Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
77 Cards in this Set
- Front
- Back
|
What are some basic general characteristics about fungi?
|
*Eukaryotic
*Don't contain chlorophyll and don't photosynthesize *chemoheterotropic *rigid cell walls composed of chitin, glycans *basic morphology: yeasts or molds or dimoprhic (mold in vitro, yeast in vivo). |
|
|
What are the clinical categories of fungal infections? (4)
|
Superficial Mycoses (dermatophytosis, Candida species, Malassezia fufur, Exophilia werneckii, Trichosporon beigelii)
Supcutaneous Mycoses (Mycetomas, Chromomycosis, Phaeohyphomycosis, Sporotrichosis Deep (Systemic) Mycoses- Classical (Sporotrichosis, Blastomyces dermatitides, Coccidiodes imitis, Histoplasma capsulatum, Paracoccidiodes brasillensis) Deep (systemic) mycosis - opportunistic fungal infections (Aspergillus species, Candida species, Cryptococcus neoformans, Zygomycetes) |
|
|
Which clinical category of fungal infection do these belong to:
dermatophytosis, Candida species, Malassezia fufur, Exophilia werneckii, Trichosporon beigelii A. Superficial Mycoses B. Subcutaneous Mycoses C. Deep (Systemic) Mycoses - Classical D. Deep (Systemic) Mycoses - opportunistic fungal |
A. Superficial Mycoses
|
|
|
Which clinical category of fungal infection do these belong to:
Mycetomas, Chromomycosis, Phaeohyphomycosis, Sporotrichosis A. Superficial Mycoses B. Subcutaneous Mycoses C. Deep (Systemic) Mycoses - Classical D. Deep (Systemic) Mycoses - opportunistic fungal |
B. Subcutaneous Mycoses
|
|
|
Which clinical category of fungal infection do these belong to:
Sporotrichosis, Blastomyces dermatitides, Coccidiodes imitis, Histoplasma capsulatum, Paracoccidiodes brasillensis A. Superficial Mycoses B. Subcutaneous Mycoses C. Deep (Systemic) Mycoses - Classical D. Deep (Systemic) Mycoses - opportunistic fungal |
C. Deep (Systemic) Mycoses- Classical
|
|
|
Which clinical category of fungal infection do these belong to:
Aspergillus species, Candida species, Cryptococcus neoformans, Zygomycetes A. Superficial Mycoses B. Subcutaneous Mycoses C. Deep (Systemic) Mycoses - Classical D. Deep (Systemic) Mycoses - opportunistic fungal |
D. Deep (systemic) mycosis - opportunistic fungal infections
|
|
|
Dermatophytosis involves a variety of skin conditions named by site, not species of infection. What is each's location and what genus(es) (Trichphyton, Microsporum, Epidermophytous) is responsible?
A. Tinea capitis B. Tinea pedis C. Tinea cruris D. Tinea corporis E. Tinea barbae F. Tinea unguium |
Tinea capitis = scalp (if only skin involved, then Epidermophyton, if skin+hair shaft, Trichphyton or Microsporum)
Tinea pedis = feet (can be caused by all three genuses, most commonly due to Trichphyton) Tinea cruris = groin region (caused by Epidermophyton) Tinea corporis = skin Tinea barbae = beard area Tinea unguium = nails (caused by Trichophyton) |
|
|
True or False:
For dermatophytosis, specific diagnosis to the causative genus is NOT required for treatment because they are all treated the same! |
True
Just treat with topical anti-fungal cream. |
|
|
Dermatophytosis is caused by 3 genera, based on conidia. Tell whether each of the following affects hair, nails, skin or any combo of em.
