![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
68 Cards in this Set
- Front
- Back
|
Life-threatening causes of chest pain |
Acute ACS |
|
|
Anterior leads |
V2-V5 |
|
|
Lateral leads |
V5, V6, aVL |
|
|
Inferior leads |
II, III, aVF |
|
|
Immediate treatment for STEMI |
Morphine 5-10mg IV; |
|
|
Early complications of MI |
Mechanical - Papillary muscle rupture, ventricular-septal rupture, free wall rupture Arrhythmias - brady / tachy |
|
|
Late complications of MI |
Pericarditis |
|
|
Medical management for NSTEMI |
Pain control |
|
|
Discharge meds after ACS |
aspirin 75mg/d |
|
|
NICE treatment pathway for hypertension step 1 |
Under 55 years: ACEi or ARB |
|
|
adverse effects of thiazides |
Excessive diuresis |
|
|
Adverse effects of ACEi |
cough |
|
|
adverse effects of beta-blockers |
Cold extremities, paraesthesia, numbness at peripheries (more common if peripheral vascular disease) |
|
|
Risk factor modification for stable angina |
lifestyle modification |
|
|
Symptom control for stable angina |
GTN, calcium channel blocker, β-blocker, long-acting nitrate (isosorbide mononitrate), consider cardiac revascularisation if uncontrolled |
|
|
4 causes of LV failure |
Ischaemic heart disease (70%) |
|
|
causes of right heart failure |
chronic LV failure chronic lung disease recurrent PE Atrial septal defect |
|
|
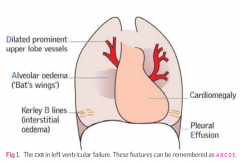
Common findings of heart failure on CXR |
|
|
|
New York Heart Association (NYHA) Functional Classification of heart disease |
I No limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, dyspnoea |
|
|
4 drugs for symptomatic management of heart failure |
Furosemide |
|
|
Drugs to avoid in heart failure |
Calcium channel blockers |
|
|
Symptoms of AF |
Fast, irregular palpitations |
|
|
Causes of AF |
Ischaemic heart disease Mitral valve disease |
|
|
Basic management of AF |
Rate control Anticoagulation |
|
|
Rate control drugs for AF |
Beta-blocker - metoprolol |
|
|
Rhythm control for AF |
Acute (<48 hours) - DC cardioversion Chronic (>48 hours) - 3 weeks warfarin then DC cardioversion Persistent AF: amiodarone, sotalol or ablation |
|
|
CHAADSVAS score for stroke risk |
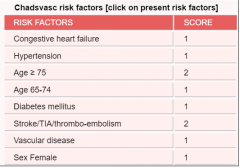
Score of 1 → consider anticoagulation |
|
|
Options for anticoagulation in AF |
heparin + warfarin or apixaban |
|
|
Types of narrow complex tachycardia (SVT) |
Sinus tachycardia Sinusnode re-entry (rare) atrial flutter atrial tachycardia atrial fibrillation AVNRT AVRT - WPW |
|
|
causes of broad complex tachycardia |
Ventricular tachycardia (VT) - 80% [95% if ACS] SVT with BBB |
|
|
management of SVT |
Carotid sinus massage |
|
|
what does adenosine do? |
blocks the AVN |
|
|
medical management of stable VT |
IV amiodarone 300mg over 20-60 mins via a central line then IV amiodarone 900mg over 24 hours |
|
|
causes of complete heart block |
idiopathic fibrosis (most common) Infective endocarditis amyloidosis, sarcoidosis |
|
|
1st degree heart block on ECG |
prolonged PR interval |
|
|
Mobitz type 1 (Wenckebach) on ECG |
progressive prolongation of the PR interval on consecutive beats followed by a blocked P wave (i.e., a 'dropped' QRS complex). After the dropped QRS complex, the PR interval resets and the cycle repeats |
|
|
Mobitz type 2 on ECG |
intermittently non-conducted P waves not preceded by PR prolongation. There is usually a fixed number of non-conducted P waves for every successfully conducted QRS complex,and this ratio is often specified in describing Mobitz II blocks e.g. 2:1 |
|
|
3rd degree heart block on ECG |
no association between p waves and QRS |
|
|
Which types of heart block require active management? |
Mobitz II and 3rd degree |
|
|
Causes of LV outflowtract obstruction |
