Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
120 Cards in this Set
- Front
- Back
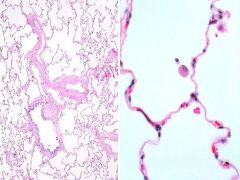
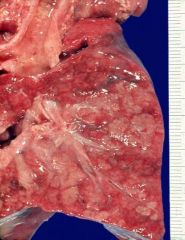
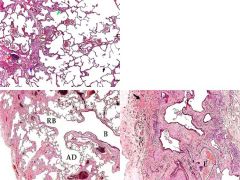
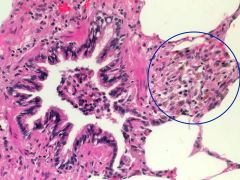
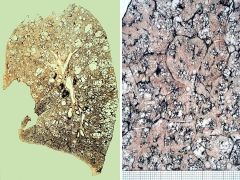
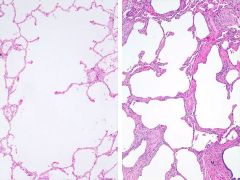
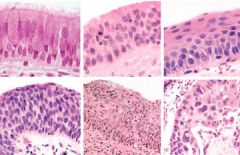
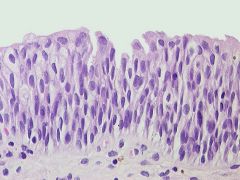
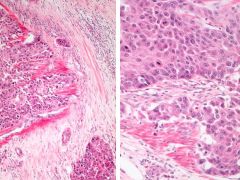
What's pictured? What is in the middle of the white space in the image on the right?
|
Normal Lung
• Macrophage in an alveoli • Ddx: Normal lung parenchyma. • Description: Thin alveolar septa are lined by flat type I pneumocytes and contain a thin-walled capillary. Occasional alveolar macrophages are a normal finding. • Stain: HE. |
|
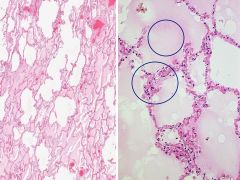
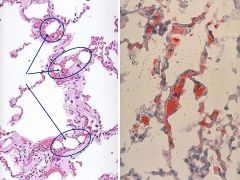
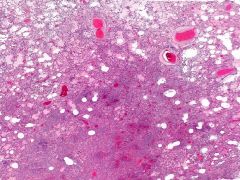
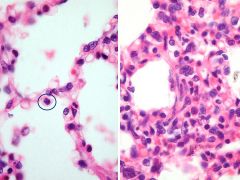
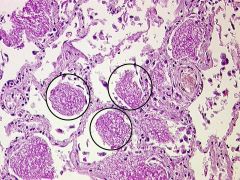
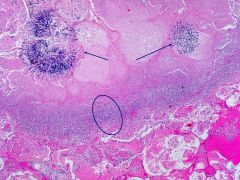
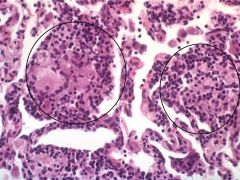
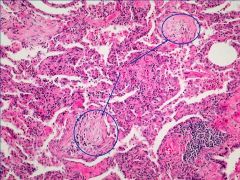
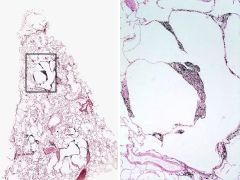
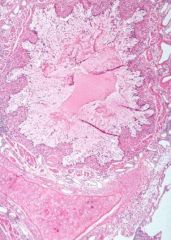
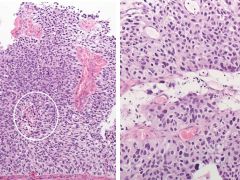
What is pictured?
• What is in the uppermost circle on the right slide? • What is in the lower circle on the right slide? |
• Acute pulmonary edema and passive congestion.
• The edema/exudate has NO PMNs. It does have protein, and by definition > 3g/dL (Transudate has < 3g/dL, or low protein content) |
|