A. Epidermophyton B. Microsporum C. Trichophyton |
A. Epidermophyton - skin and nails
B. Microsporum - skin and hair C. Trichophyton- skin, hair and nails |
|
|
In healthy individuals, this causes: Diaper rash, interiginous folds (bra lines in pendulous breasts, under ipanis aka large bellies).
|
Candida species
IMMUNOCOMPROMISED: Fungemia, disseminated candidiases (in blood!), hepatosplenic candidiases (in neutropenic cancer patients), oral and esophageal thrush, chronic mucocutaneous candidiases (a genetic immune disorder with crusted painful skin and oral lesions) |
|
|
In immunocompromised individuals, this causes: Fungemia, disseminated candidiases (in blood!), hepatosplenic candidiases (in neutropenic cancer patients),
oral and esophageal thrush, chronic mucocutaneous candidiases (a genetic immune disorder with crusted painful skin and oral lesions) A. Candida species B. Exophilia werneckii C. Malassezia furfur |
A. Candida species
|
|
|
What is tinea versicolor caused by? (instigator, fungus, and necessary component)
|
After sun exposure, folliculitis or patchy skin depigmentation occurs due to Malassezia furfur. Requires lipids to grow.
|
|
|
Malassezia furfur is a fungus that causes...
A. Tinea nigra B. Tinea versicolor C. White piedra |
B. Tinea versicolor. After sun exposure, folliculitis or patchy skin depigmentation occurs due to Malassezia furfur. Requires lipids to grow.
|
|
|
Exophilia werneckii is a fungus that causes...
A. Tinea nigra B. Tinea versicolor C. White piedra |
A. Tinea nigra. Brown or black macules on palms and soles.
|
|
|
Trochosporon beigelii is a fungus that causes...
A. Tinea nigra B. Tinea versicolor C. White piedra |
C. White piedra. Hair shaft infection.
|
|
|
What is described: Common in tropical areas. Caused by dematiaceous fungi (brown black pigemented), suppurative sinuses, abscesses, granulomas. Synonymous with maduramycosis, madura foot.
A. Chromoycosis B. Mycetomas C. Phaeohyphomycosis D. Sporotrichosis |
B. Mycetomas
infection results in a granulomatous inflammatory response in the deep dermis and subcutaneous tissue, which can extend to the underlying bone. Mycetoma is characterized by the formation of grains containing aggregates of the causative organisms that may be discharged onto the skin surface through multiple sinuses. -webmd Amputation often needed for effective treatment! |
|
|
True or False:
For some subcutaneous mycoses, amuptiation is needed for effective treatment. |
True. For Mycetomas.
Tissue, muuscle, bone, fascia of hands and feet. infection results in a granulomatous inflammatory response in the deep dermis and subcutaneous tissue, which can extend to the underlying bone. Mycetoma is characterized by the formation of grains containing aggregates of the causative organisms that may be discharged onto the skin surface through multiple sinuses. -webmd |
|
|
**KNOW FOR EXAM**
What fungus condition does this describe: dematiaceous (pigmented) fungi. Brown, sepatate, yeast-like cells (SCLEROTIC BODIES). A. Mycetomas B. Chromomycosis C. Phaeohyphomycosis D. Sporotrichosis |
B. Chromomycosis
this is the one that looks "cauliflower like" **KNOW FOR EXAM** |
|
|
This is a subcutaneous mycoses that involves soil saprophytes that are inoculated traumatically.
A. Mycetomas B. Chromomycosis C. Phaeohyphomycosis D. Sporotrichosis |
C. Phaeohyphomycosis
|
|
|
Which looks "cauliflower-like"?
A. Mycetomas B. Chromomycosis C. Phaeohyphomycosis D. Sporotrichosis |
B. Chromomycosis
|
|
|
True or False:
Deep (Systemic) mycoses - classical are all dimorphic fungi. |
True. Means they are yeast at body temp and mold out of body.
|
|
|
Which classical deep mycoses is described:
Tramuatic inoculation (usually a gardener working in a garden and pricks themselves with thorn from roses, etc.) . Alternatively, inhalation of airborne spores is possible. A. Blastomyces dermatitides B. Coccidiodes imitis C. Histoplasma capsulatum D. Paracoccidioides brasillensis E. Sprothrix schenkii |
E. Sprothrix schenkii aka the thing that causes SPOROTRICHOSIS and/or Drunken Gardner Syndrome
|
|
|
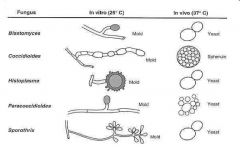
Describe the morphology /histology of each.
