Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back
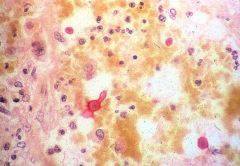
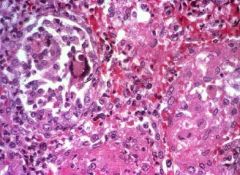
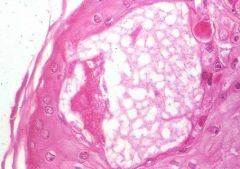
This is mucicarmine and india ink stain.What is depicted?
|
Cryptococcus neoformans.
The organism grows in tissue as an encapsulated yeast. The polysaccharide capsule is the virulence factor, and is mucicarminophilic (stains with mucicarmine as illustrated). Infection is usually pulmonary; the organism may spread to the CNS and produce a meningoencephalitis. The organism can be identified by staining a CSF sample with India ink.Immune competent persons can be infected, but the infection is more often encountered in immunosuppressed individuals. |
|
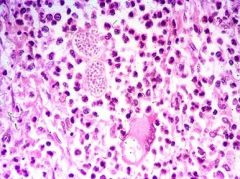
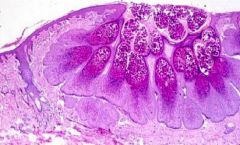
Road trip across the US. Saw this spherules with endospores. What is it?
|
Coccidioides immitis
Infection occurs by inhalation of spores. Primary infection causes delayed-type hypersensitivity and may be asymptomatic. In 10% of cases, patients develop lung lesions with cough, fever and pleuritic pain. The tissue response may be granulomatous or neutrophilic inflammation, or combination of both. In a small number of cases, the infection disseminates to skin and meninges. The organism occurs as hyphae with arthrospores in nature; and as spherules with endospores in tissue. Causes pulmonary, cutaneous, subcutaneous, osseous and uniquely, meningitis. PULMONARY: Similar to Blasto. Generally get upper lobe infiltrates, a pneumonia that doesn't respond to antibiotics. Primary: infiltrates in upper lobes, then persistent pneumonia, nodular and cavitary disease SKIN AND SUBCUTANEOUS: Verrucous granulomas, nodules, abscesses OSSEOUS: Predilection for areas where tendons insert into long bones or joints, may form sinus tracts to skin, can cause vertebral infection. Grossly looks like Blasto, only hint is where the person has traveled. |
|
|
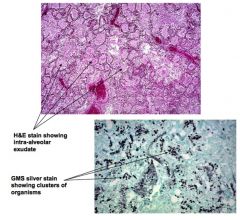
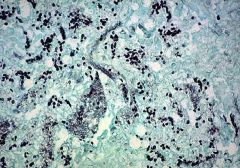
PJP
- causes opportunistic pneumonia in patients with immunodeficiency, such as in HIV/AIDS - P. jirovecii is a yeast-like fungus that can be found in the lungs of normal persons, but causes pneumonia in immunocompromised individuals. The typical tissue reaction in the lung is the presence of an intra-alveolar “foamy” pink exudate (seen on H&E stain), within which the cyst form of the organism can be seen in clusters (on silver stain). Other common causes of opportunistic infection in patients with HIV/AIDS include: Candida sp., CMV, atypical mycobacteria, Cryptococcus, Toxoplasma, and Cryptosporidia. |
|
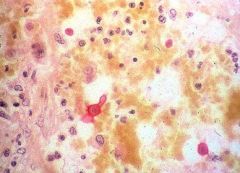
High mag view of organsism found at edge of flask-shaped ulcer bed
|
Entamoeba histolytica
protozoan parasite that is transmitted via fecal-oral contamination, with ingestion of mature cysts. chief differential diagnosis for patients presenting in the acute phase in ulcerative colitis. The organisms can spread to the liver via the portal system, and cause one or more abscesses in the liver. Occasionally the organisms spread to lung, kidneys and brain. The organisms can be identified by examination of stool or culture. Liver involvement may be diagnosed by aspirates or biopsy of the edge of an abscess. |
|
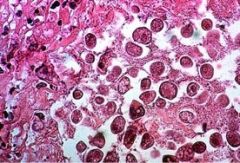
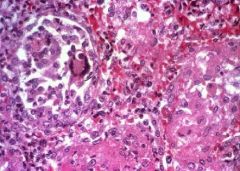
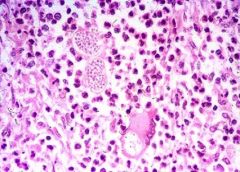
Yeast form in a giant cell, granulomas
|
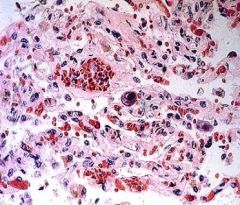
Blastomycosis
endemic in the Ohio and Mississippi river valleys and the southeast US, including parts of Virginia. Infection is acquired by inhalation. Spread is hematogenous. Infection and disease can occur in immune competent as well as immunocompromised individuals. Major sites of involvement are the lungs, skin, bones and genitourinary tract. The tissue response is usually suppurative granulomas (granulomas with central collection of neutrophils). Skin lesions are characterized by marked hyperplasia of the epidermis and microabscesses. |
|
|
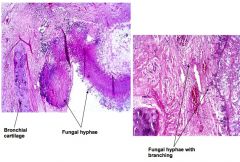
Aspergillosis! Fungal hyphae are sepate and branch at 45 degree angles. Common in immunocompromised. IS ALWAYS A MOLD!