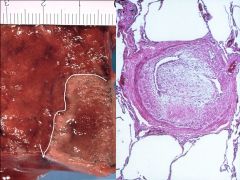
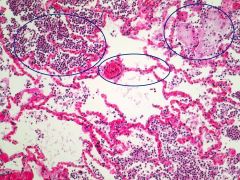
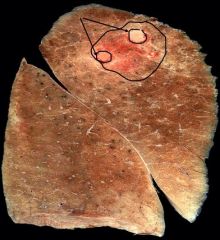
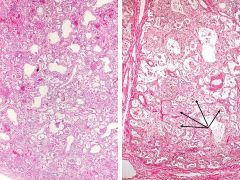
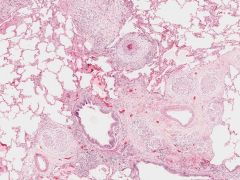
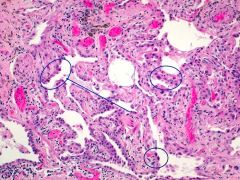
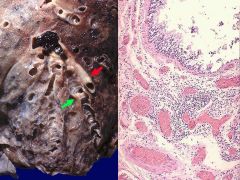
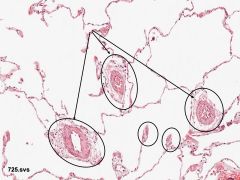
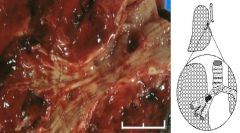
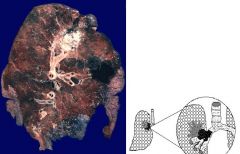
What is pictured on the left? What is in the circle?
What is pictured on the right? What is the color due to? What process is this the result of? |
Normal lung, w/ carbon in the peribronchovasicular lymphatics
Dark lung, Brown indurated lung: • due to hemosiderin containing macrophages in the alveoli (engulfment of RBCs) • result of chronic congestion |
|
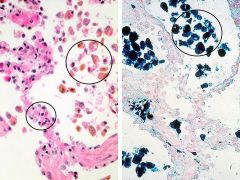
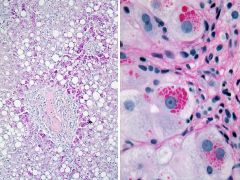
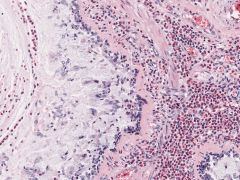
What is pictured?
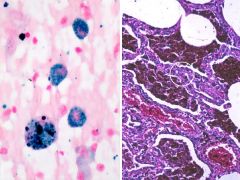
On the left what is in the small circle? What is in the larger circle? What stain is used on the right? What does it stain for? |
Chronic congestion of the lung.
• Thickened septa • Hemosiderin-containing macrophages "heart failure cells" • Prussian blue stain on the right • Stains for iron |
|

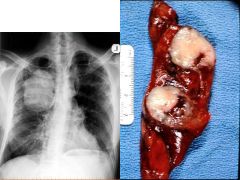
What is pictured? How did it occur?
What are the symptoms? What is the prognosis? |
Pulmonary Thromboembolus
*Thrombus is old, the embolus is new* • Typically occur from thrombi originating in the deep veins of the legs. Those immobilized for a long time are at greatest risk. • Present with sudden SOB • Prognosis is poor (if embolus is this size and blocking a main pulmonary artery) death possible w/in minutes |
|
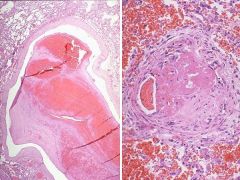
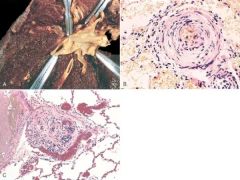
What is pictured on the left? How do you know? What distinctive feature is shown?
What is pictured on the right? How do you know? |
Left: Pulmonary Embolus in a larger P. artery.
• Know that it is a new embolus because it is not attached to the side of the vessel. Fibroblasts will invade an old embolus in attempts to vascularize and organize it. • Key feature = lines of Zahn Right: A partially recanalized PE in a small peripheral P. artery. • Can tell it is old because it is being organized. • Could lead to pulmonary HTN. |
|