A. Blastomyces dermatitides B. Coccidiodes imitis C. Histoplasma capsulatum D. Paracoccidioides brasillensis E. Sprothrix schenkii |
A. Blastomyces dermatitides: Broad-based budding yeast
B. Coccidiodes imitis: Hyphae with arthrospores (individual cells of hyphae) at room temp ; Spherules with endospores (yeast like cells that spread hematogenously) in tissue C. Histoplasma capsulatum: small yeast D. Paracoccidioides brasillensis: thick walled yeast with multiple buds E. Sprothrix schenkii: small yeast |
|
|
This fungus can manifest pulmnoary, cutaneous (can be misdiagnosesd as squamous cell carcinoma), osseous or GI tract infection.
A. Blastomyces dermatitides B. Coccidiodes imitis C. Histoplasma capsulatum D. Paracoccidioides brasillensis E. Sprothrix schenkii |
A. Blastomyces dermatitides
|
|
|
This fungus is diagnosed by the presence of BROAD BASED BUDDING YEAST in clinical specimens.
A. Blastomyces dermatitides B. Coccidiodes imitis C. Histoplasma capsulatum D. Paracoccidioides brasillensis E. Sprothrix schenkii |
Blastomyces dermatitides
|
|
|
For this fungus, what is diagnostic is : Observation of spherules in clinical specimens.
Serology (complement fixation for antibodies, high titers) helpful. Skin test is epidemiologic, not diagnostic tool. Gold standard is to culture, but if you see spherules culture is VERY DANGEROUS and should NOT be done! |
Coccidiodes imitis
|
|
|
Gold standard is to culture, but if you see spherules culture is VERY DANGEROUS and should NOT be done!
Which is the above statement true for? A. Blastomyces dermatitides B. Coccidiodes imitis C. Histoplasma capsulatum D. Paracoccidioides brasillensis E. Sprothrix schenkii |
B. Coccidiodes imitis
|
|
|
Match.
A. SE and Central US B. Ohio and Mississippi River basins C. SW US, Northern Mex, South American deserts D. South, Central American forested regions E. Worldwide 1. Blastomyces dermatitides 2. Coccidiodes imitis 3. Histoplasma capsulatum 4. Paracoccidioides brasillensis 5. Sprothrix schenkii |
1. Blastomyces dermatitides: Endemic in Southereastern and Central US.
2. Coccidiodes imitis: Endemic in Southwestern US, Northern Mexico, South American deserts 3. Histoplasma capsulatum: Ohio and Mississippi River basins 4. Paracoccidioides brasillensis: South, Central American forested regions 5. Sprothrix schenkii: worldwide |
|
|
Name the deep systemic opportunistic mycsoes. (4)
|
Aspergillus species, Candida species, Cryptococcus neoformans, Zygomycetes.
|
|
|
Which of the deep systemic opportunistic mycoses is a huge problem in transplant patients?
|
Aspergillus species
Causes various pulmonary diseases: Allergic bronchopulmonary aspergillus: Clinically represents asthma. Wheezing patient. Problem is airways are colonized with aspergillus and are having an allergic reaction to it! Blood tests will yield: eosinophilia, an increase in IgE. Treat with corticosteroids since it is not an infection but an immunological thing. Fungus ball: growth in pre-existing pulmonary cavity (sarcoidosis, TB, emphysema). Aspergillosis: Invasive pulmonary disease Neutropenia (leukemia, bone marrow transplant) High doses of corticosteroids for prolonged periods Primarily pulmonary but may spread hematogenously to brain. Acute rhinosinusitis might also occur --> invasion of vessels, necrosis and black eschar occur. OTHER DISEASES: ENDOCARDITIS: usually occurs post operatively on prosthetic heart valves SKIN, WOUND INFECTIONS: spores contaminate wound, germinate |
|
|
Which of the deep systemic opportunistic mycoses can yield superficial infections, mucosal infections and severe disseminated disease that includes enopthalmitis in 10% of cases?
|
Candida species that cause candidiasis.
|
|
|
What is the most common cause of meningitis in patients with HIV?
|
Cryptococcus neoformans.
