteins GAG and Env and Pol are translated as polyproteins |
|
|
assembly and budding |
Env polyprotein (gp 160) is cleaved into gp 120 and gp41 in the cell during budding and release: Gag polyprotein is cleaved into matrix and nucleocapsid Pol polyprotein is cleaved into protease, reverse transcriptase and integrase virus can cause syncytia formation with subsequent lysis of these cells |
|
|
HIV infection |
1 mucosal DC deliver HIV into lymph nodes where it can infect CD4 T cells, mucosal LN are especially affected 2 massive viremia leads to disseminated infection of other lymphoid organs as well as macrophages (microglial cells) in the brain 3 infection of cells of the brain including microglial cell and neurons causes the release of neurotoxic substances and promote inflammatory response in the brain 4 CD4 T cells most likely to be killed by HIV are those currently fight HIV or other infection because they are activated and support replication of HIV 5 diseases related to AIDS mainly consists of opportunistic infections, infection, cancers & CNS pathology |
|
|
HIV disease progression |
initial HIV symptoms occur 2-4 week after infection, resemble influenza or mono these subside after several weeks and are followed by a period of asymptomatic infection with some lymphadenopathy that can last for years. CD4+Th cells and CD8+CTL and antibodies control viral load but do not clear the virus; when CD4 T cell count drops below 450 cells per microliter opportunistic infection may begin to appear; when T cell count drops below 200 then serious infection can occur |
|
|
HIV subversion |
CD4 T cells are killed directly by HIV indirect killing → inflammation & apoptosis homeostatic deregulation (damage of lymphoid organs (ex. thymus + lymph node) |
|
|
HIV mutations |
during replication of genome can lead to escape of HIV from the immune response epitope recogntion
|
|
|
HIV latency |
there is a latent viral reservoir in lymphoid tissue |
|
|
HIV inhibitory molecules |
long term exposure to virus causes immune cells to upregulate inhibitory receptors
|
|
|
Passage of virus from mother to fetus
|
in the absence of treatment, the risk of HIV transmission from mother to child is 25-30%
antiretroviral medication lower mother to infant transmission to less than 2% the vast majority of transmission of HIV mother to child occurs at the time of birth when the membrane is ruptured and the blood system can mix |
|
|
HIV detection assays |
anti-HIV-1 antibodies: serum ELISA or WESTERN Viral DNA: blood or cells PCR p24: blood ELISA |
|
|
HIV treatment |
nucleoside RTase inhibitors (NRTIs) non-nucleoside RTase inhibitor (NNRTIs) helped stop perinatal transmission protease inhibitor (Pls) integrase inhibitor (IIs) CCR5 antagonists Fusion inhibitor target gp41 these drugs only work in active cells |