![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
16 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
1. List 7 Germ cell tumors of the mediastium? |
1. chorioCA Embryonal Germinoma Benign teratoma Malignant teratoma Yolk sac tumor Mixed GCT |
|
|
|
1. List 10 tumors of mediastium? |
1. ganglioma MPNST Mediastinal ependymoma neuroblatoma Ganglioneurobalstoma neurofiroma/neurofibromatosis paraganglioma pigmented neuroectodermal tumor of infancy primitive neuroectodermal tumor schwannoma |
|
|
|
1. List 3 thymic lesions? 2. List 4 branchial pouch differentations and one form of mediastinal fibrosis? |
1. thymoma, thymic CA, thymic carcinoid 2. carcinoma showing thymus like elements (CASTLE), ectopic cervical thymoma, ectopic hamartomatous thymoma, spindle epithelial tumor with thymus like elements (SETTLE); sclerosing mediastinitis |
|
|
|
1. From where is mesotheliuma derived? 2. patient population ? 3. What is linked epidemilogically w/ mesothelioma? list most common to least? 4. What is the time frame of exposure to carcinogen and development of mesotheliom? 5. most common locations? 6. What do mesotheliumas produce? |
1. the mesothelium cells that line serous cavities 2. 75% in men age 50-70yrs 3. asbestos: crocidolite > chrysotile and amosite; NO link to smoking! 4. 35 years on average 5. pleura 65-75% peritoneum 25% pericardium 2% and tunica vaginalis of testis 6. interleukin 6 |
|
|

|
malignant mesothelioma 1. w/ the peritoneal versions what is important about patient presentation? 2. List histologic types and variants |
1. 50% w/ mets to abdominal nodes AT presentation 2. epithelial (epithleioid and tubulopapillary), sarcomatous, desmoplastic, biphasic (mixed), poorly diff (undiff), deciduoid peritonieal, clear cell, lymphohistiocytoid, small cell, in situ, well diff papillary, MM of tunica vaginalis, localized, |
|
|
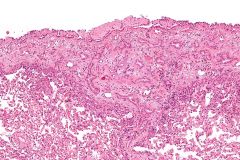
epithelioid malignant mesothelioma 1. histo? |
1. epithelial usually tubulopapillary and often cuboidal flattened w/ adicophlic cytoplasm uiform vesicular nuclei w/ prominent nucleoli, may form solid sheets of plump polyhedral cells |
|
|
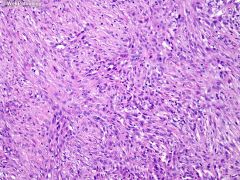
sarcomatoid mesothelioma 1. what are the definitions of spindled and desmoplastic variants of mesothelioma? 2. describe histology? 3. what does myxed or biphasic mesothelioma resemble? |
1. spindled needs >90% spindled tumor cells and desmoplasia must be in >50% of tumor cells to call variant 2. spindled or oval neoplastic cells arranged in numerous patterns, but not usually fasicles, may contain osteoid or cartilage; desmoplastic mmay appear identical to reactive pleural fibrosis so dx needs invasion of chest wall or necrosis to call 3. synovial sarcoma! |
|
|
1. Describe poorly diff mesothelioma? 2. how common are variatns in pleural vs peritoneal spaces? 3. What is different abou the well diff papillary variant? 4. What's different about deciduoid variant? |
1. sheets of polygonal tumor cells w/marked nuclear pleomorphism, 2. pleural is 50% epithelial, 25% biphasic, 15% sarcomatous and 10% poorly diff while in the peritonium 75% are epithelial and sarcomatous is rare 3. it has intermediate malignant potential, usually seen in peritoneum of 30-40yr old women, w/ multiple peritoneal nodules w/ well developed tubulopapillary pattern 4. Also affects young women, has no relationship w/ asbestos exposure |
|
|
|
1. what special stain can be used to differentiate mesothelioma from adenocarcinoma? 2. how do mesotheliomas stain w/ keratins? 3. What other stains can be used to diff ACA from mesothelioma? 4. Prognosis of mesothelioma? |
1. mucicarmine 2. they are positive for low more than high molecular wight keratins 3. CEA + 75-100% ACAs, CD15 aka LEUM1 + 60-100% ACAs, BerEP4 + 85% ACAs, ACAs also posiivr for B72.3, MOC31 TTF1 Napsin A; Mesotheliomas are positive for p53 and 75-95% + for calretinin 4. horrible w/ 15-35% 3 year survival rate |
|
|
|
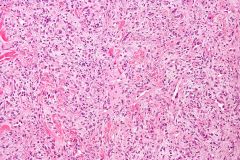
solitary fibrous tumor 1. patient population and presentation? 2. gross? 3. histology? 4. What histology suggets malignancy? 5. IHC? 6. Prognosis? 7. What is essenitally the same as an SFT? also? |