What is pictured on the left? Why does it appear this way?
What is pictured on the left? |
Pulmonary infarct
• Hemorrhagic because of the dual blood supply from the non-occluded bronchial arteries which continue to supply blood, but do not prevent the infarction On the left: An organizing infarct w/ pleural reaction. |
|
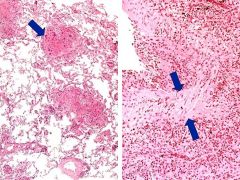
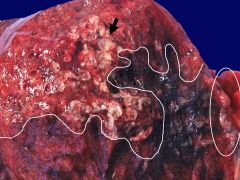
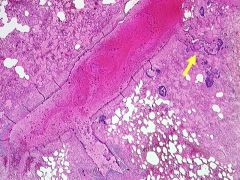
What is pictured on the left? What does the line around the whitish area represent? What is the white arrow pointing to?
What is pictured on the right? What characteristic of the patient may have caused this to occur? |
Left: Organizing Pulmonary infarct
• Fibrotic border (white line) • Thicked pleura (arrows) Right: Partially recanalized thromboembolus in P. artery branch. ***This patient has a coagulopathy - Factor V Leiden - predisposing him to clots. |
|
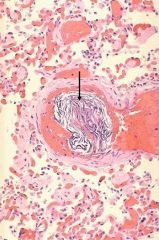
What is pictured on the right? How can you confirm this diagnosis?
In what situations would this occur? |
Fat embolism
• Use Oil Red stain: demonstrates the fat globules within the pulmonary arterioles. The globules stain reddish-orange. • Fat embolism syndrome is most often a consequence of trauma with *long bone fractures*. It can also be seen with extensive soft tissue trauma, burn injuries, severe fatty liver, and very rarely with orthopedic procedures. |
|
What is pictured? How might this occur? What is the presentation?
|
Amniotic fluid embolism
• A rare complication • Seen at term during or shortly after labor • Amniotic fluid may gain access to uterine veins following a tear in the placental membranes and embolize to the lungs • Presents w/ acute dyspnea w/ cyanosis & shock. Sudden death. |
|
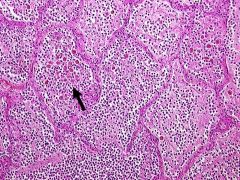
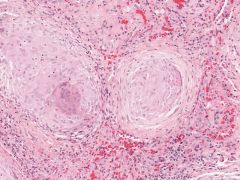
What is pictured in A? In B? In C?
|
Pulmonary HTN
Summary of vascular changes: A. Atheromatous streaks in large pulmonary arteries (does not occur in pts w/ atherosclerosis - only if they also have pulmonary HTN) B. Medial hypertrophy C. Plexiform lesions in severe pulmonary hypertension (red globules) |
|
What is pictured on the left? What are the dark circles?
What is pictured on the right? What is the white circle indicating? |
Left: Bronchiolar Lavage of DAD (Diffuse Alveolar hemorrhage, or ARDs)
• Dark structures = hemosiderin laden macrophages suggesting previous bleeding (black dots = carbon) Right: Alveoli are filled w/ blood and hemosiderin-laden macrophages • White circle: Thickened alveolar septa |
|
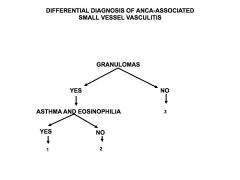
What is 1? What is 2? What is 3?
Which of these diseases may also present in the kidney? |
1. Churg-Strauss (asthma-eosinophil related)
2. Wegners (can present in the kidney) 3. Microscopic polyangitis |
|
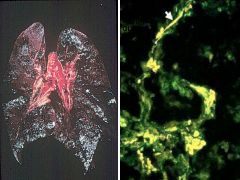
What is pictured on the left? Why the dark color? What has this disease progressed to? Where else might this disease present? What is the typical patient presentation?
What is pictured on the left? Why such a pattern? |
Goodpastures disease
• Dark lungs full of blood hemosiderin • Progressed to DAH (Diffuse Alveolar hemorrhage) • May present in the kidney • Typical presentation is young boys Left: • Immunofluorescene of Anti-basement mb Ig. • Linear pattern |
|

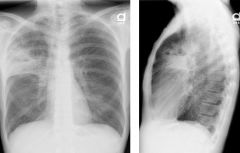
What disease is shown on the left? What are the arrows pointing to?
|
Wegner's Granulomatosis
• Showing multiple cavitary lesions • The arrow is indicating the fluid level in the cavity |
|
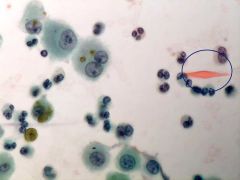
What type of slide is this? What disease presentation? What is in the circle? Where did it come from?
|
Bronchio-lavage of Churg-Strauss Vasculitis
• Charcot-leyden crystal • It is crystalized cytoplasmic protein from eosinophils |
|
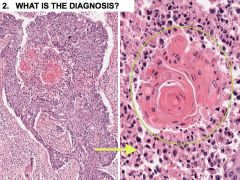
What disease is shown? What is in the history that is relevant? What might a CBC show?
What is the arrow on the left pointing to? What types of cells are in there? What inflammatory cells are likely present? What is the arrow on the right pointing to? What cells are infiltrating? |
Churg-Strauss allergic granulomatosis and angiitis.
Clinical features: • History of asthma and allergic rhinitis. • CBC shows peripheral hypereosinophilia, anti-mpo +(<50% of cases). Left: Necrotizing granulomatous angiitis affecting small and medium-sized pulmonary arteries. • Inflammatory cells = eosinophils. • Dark dots are multinucleated giant cells. Right: A medium-sized pulmonary artery shows destructive angiitis. • The inflammatory cells in the intima, media, and surrounding tissue are mainly eosinophils. The arrows mark the media of the vessel. |
|
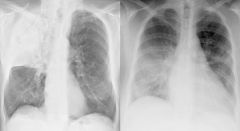
What is pictured on the left? What is pictured on the right?
|
• Lobar pneumonia in RUL
• Bilateral bronchopneumonia |
|

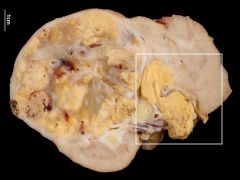
What is pictured? What stage is this?
|
Lobar pneumonia of the lung
• Red hepatization Diagnosis: Lobar pneumonia: red hepatization. Description: Cut surface of the affected lobe is dense, airless and homogeneously red. Comment: The second day of lobar pneumonia. |
|