Disease in T-cell deficiencies (esp AIDS), occasionally in normal hosts. Has a big wide gelatenous capsule around it. Acquired by inhalation and causes a brief pneumonia. Has meningeal involvement. Associated with pigeon droppings. Acquired by inhalation. |
|
|
Which of the deep systemic opportunistic mycoses can yield rhinocerebral symptoms?
|
Zygomycetes.
Predilection for blood vessel invasion→ischemia, necrosis Rhinocerebral isMost common Poorly controlled diabetics with acidosis (↓ phgocytosis), severe neutropenia, rare in AIDS Spores inhaled into sinus→germinate→invade Devastating, rapid: adjacent bone, blood vessels→brain invasion→ischemic necrosis |
|
|
Aspergillus is characterized by [ non-septate / septate ] hyphae.
|
septate hyphae!
|
|
|
What does it mean to be a dimorphic fungi?
|
Yeast inside body temp; Mold outside body temp
|
|
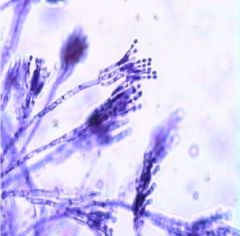
What is this a pic of?
A. Conidia B. Spore C. Septate hyphae D. Non septate hyphae E. Pseudohyphae |
A. Conidia
|
|

What subcutaneous fungal infection is this?
|
Mycetoma
Involve tissue, muscle, bone, fascia of hands and feet Dematiaceous fungi Suppurative sinuses, abscesses, granulomas Contain granules of varying colors (colonies) Synonyms: maduramycosis, madura foot Amputation is often needed for effective treatment. |
|

What subcutaneous fungal infection is this?
|
Chromoblastomycosis
Caused by dematiaceous (pigmented) fungi Tropical, subtropical areas VERRUCOUS (CAULIFLOWER-LIKE) dermatitis Histology: brown, septate, yeast-like cells (SCLEROTIC BODIES) |
|
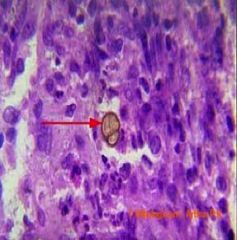
With this histological finding, what is the diagnosis?
|
This is a sclerotic body, thus points to chromomycosis.
|
|
What does this histological finding indicate for diagnosis?
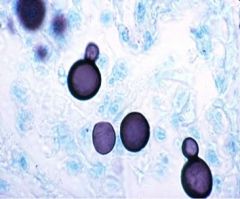
|
Broad based budding yeast in clinical specimens = blastomycosis
|
|
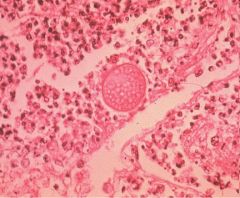
This histological finding indicates which diagnosis?
|
This is a coccidiodes spherule => Coccidioidomycosis
|
|
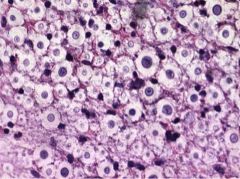
What is this diagnostic of?