Sub-valvular e.g. hypertrophic cardiomyopathy (HCM) |
|
|
Symptoms of aortic stenosis |
SAD: Syncope Angina Dyspnoea heart failure (usually after age 60) |
|
|
Signs of aortic stenosis |
Slow rising pulse with narrow pulse pressure |
|
|
causes of aortic stenosis |
Senile calcication |
|
|
symptoms of mitral regurgitation |
Dyspnoea |
|
|
Signs of mitral regurgitation |
AF |
|
|
Mechanisms of mitral regurgitation |
Annulus problem (annulus = fibrous ring surrounding the valve) - due to dilated LV or annular calcification (elderly) |
|
|
symptoms of tricuspid regurgitation |
Fatigue |
|
|
Signs of tricuspid regurgitation |
Giant v waves and prominent y descent in JVP |
|
|
causes of pericarditis |
1. virus (typically coxsackie) |
|
|
Clinical features of pericarditis |
Central chest pain worse on inspiration or lying at ± relief by sitting forward |
|
|
pericarditis on ECG |
ECG classically shows widespread concave (saddle-shaped) ST segment elevation, but may be normal or non-specific (10%) |
|
|
immediate therapy for confirmed DVT |
Start LMWH, fondaparinux or UFH as soon as possible and continue it for at least 5 days or until the INR is ≥2 for >24 hours, whichever is longer |
|
|
maintenance therapy after DVT |
Offer warfarin to patients with confirmed proximal DVT within 24 hours of diagnosis and continue warfarin for 3 months. At 3 months, assess the risks and benefits of continuing warfarin treatment |
|
|
Arterial disease on ABPI |
1.0-1.2 = normal |
|
|
features of critical ischaemia |
Rest pain - typically occurs when leg is horizontal in bed; patient sleeps with leg hanging out of bed |
|
|
features of acute limb ischaemia |
Pain Pallor Pulselessness Paraesthesia Paralysis Perishingly cold |
|
|
indications for AAA surgery |
AAA of ≥ 5.5 cm should be repaired electively |
|
|
Signs of chronic venous insufficiency |
Oedema |
|
|
treatment for varicose veins |
foam sclerotherapy |
|
|
Clinical features of carotid artery disease |
Amaurosis fugax |
|
|
Causes of hypertension |
1. Primary/Essential hypertension (95%) of 2. Secondary hypertension (5%) A. Renal disease - intrinsic renal disease & renovascular disease B. Endocrine disease - Cushing’s and Conn’s, phaeochromocytoma, acromegaly C. Drugs: steroids, MAOI, OCP, NSAIDs D. Others: Coarctation, pregnancy, sleep apnoea |
|
|
Indications for CABG on angiography |
Left main stem disease Triple vessel disease For unresolving unstable angina and NSTEMI, if PCI unsuccessful |
|
|
tests for monitoring amiodarone |
6 monthly TFTs and LFTs |
|
|
treatment for acute limb ischaemia |
1. Embolectomy 2. localised thrombolysis 3. Amputation |
|
|
Indications for Aortic valve replacement |
Severe aortic stenosis ( transvalvular gradient of>40mmHg) Severe AS and LVEF <50% Patients with AS undergoing other cardiacsurgery (e.g. CABG) Symptomatic AS, especially if clear causeof angina, syncope and HF |
|
|
signs of aortic regurgitation |
wide pulse pressure, displaced, hyperdynamic apex beat, early diastolic murmur, collapsing pulse |
|
|
management of acute heart failure |
Sit patient up, high flow give O2 Get access, ECG, CXR, ABG, sats IV 40-80mg furosemide - repeat at 30-60 mins Consider slow IV morphine IV isosorbide or glyceryl trinitrate, titrated to BP Refer to seniors and ITU for IV inotropes or CPAP or invasive ventilation |
|
|
causes of acute limb ischaemia |
1. thrombosis formation (60%) - pre-existing peripheral artery disease, dehydration, hypotension, malignancy, polycythaemia, prothrombotic state 2. Embolism (30%) - AF, post MI, prosthetic valves, from aneurysms 3. Other (10%): aortic dissection, trauma, iatrogenic injury, thrombosed aneurysm, thrombosed graft, extreme cold |