What is pictured? What stage?
|
• Lobar pneumonia
• Gray hepatization Diagnosis: Lobar pneumonia: grey hepatization stage. Comment: Day 4.-6. of pneumococcal pneumonia. |
|
What is pictured? What stage? What is the arrow pointing to? What is filling the alveoli???
|
• Lobar pneumonia
• grey hepatization. • Arrow: siderophages (hemosiderin-containing macrophages) • All alveoli are filled with fibrin, edema and ****neutrophils**** Additional findings: Pleuritis. Clinical findings: Heavy smoker and alcoholic. Stain: HE. |
|
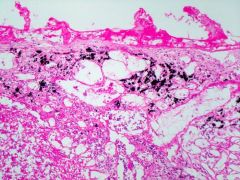
What is pictured? What is on the pleural surface? What clinical findings may be present? What is in the subpleural lymphatics?
|
Lobar pneumonia w/ fibrinous pleuritis
• Fibrin on pleural surface • May hear a pleural rub (once there is more fluid, you will not hear that) • Carbon |
|
What is pictured?
How can you tell? |
• Diagnosis: Severe bronchopneumonia.
• Description: Several grayish-yellow infiltrates that are becoming confluent. |
|
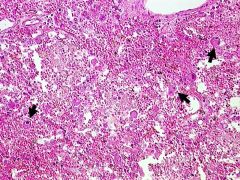
What is pictured? How will the patient present?
|
Acute bacterial pneumonia.
• Edema and congestion and pneumonic infiltrates. • Clinical findings: Abruptly beginning symptoms with high fever, shaking chills, productive cough, general malaise, air hunger, cyanosis, pain when breathing, and leukocytosis. Comment: Because of antibiotics, the classic stages of lobar pneumonia are seldom seen. Microscopically lobar pneumonia and bronchopneumonia look the same. It is more important to identify the causative agents. Stain: HE. |
|
What is shown? What classic features are shown?
What is the left most circle? Middle? Right? |
• Acute bacterial pneumonia. ****Hyperemia, edema, neutrophilic granulocytes in alveoli****
Left = PMNs in alveoli Middle = hypermia Right = edema |
|

What two conditions are pictured? What can predispose a pt to this condition?
|
Aspiration pneumonia w/ abscess (+ empynema, pus in pleural cavity) AND a pulmonary emobolus
What predisposes a pt to pneumonia? • Any kind of viral infection • In surgery, pts can aspirate there stomach contents. • Alcoholics • Pts w/ seizure disorders Predisposed to emboli by? • Being sedentary. After a pt is in the hospital you want them to be ambulating to get things moving and also to prevent the emboli |
|
What is the white border indicating? What is the circle showing?
|
• Pneumonia with abscess formation.
• Circle shows emphysematous blebs Additional findings: lung emphysema. |
|
What is pictured? What is the yellow arrow pointing to?
|
• Septic embolus.
• Blue masses of bacteria in a branch of the pulmonary artery. The surrounding lung is edematous. Additional findings: Several septic emboli in both lungs. Coagulase positive Staphylococcus grew from blood and pericardial fluid. Clinical findings: Patient lanced a boil in his own axilla and died of staphylococcal sepsis 10 days later. Stain: HE. |
|
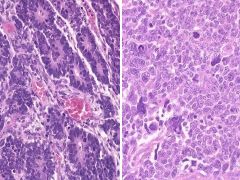
What is pictured? What is distinct about the cells on the left? What is indicated by the circle?
What is pictured on the right? What can this progress to? |
Left: Viral pneumonia with mild interstitial edema and swollen alveolar lining cells.
• The swollen alveolar lining cells is distinct in VIRAL pneumonia (not seen in bacterial pneumonia) • Circle indicates macrophages Right: Widened alveolar septa with mononuclear infiltrates (there must have been some necrosis). • Can progress to DAD/ARDs! |
|
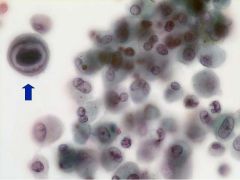
What is pictured? What are the arrows pointing to? What condition allowed this disease to present?
|
• Viral infection, most probably herpes simplex. --> Pneumonia
• Nuclear inclusion bodies - Cowdry type A. • Pt was under immuno-suppression for rapidly progressive glomerulonephritis. Stain: Papanicolaou. |
|
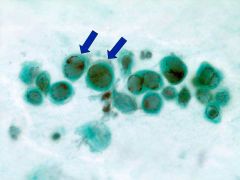
What is pictured? What is the arrow pointing to?
|
Cytomegalovirus pneumonia***
• Arrow: Intranuclear inclusion body with halo (owl's eye). Additional findings: Combined cytomegalovirus- and Pneumocystis carinii infection. Stain: Papanicolaou. |
|
What is being shown? What is the arrow pointing to?
|
Cytomegalovirus pneumonia***
• Arrow: Intranuclear inclusion body with halo (owl's eye). Additional findings: Combined cytomegalovirus- and Pneumocystis carinii infection. Stain: Papanicolaou. |
|
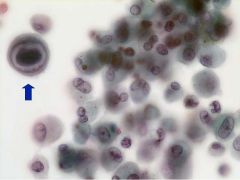
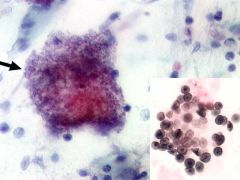
What is the being shown? What are the circles indicating? In what demographic does this tend to present?
|
• Pneumocystis carinii (jiroveci) pneumonia.
• Circles indicate: Conglomerates of organisms in alveoli • Tends to affect HIV & immunosuppressed pts. Description: Granular, foamy PAS positive masses of organisms in alveoli with remarkably little host reaction. |
|
What is being pictured? What is the arrow pointing to? In what demographic does this tend to present?
What is the lower right showing? What kind of stain is being used? |
• Pneumocystis jiroveci pneumonia.
• A mass of pneumocystis jiroveci organisms • HIV & immunosuppressed pts. • Lower right = pneumocysts • Crocott's Silver stain Description: Characteristic foamy and granular lumps in bronchoalveolar lavage fluid. Clinical findings: Bilateral basal interstitial pneumonia. |
|
What is pictured? What is shown in the alveoli? What is the arrow showing?
|
• Cytomegalovirus pneumonia combined with bacterial pneumonia.
• PMNs and blood in the alveoli • Arrow is showing Intranuclear CMV inclusion Description: Severe necrotizing pneumonia; viral intranuclear inclusion bodies. Clinical findings: HIV positive patient for 5 years. At autopsy evidence of CMV was found in brain, lung, GI-tract, kidneys and adrenals. |
|
What is being pictured? Why does it look red?
|
Aspergillus pneumonia
• Can cause a necrotizing granuloma • Looks red because it also tends to be *angioinvasive* |
|
What is being shown? What are the arrows pointing to? What is the circle indicating?
|
• Aspergillosis.
• Arrows - pointing to hyphae (angioinvasive) • Circle: Rim of inflammatory cells surrounding the are of necrosis. • There is also fibrin within the alveolar spaces. |
|

