Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
24 Cards in this Set
- Front
- Back
|
What does a positive PPD indicate?
|
1. Current infection 2. Past exposure 3. BCG vaccination
|
|
|
What does a negative PPD indicate?
|
1. No infection 2. Anergy (due to: steroids, immunocompromise, malnutrition)
|
|
|
Fast-fermenting lactose bacteria
|
Fast fermenters: (EEK! Too fast!) 1. E.coli 2. Enterobacter sp. 3. Klebsiella
|
|
|
Slow fermenting lactose bacteria
|
Slow fermenters: 1. Serratia 2. Citrobacter 3. "Others"
|
|
|
Tuberculosis infection: Gross mechanism
|
1. Inhaled aerosols from infected adults
2. Land in middle or lower lobes of lung (highest airflow) leading to small area of pneumonitis. 3. Bacteria enter macrophages, multiply, and spread hematogenously. |
|
|
Mechanism of asymptomatic primary TB
|
1. Cell-mediated defense walls off foci of bacteria in caseous granulomas 2. Granulomas heal with fibrosis, calcification and scar formation
|
|
|
Difference between Ghon focus and Ghon complex
|
Ghon focus: Calcified tubercle in the middle or lower lung
Ghon complex: Ghon focus accompanied by perihilar or lobar lymph node calcified granulomas |
|
|
What is a Ranke complex?
|

Same as a Ghon complex: Ghon focus (TB granulomas) and perihilar or lobar lymph node calcified granulomas
|
|
|
Mechanism of symptomatic primary TB
|
1. Large caseous granulomas develop in the lungs/other organs. 2. In the lungs, caseous material liquifies, is extruded out the bronchi and leaves cavitary lesions behind.
|
|
|
Mechanism of secondary Pulmonary TB
|
1. Infection occurs at apical areas of lung around the clavicles due to highest oxygen tension caused by decreased pulmonary circulation.
2. Infected areas grow, caseate, liquify and cavitate. |
|
|
TB reactivation sites
|
1. Pulmonary (Lung parenchyma)
2. Pleura 3. Pericardium 4. Scrofula (Cervical lymph nodes: most common extrapulmonary site worldwide) 5. Kidney (Sterile pyuria) 6. Thoracic and lumbar spine (Pott's disease) 7. Chronic monoarthritis 8. CNS (subacute meningitis or parenchymal tuberculoma) 9. Miliary TB (Millet sized tubercles all over the body) |
|
|
Tuberculosis rule of 5s
|
1. Droplet nuclei are 5 micrometers and contain 5 mycobacteria 2. 5% risk of reactivation in first 2 years and then 5% lifetime risk 3. Patients with HIV ("High five") have 5+5% yearly reactivation risk. 4. Induration measurements: a. HIV: >5 mm b. High risk: >5+5 mm c. Everyone else: >5+5+5 mm
|
|
|
Cause of Miliary tuberculosis
|
Severe bacteremia
|
|
|
Types of Mycobacteria and what they cause
|
Mycobacterium:
1. Leprae: Leprosy/Hansen's disease 2. Tuberculosis: TB 3. Avium-intracellulare: Disseminated disease in AIDS 4. Scrofulaceum: Cervical lymphadenitis in kids 5. Kansasii: Pulmonary TB-like synmptoms Mnemonic: Identifying mycobacteria is no Light TASK |
|
|
What disease state does Mycobacterium Avium-intracellulare cause?
|
bugs are multiple drug resistant and cause disseminated disease in AIDS
|
|
|
Symptoms of tuberculosis
|
1. Fever 2. Night sweats 3. Weight loss 4. Hemoptysis
|
|
|
Langhans type giant cells in which the nuclei are lined up around the periphery of the cell in a horseshoe pattern. Seen in granulomatous conditions like TB
|
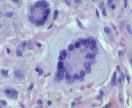
What is this?
|
|
|
What is Hansen's disease?
|
leprosy
|
|
|
What is leprosy caused by?
|
Mycobacterium leprae
|
|
|
Characterization and reservoir of Mycobacterium Leprae
|
1. Acid fast bacillus
2. Likes cool temperatures 3. Infects skin and superficial nerves 4. Cannot be grown invitro 5. Reservoir: Armadillos |
|
|
Presentation of lepromatous leprosy
|
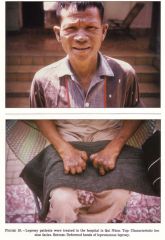
"Leonine facies": 1. Loss of eyebrows 2. Nasal collapse 3. Lumpy earlobe
|
|
|
Treatment for leprosy
|
Long-term oral dapsone - Alternative: Rifampin or combo clofazimine and dapsone
|
|
|
Toxicity of longterm oral dapsone
|
1. Hemolysis 2. Methemoglobinemia
|
|
|
2 forms of leprosy
|
1. Lepromatous (Due to failed cell-mediated immunity. Lep. is Lethal)
2. Tuberculoid (self-limiting) |