|
Cryptococcus
Encapsulated yeast in nature and in tissue Capsule is virulence factor |
|
|
There are four classes of antifungal drugs. _______ binds to ergosterol in the fungal cell membrane and alters membrane permeability.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
A. Polyenes
|
|
|
There are four classes of antifungal drugs. ____ interferes with the synthesis of membrane ergosterol leading to altered membrane permeability; also buildup of toxic sterols.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
B. Azoles
|
|
|
There are four classes of antifungal drugs. ____ inhibits synthesis of beta-D-glucan which leads to disruption of cell wall which leads to cell death.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
C. Echinocandins
|
|
|
There are four classes of antifungal drugs. ____ interfere with the synthesis of lanosterol, a precursor of ergosterol, by inhibiting squalene epoxidase.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
D. Allylamines
|
|
|
This drug's IV form is amphotericin and its topical form is nystatin. It is highly effective against many species but has high incidence of toxicity.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
A. Polyenes
|
|
|
This drug is a teratogenic mutagenic pregnancy category C drug and has many drug-drug interactions. This has 1st and 2nd generation types that work topically and systemically, respectively.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
B. Azoles
|
|
|
This is the newest class of antifungal drugs and has limited resistance, minimal toxicity and no interaction wtih Cyp 450 enzymes. The downside, though, is that it is only available IV.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
C. Echinocandins
|
|
|
This works because squalene buildup is toxic.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
D. Allylamines
|
|
|
Describe briefly how each class of antifungal drug works.
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
A. Polyenes: bind to ergosterol in fungal cell membrane and alters membrane permeability --> fungicidal
B. Azoles: interferese with synthesis of ergosterol leading to altered membrane permeability AND buildup of toxic sterols. Has 1st and 2nd generation. C. Echinocandins: newest class. inhibits synthesis of beta-D-glucan, disrupting cell wall synthesis and leading to cell death D. Allylamines: interferes with synthesis of lanosterol, a precursor of ergosterol, by inhibiting squalene epoxidase |
|
|
Terbinafine (Lamisil) is [ what type of class ] that is used to treat
A. Candidiasis B. Cryptococcosis C. Onychomycosis |
allylamine- interferes with synthesis of lanosterol, a precursor of ergosterol, by inhibiting squalene epoxidase
C. Onychomycosis |
|
|
What class of antifungal drug interferes with synthesis of lanosterol, a precursor of ergosterol, by inhibiting squalene epoxidase?
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
D. Allylamines
|
|
|
What class of antifungal drug interferes with synthesis of membrane ergosterol leading to altered membrane permeability; also buildup of toxic sterols?
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
B. Azoles
|
|
|
What class of antifungal drug inhibits synthesis of beta-D-glucan --> disrupts cell wall synthesis --> cell death?
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
C. Echinocandins
|
|
|
What class of antifungal drug binds to ergosterol in the fungal cell membrane and alter membrane permeability?
A. Polyenes B. Azoles C. Echinocandins D. Allylamines |
A. Polyenes
|
|
|
Which antifungal drug is described: [high] in stratum corneum, hair and nails, persists up to 36 weeks after stopping administration?
A. Fluconazole (Diflucan) B. Griseofulvin C. Itraconazole (Sporonox) D. Terbinafine (Lamisil) |
D. Terbinafine (Lamisil)
|
|
|
With regards to systemic dermatophytic infections, which has very little penetration into CSF and which has HIGH CSF levels?
A. Fluconazole (Diflucan) B. Griseofulvin C. Itraconazole (Sporonox) D. Terbinafine (Lamisil) |
VERY LITTLE IN CSF -->
C. Itraconazole (Sporonox) HIGH CSF LEVELS --> A. Fluconazole (Diflucan) |
|
|
True or False:
Fluconazole (Diflucan) has very little CSF penetration though otherwise generally good penetration in general. |
FALSE. This describes Itraconazole! Fluconazole has very high CSF level penetration and thus is good for cryptococcosis!
|
|
|
Of the dermatophytic systemic infection drugs, which is the only one that is metabolised via kidneys and not liver?
A. Terbinafine B. Itraconazole C. Fluconazole D. Griseofulvin |
C. Fluconazole
|
|
|
What are the general side effects for azoles?
|
Many drug-drug interactions, resistance reported, Pregnancy category C, has cardiac effects with many drugs too (prolongs Q/T interval potentially)
|
|
|
Which two antifungal classes are Pregnancy Category C?
|
Azole Itraconazole and Echinocandins Capsofungin, Anidulagunfin, Micafungin
|
|
|
What is the best drug for cryptococcosis and if that doesn't work what is the next best drug?
|
Fluconazole, then Voriconazole
|
|
|
Voriconazloe is indicated for use in...
|
invasive aspergillosis, and as a backup drug for cryptococcus if it is resistant to Fluconazole.