What is pictured? What is the organism? What can this lead to?
|
Invasive aspergillosis.
• Can lead to vascular obstruction and pulmonary infarcts. Diagnosis: Invasive aspergillosis. Clinical findings: Mycotic meningoencephalitis and fungal pneumonia in a patient with metastatic gastric carcinoma. Fungus invades blood vessels |
|
What is being pictured?
|
Coccidiodomycosis w/ cavitary lesion
|
|
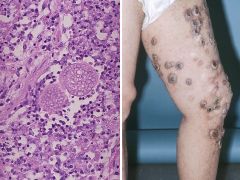
What is pictured on the left? What is pictured on the right?
|
Disseminated coccidiodomycosis.
• Necrotic poorly formed granulomas in lungs and other organs (left) • Necrotic umbilicated skin lesions (right) |
|

What is shown?
|
ARDS/HMD/DAD
|
|

What is pictured? What stage? What are the circles indicating? What cells are likely to be damaged?
|
• DAD, exudative stage. • Circles indicating hyaline membranes are lining alveolar walls.
• Damage to both ****Type I and Type II cells*** Clinical findings: ARDS after induction chemotherapy for stem cell transplantation to treat acute myeloid leukemia. • Mechanism is damage to the alveolar wall or capillaries • Acute restrictive disease • Pt becomes acutely hypoxemic • Need PAPressures which will also help to blast the plasma proteins against the alveolar walls |
|
|
What is being pictured? What stage? What do you see on the left? What are the arrows pointing to on the right?
|
• Diffuse alveolar damage in proliferative stage
• Beginning organization (left) • Plugs of fibroblasts inside the alveoli. (right) Clinical findings: RSV-pneumonia, ARDS. S/P bone marrow transplantation 6 months ago. |
|
What is being shown on the left? What stage? What is shown on the right? What are the arrows pointing to?
|
• Diffuse alveolar damage in proliferative stage with beginning organization (left)
• Plugs of fibroblasts inside the alveoli (arrows, right) Clinical findings: RSV-pneumonia, ARDS. S/P bone marrow transplantation 6 months ago. Stain: HE. RIGHT: Elastic van Gieson. |
|