Allergic bronchopulmonary aspergillus: Clinically represents asthma. Wheezing patient. Problem is airways are colonized with aspergillus and are having an allergic reaction to it! Blood tests will yield: eosinophilia, an increase in IgE. Treat with corticosteroids since it is not an infection but an immunological thing. Fungus ball: growth in pre-existing pulmonary cavity (sarcoidosis, TB, emphysema). Aspergillosis: Invasive pulmonary disease Neutropenia (leukemia, bone marrow transplant) High doses of corticosteroids for prolonged periods Primarily pulmonary but may spread hematogenously to brain. Acute rhinosinusitis might also occur --> invasion of vessels, necrosis and black eschar occur. |
|
A chest radiograph demonstrates diffuse density involving a large portion of the right lung, with sharp demarcation from the surrounding normal-appearing lung. The physician obtains a sputum sample, performs a Gram stain, and examines the specimen under the microscope. She sees numerous neutrophils and Gram-positive cocci.
|
the inflammatory infiltrate (neutrophils and fibrin) fills alveolar spaces and involves all, or most of, one or more lobes.
Streptococcus pneumoniae causes most cases of lobar pneumonia, and is the most common cause of community-acquired acute bacterial pneumonia (lobar pneumonia or bronchopneumonia). |
|
|
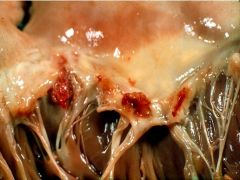
That is infective endocarditis and vegetations on the valve leaflet.
|
|
papular lesions on the skin of the boy’s arm, which he had been scratching. The child denied any symptoms and showed no change in appetite or energy level. On physical examination, the pediatrician found no abnormalities except for the skin lesions. These were a cluster of raised skin lesions, each measuring about 2 mm, on the forearm. The papules had a pearly appearance and central umbilication.
|
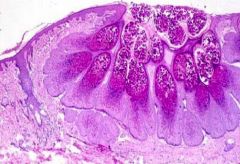
Molluscum contagiosum
- Infection causes umbilicated, painless but pruritic, 2-5 mm papules, usually on the trunk and extremities - Histology of lesions shows epidermal hyperplasia, with diagnostic cytoplasmic viral inclusions (“molluscum bodies”) in the stratum granulosum and stratum corneum. |
|
A 50 year old man, six months post kidney transplantation, presented to his physician with complaints of fever, malaise and non-productive cough. Chest radiograph demonstrated bilateral densities in the lung fields.
|
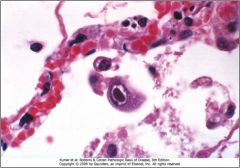
CMV
- Member of β-herpesvirus subfamily. Causes latent infections (within leukocytes), that are usually asymptomatic except in immunosuppressed individuals. - CMV-infected cell typically is increased in size (cytomegaly) with a single large intranuclear inclusion and multiple smaller intracytoplasmic inclusions. - Congenital form causes jaundice, encephalitis, hepatitis, pneumonitis; in adolescents CMV can cause a mononucleosis-like illness; lungs, GI tract and other sites can be affected in immunocompromised patients |
|

|
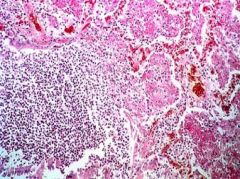
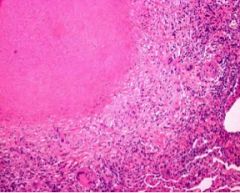
Tuberculosis of lung with numerous caseating granulomas.
|
|
|
Necrotizing (caseating) granulomas in a case of tuberculosis. Ziehl-Neelsen (acid fast) stain would demonstrate the organisms within the granulomas.
|
|
|
Cytomegalovirus infection of the lung. The infected cell is enlarged, and there is a single large inclusion in the nucleus and multiple small inclusions in the cytoplasm.
|
|
|
Varicella infection, with vesicle formation in the epidermis. Note the intranuclear inclusions in infected cells at the edge of the vesicle.
|
|
|
Molluscum contagiosum, with hyperplasia of the epidermis and numerous brick-red inclusions in the infected cells.
|
|
|
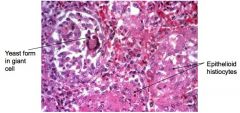
High magnification: Blastomycosis in lung. One of the organisms is present within a giant cell (arrow). The inflammatory response is granuloma formation.
|
|
|
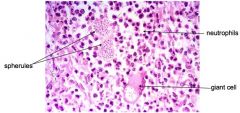
Coccidioidomycosis involving lung. Note the distinctive appearance of the fungus as spherules containing endospores. There is a neutrophilic and granulomatous (giant cell) response.
|
|
|
High magnification of Cryptococcus, stained with mucicarmine stain, which highlights the capsule of the yeast. Note the narrow-necked bud typical of this organism.
|
|
|
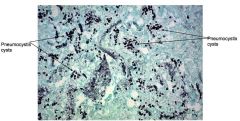
Pneumocystis jiroveci (formerly called P.carinii) is a fungus that can cause disease in the lungs of immunocompromised persons. The characteristic histologic change (on H&E stain) is the presence of foamy pink material in alveolar spaces. Clusters of the cyst form of the organism are identified within this material on silver stain (GMS stain), as illustrated here.
|
|
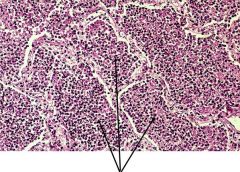
Is this lobar or bronchopneumonia?
|
Microscopic: Lobar Pneumonia - Gray Hepatization. The alveoli show a uniform infiltration of neutrophils. Note that all alveoli show the same stage of pneumonic infiltration. In bronchopneumonia, patches of inflammation are at different stages of development.
|