Note: Side effect is typical azoles + photosensitivity |
|
|
What drug is described: is a VERY TOXIC drug! RENAL TOXICITY and INFUSION REACTIONS common as are hypokalemia, anemia and shock. Liposomal preps help lower renal toxicity. To thwart likelihood of infusion reactions, pretreat with antihistamines or anti-inflammatory drugs.
|
Amphotericin B
So why use if so horrible? *has been around for a LONG time and is very well studied *used for SEVERE stystemic fungal infections *used as an induction agent or as backup if treatment is not working *CAN BE USED ON PREGNANT WOMEN! :) Sometimes flucytosine is given for synergistic effect. |
|
|
Which antifungal drug is described: [high] in stratum corneum, hair and nails, persists up to 36 weeks after stopping administration?
A. Fluconazole (Diflucan) B. Griseofulvin C. Itraconazole (Sporonox) D. Terbinafine (Lamisil) |
D. Terbinafine (Lamisil)
|
|
|
With regards to systemic dermatophytic infections, which has very little penetration into CSF and which has HIGH CSF levels?
A. Fluconazole (Diflucan) B. Griseofulvin C. Itraconazole (Sporonox) D. Terbinafine (Lamisil) |
VERY LITTLE IN CSF -->
C. Itraconazole (Sporonox) HIGH CSF LEVELS --> A. Fluconazole (Diflucan) |
|
|
True or False:
Fluconazole (Diflucan) has very little CSF penetration though otherwise generally good penetration in general. |
FALSE. This describes Itraconazole! Fluconazole has very high CSF level penetration and thus is good for cryptococcosis!
|
|
|
Of the dermatophytic systemic infection drugs, which is the only one that is metabolised via kidneys and not liver?
A. Terbinafine B. Itraconazole C. Fluconazole D. Griseofulvin |
C. Fluconazole
|
|
|
What are the general side effects for azoles?
|
Many drug-drug interactions, resistance reported, Pregnancy category C, has cardiac effects with many drugs too (prolongs Q/T interval potentially)
|
|
|
Which two antifungal classes are Pregnancy Category C?
|
Azole Itraconazole and Echinocandins Capsofungin, Anidulagunfin, Micafungin
|
|
|
What is the best drug for cryptococcosis and if that doesn't work what is the next best drug?
|
Fluconazole, then Voriconazole
|
|
|
Voriconazloe is indicated for use in...
|
invasive aspergillosis, and as a backup drug for cryptococcus if it is resistant to Fluconazole.
Note: Side effect is typical azoles + photosensitivity |
|
|
What drug is described: is a VERY TOXIC drug! RENAL TOXICITY and INFUSION REACTIONS common as are hypokalemia, anemia and shock. Liposomal preps help lower renal toxicity. To thwart likelihood of infusion reactions, pretreat with antihistamines or anti-inflammatory drugs.
|
Amphotericin B
So why use if so horrible? *has been around for a LONG time and is very well studied *used for SEVERE stystemic fungal infections *used as an induction agent or as backup if treatment is not working *CAN BE USED ON PREGNANT WOMEN! :) Sometimes flucytosine is given for synergistic effect. |
|
|
True or False:
Sometimes flucytosine is given for synergistic effect. |
True
|
|
|
Echinocandins like Caspofungin, Anidulagunfin, Micafungin, Azoles like Itraconazole, Fluconazole, Voriconazole, Posaconazole and Amphotericin B are all used for...
A. drugs used in treating deep/systemic fungal disease B. drugs used for systemic dermatophytic infections |
A. drugs used in treating deep/systemic fungal disease
|
|
|
This drug is used in prevention of Candida and Aspergillus in severely immunocompromised patients.
|
Posaconazole
|