What is pictured? What stage?
|
DAD (ARDs)
Organizing stage |
|
What is pictured? What is special about this disease? What is pathologic about the pleura?
|
• Silicosis.
• ***Silicosis is currently the most prevalent chronic occupational fibrogenic dust-related disease*** • Pleura is thickened Description: Silicotic nodules. Additional findings: Up to 5mm palpable gray-white nodules and star shaped scars in the apical portion of the lung. Clinical findings: The specimen is from the lung of a construction worker. |
|
What is pictured? WHat are the white spots?
|
• Silicosis
• Crystalline material Diagnosis: Silicosis. Description: Silicotic nodule composed of fibroblasts and macrophages contains bi-refringent crystalline material and carbon. Additional findings: Grossly up to 5mm palpable gray-white nodules and star-shaped scars are located in the apices of both upper lobes. Clinical findings: The specimen is from the lungs of a construction worker. StainHE. |
|
What is pictured on the left? On the right? What is significant about the white space on the right?
|
LEFT:: Anthracosilicosis. Description: Anthracotic grey-black silicotic granuloma. Mixed dust pneumoconiosis.
RIGHT: Anthracosilicotic nodule. ****Note traction emphysema around the fibrotic nodule.*** |
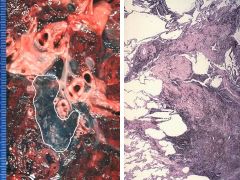
|

What is pictured? What is circled on the right?
|
Asbestosis, pleural plaques
• Can see the calcified pleural plaque more prominent in the diaphragmatic pleura (circle) |
|

What is pictured?
|
Asbestos body. Being eaten (unsuccessfully) by a macrphage.
Description: Club-shaped asbestos body with a central asbestos fiber, which is coated with iron. Macrophages are trying to phagocytose the asbestos fiber/asbestos body and ***die trying releasing growth factors that stimulate fibroblast proliferaton.*** |
|

What is being shown? What is on the Right?
|
Pleural plaques of asbesosis
• Dense fibrous tissue of the pleural plaques |
|
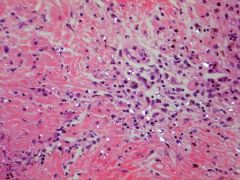
What is being shown? Why is a history important? What is the circle indicating?
|
Granulomatous inflammation of hypersensitivity pneumonitis
• Hx important because often workplace associated • Circle indicating poorly formed granulomas w/ multinucleated giant cells in alveolar walls |
|
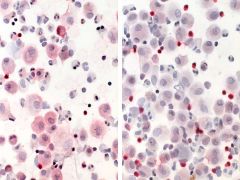
What is being shown? What type of sample? The left is showing a CD4 stain and the rights a CD8 stain. Why is this important?
|
• Hypersensitivity pneumonitis
• Broncholavage • On the immunostained BAL samples fewer T cells are positive for CD4. Additional findings: T-Helper cells (CD4) 29%, T-Suppressor cells (CD8) = 83%, Helper / suppressor ratio is 0.35. ***In sarcoidosis the CD4 count would be higher Clinical findings: Chronic cough. |
|

What is being shown? What is notable around the carina?
|
Granulomatous inflammation of sarcoidosis.
• See perihilar lymphadenopathy |
|
|
What is being shown? Where are the nodules presenting?
|
Sarcoidosis
• Confluent granulomas in typical peri- broncho- vascular distribution |
|
What is being shown? Where are the nodules forming?
|
Sarcoidosis
• Confluent granulomas in typical peri-broncho-vascular distribution |
|
What disease is being shown? What is distinctive about the granulomas shown?
|
Sarcoidosis
• Non-caseating granulomas (classic, w/ fibrosis) |
|
What is being shown? What are the arrows indicating? What is the circle on the left showing?
|
• Idiopathic pulmonary fibrosis (IPF), aka usual interstitial pneumonia (UIP).
• Atypical alveolar lining cells (arrows) • Alveolitis (circle) Description: Prominent interstitial fibrosis accompanied by sparse mononuclear inflammatory infiltrates. Irregular air spaces are lined by **reactive bronchiolar and type II cells with nuclear atypia**, which may be incorrectly interpreted as malignancy. Note: Lesions of varying ages ranging from patchy alveolitis with variable degree of organization to dense fibrosis are typical in UIP. |
|
What process is being shown? What does the bottom right show?
|
UIP (IPF) The process of remodeling of the lung.
• Bottom right shows honeycombing. |
|
What is being shown? What are the circles indicating? What is significant about these lesions?
|
Idiopathic pulmonary fibrosis (Cryptogenic organizing pneumonia)
• Circles are indicating plugs of PMSNs + young fibroblasts (Masson bodies) fill the alveoli • ****All lesions appear to be of the same age***** Comment The diagnosis of idiopathic organizing pneumonia can only be made after careful consideration of both clinical and radiologic findings. The following possibilities should be excluded first: Infection, organizing DAD, bronchial obstruction, aspiration pneumonia, hypersensitivity pneumonia, drug reaction, toxic gas, bone marrow, lung or heart-lung transplantation. |
|