1. may happen in kids but usually b/w 4-7 decades, women sligntly more common, often asymptomatic, may have chest pain couch dyspnea, digital clubbign and fever; 5% of large tumors have pleural effusion and/or hypoglycemia 2. 65% are attached to visceral pleura, 35% arise from parietal diaphragmatic or mediastinal pleura 3. bladn spindled cells w/ variable arrangment "patternless patter", prominent areas of hyalinization, areas w/ increased cellularity, variable vasculature 4. >4 mits /10 HPF and fascicles like in fibrosarcoma 5. 90-95% + CD34 and 70%+ CD99, but are keratin and S100 neg 6. most are benign 7. hemangiopericytoma and share features w/ lipomatous hemangiopericytoma and giant cell angiofibroma |
|
|
1. what germ cel tumors can grow in the mediastinum? 2. how are germ cell tumors tx? 3. With what syndrome are mediastinal GCTs assoc? 4. What malignancies can be synchronous w/ these tumors? 5. What malignancies have occured s/p tx for this? |
1. benign mature or immature teratomas, malignant teratoma (due to malignant germ or non-germ cell tumors, or immature teratoma can met), germinoma, embryona CA, YST, Chorio CA, Mixed germ cell tumor 2. non seminomatous GCTs tx w/ intensive chemo and poor risk pts also follow up w/ BM transplant 3. 4. Klinefelter, 47XXY, get mediastinal GCTs 30-40x MORE than general population 4. malignant histiocytosis, anaplastic large cell lymphoma, AML 5. AML, megakaryocytic leukemia and AMML |
|
|
|
choriocarcinoma 1. patient pop and presentatin? 2. Histo? 3. IHC? |
1. equal in sexes present w/ elevated Beta HCG, men w/ gynecomastia 2. mix of syncitio and cyto trophoblasts and hemorrhage can mixed w/ any other GCT 3. CK +, syncitios (and some cytos) always Beta HCG positive |
|
|
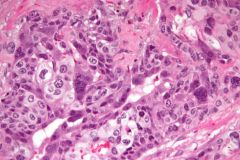
embryonal carcinoma 1. presentation? 2. histo? 3. IHC? |
1. elevated afp diagnostic; almost always widely invasive and UNresectable at dx 2. sheets tu bules papillary structures of large polygonal cells w/ prominant nucleoli pale cytoplasm indistinct borders, frequent mits 3. tumor cells react to PLAP, CK, CD30; 1/3 positive for AFP also |
|
|
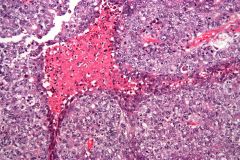
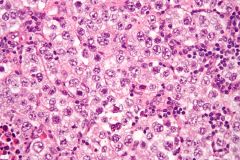
germinoma 1. patient population? 2. histology? 3. IHC? 4. tx and prognosis? |
1. men > women (rare) b/w 2nd and 4th decades 2. sheets of large polygonal cells w/ distinct cell membranes, clear or finely granular cytoplasm and round partly flat nucleus w/ 1+ prominent nucleoli, in loose stroma infiltrated by lymphocytes or 50-60% w/ granulomatous inflammation 3. NEG for CK, EMA POS PLAP CD117 (ckit) 4. curable when tx w/ sx + aduvant radiotherapy for mediastinal dz, and cysplatin based chemo for mets, 80% long term survival |
|
|
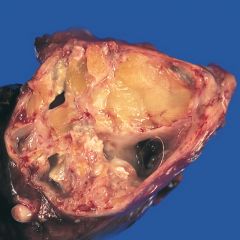
benign teratoma 1. What is the most freequent site? 2. patient population w/ most common teratoma type? 3.histo for mature and immature benign teratomas? 4. Tx and prognosis? |
1. anterior mediastinum w/in or adjacent to thymus gland 2. mature account for 75% usually in adolescents; in women all GCTs are mature teratomas often cystic; immature (pure and mixed) more common in kids/teens 3. mature: abnormal mix of tussues frome 2-3 embryonic layers, (most to least common) usually skin w/ appendages, bronchial tissue, GI, smooth muscle fat, bone cartilage, exocrine/endocrine pancrease, salivary gland, CNS, protate, hepatocytes immature: tissue from all 3 germ layers present, in various stages of maturation from embryonic to fetal 4. mature is benign and tx w/ sugical removal, immature w/ malignant GCT component tx w/ debulking and aduvant radiochemotherapy, some cases cured |
|
|
1. patient population and presentation for malignant teratomas? 2. Histology? 3. What can happen after tx to diff components? |
1. exclusively in males (along w/ malignant GCTs) w/ cough dyspnea chest pain fatigue and weight loss 2. malignant compoent of teratoma usually mesenchymal much more than carcinoma, (can be in mature of immature) rhabdosarcoma, angiosarcoma, liposarc, chondrosark, leiomyosark, glioblatoma, neuroblasoma, nephroblastoma, adenosquamous CA 3. the GCT disappears completely and the carcioma or mlignant mesenchymal component survives and is left behind (tx is radio/chemo after debulking and BM follows in poor risk patients) |
|