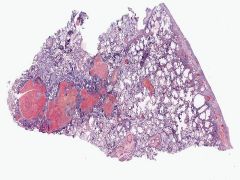
What is pictured here? What is a sequelae?
|
End-stage honey comb lung
• Cor pulmonale and pulmonary embolus |
|
What is pictured here? What is a sequelae? What is significant about the sub-pleural region?
|
End-stage lung (honeycomb) due to UIP
• Cor pulmonale & PE • More pronounced fibrosis in the subpleural region. No normal alveoli are left in this lung. |
|
What is being pictured? What is this the earliest manifestation of? How can you detect this? What is the circle indicating?
|
Respiratory bronchiolitis
• ****Earliest manifestation of COPD**** usually very few accompanying symptoms. • Could be detected by ***FEF 25-75**** • Pigment containing macrophgaes (circle) |
|
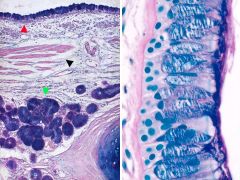
What is being pictured? What is the red arrow pointing to? Black arrow? Green arrow? Normally how do these cells relate to each other (ratio)?
|
• Goblet cell hyperplasia (red)
• Hypertrophic smooth muscel (black) • Mucous gland hypertrophy (green) • Normal goblet:ciliated cell = 1:5 to 1:20 Diagnosis: COPD, mucus gland hypertrophy, goblet cell hyperplasia. Description: Prominent goblet cell increase in bronchial epithelium. • Goblet cell hyperplasia is most often seen in chronic bronchitis or asthma. It can also occur in the drainage area of tumors or tuberculous cavities. Stain: Alcian Blue-PAS. |
|
What is being shown? What is shown on the right? What cell type?
|
Chronic bronchitis w/ acute exacerbation
• Chronic inflammation on the right w/ PMNs |
|
What is pictured? What are the arrows indicating? What is shown on the right?
|
Bronchiectasis in COPD. • Diameter of peripheral bronchus is greater than that of its accompanying artery. (arrows)
• Histology: Acute and chronic inflammation, edema and hyperemia (accompanying acute inflammation) in bronchial wall. Thick basement membrane. |
|

What is pictured? What are the arrows indicating on the left?
What is shown under the pleura on the right? |
Chronic bronchitis, bronchiectasis & chronic pneumonia in Cystic Fibrosis
• Acute and chronic inflammation w/ scarring • Dilated pus filled bronchi (arrows) • Tenacious mucous (right) with diffusely thickened pleura |
|
What is shown?
|
Centriacinar emphysema (typical smokers emphysema)
|
|
What is being shown?
|
Centriacinar emphysema (antracosis)
|
|

What is being shown? What deficiency is likely present? What genetic component is associated?
|
Panacinar emphysema
• alpha-1 antitrypsin deficiency • PiZZ (homozygous for Z allele is associated w/ markedly decreased serum levels of alpha-1 AT) • PiMM is normal |
|

What is shown? What deficiency? What genetic association?
|
Panacinar emphysema
- alpha-1 AT is encoded by codominantly expressed genes in the polymorphic Pi locus on chromosome 14 - PiMM (normal) is the most common genotype - 0.012% of US population is homozygous for the Z allele, PiZZ, which is associated with markedly decreased serum levels of alpha-1 AT |
|
What is being shown? What are the circles indicating? What is characteristic of the alveoli?
|
Emphysema
• Thick walled arterioles (arrows) due to increased pulmonary artery pressure and cor pulmonale, which this patient had • Alveoli are thin-walled and large |
|
What is being shown? Left? Right?
|
Liver in alpha-1 AT deficiency. • The enzyme accumulates particularly in the periportal hepatocytes and can lead to lever damage and cirrhosis. • Stain: Digested-PAS. Diastase enzyme removes glycogen; the remaining red staining is due to α-1 AT.
|
|
What is being shown? What are the 3 characteristic morphological changes?
|
Asthma
1. Thickening of the basement membrane 2. ↑ of airway smooth muscle 3. Inflammatory infiltrates and edema in bronchial wall with many eosinophils and mast cells 4. Enlarged mucus glands 5. Mucus plugs in airways 6. Charcot-Leyden crystals in mucus |
|
What is being shown? What are the three key morphological changes? What inflammatory cell is present?
|
Asthma
1. Thickening of the basement membrane 2. Increase of airway smooth muscle 3. Inflammatory infiltrates and edema in bronchial wall with many ***eosinophils and mast cells*** 4. Enlarged mucus glands 5. Mucus plugs in airways 6. Charcot-Leyden crystals in mucus |
|
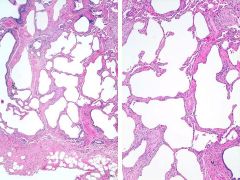
What is being shown on the left? What is on the right? What is the distinguishing factor?
|
• Emphysema on the left (Obstructive)
• Interstital Pneumonitis Fibrosis (UIP) (Restrictive) --> honeycomb lung • ***Distinguishing factor is the thickness of the alveolar walls*** |
|
What is being shown? Why is this concerning?
|
• Atypia - dysplasia in the bronchus (Whitis, thickened patches)
• May progress to carcinoma in-stiu if the following characteristics appear: --Disturbed cellular polarity --Increased N:C --Nuclear hyperchromatism --Anisonucleosis --Nuclear pleomorphism --Increased mitoses --No invasion |
|
What is being shown?
|
Epithelial changes leading to squamous cell carcinoma
|
|
What is being shown? First arrow? second arrow? Third (double arrow)?
|
• Metaplasia (lower arrow)
• Dysplasia (second arrow) • Carcinoma in situ |
|
What is being shown?
What does the purple circle indicate? What does the orange circle indicate? What is the arrow pointing to? Why is this important? |
Carinoma in situ
• Intracellular keratin production (pink inside the cell) [purple circle] • Nuclei are abnormally enlarged, they are hyperchormatic, there is loss of polarity. They vary in size and shape (anisonucleosis) [orange circle] • Basement membrane is intact (the way you can say it is a carcinoma in-situ), and the entire epithelium of the bronchos is cancerous [arrow] |
|

What is being shown? What symptoms may be associated with this?
|
Squamous cell carcinoma
• Associated with para-thyroid like hormone and hypercalcemia (paraneoplastic syndrome) |
|
What is being shown? What are the arrows showing? What is this indicative of?
What are symptoms that may be associated with this? |
Squamous cell carcinoma (well-differentiated)
• Arrows are pointing to cytoplasmic keratinization, keratin pearls, intercellular bridges • Indicates that the tumor is well-differentiated • Can be associated with PTH-like hormone --> hypercalcemia (paraneoplastic syndrome) |
|
What is being shown? Where in the lung does this typically occur? With what reaction does this have a relationship? What mutations are associated with this?
|
• Adenocarcinoma
• Usually in peripery, can be centrally located • Associated w/ demoplastic (scarring) reaction • Associated with KRAS & EGFR oncogene mutations * Most common primary lung tumor |
|
What is being shown? Where is it usually located? What rxn is it associated with? What mutations is it associated w/?
|
• Adenocarcinoma
• Usually in peripery, can be centrally located • Associated w/ demoplastic (scarring) reaction • Associated with KRAS & EGFR oncogene mutations |
|
What is being shown? What part of the lung is it typical?
|
Bronchiolo-alveolar carcinoma (subset of adenocarcinoma)
• Arises in the terminal bronchioles and alveoli • Typically peripheral gray-white nodules • May appear as a single nodule or resemble pneumonia or TB both in chest films and grossly • “Lepidic” growth pattern is a typical feature (tumor cells grow along existing alveolar walls) • May produce copious ***mucin*** |
|
What is shown?
|
Large cell carcinoma
|
|
What is being shown? What is not present on the left? What are the arrows pointing to on the right?
|
Large cell carcinoma
• No keratin (not squamous) no glands (not adenocarcinoma) • Arrows show tumor in lymphatics |
|

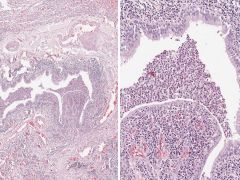
What is shown? What is it origin? What is concerning?
What markers is it associated with? What is a key histological feature? What syndromes are it associated with? |
Small cell carcinoma
• Neuroendocrine origin • Metastasizes early and widely; bone marrow metastases common and often present at the time of diagnosis Markers: • Diagnosis: – Morphology – • chromogranin, • synaptophysin • CD57 Features: Scant cytoplasm, granular chromatin, nuclear molding • Invasion and obstruction of superior vena cava is common leading to superior vena cava syndrome • Produces ACTH, ADH, Gastrin-releasing peptide, calcitonin leading to many paraneoplastic syndromes |
|
What is shown? Is it concerning?
What are markers? Key features? And associted syndromes? |
Small cell carcinoma
• Neuroendocrine origin • Metastasizes early and widely; bone marrow metastases common and often present at the time of diagnosis Markers: • chromogranin, • synaptophysin • CD57 Features: Scant cytoplasm, granular chromatin, nuclear molding • Invasion and obstruction of superior vena cava is common leading to ***superior vena cava syndrome*** • Produces ACTH, ADH, Gastrin-releasing peptide, calcitonin leading to many paraneoplastic syndromes |
|
What is being shown? What are some of the characteristics?
|
Carcinoid tumor
- Endobronchial polypoid obstructing mass or mucosal plaque (collar- button lesion) - Well demarcated - May cause atelectasis - Bleeds easily - metastasizes to hilar lymphnodes - nests of uniform cells that have "salt & pepper chromatin" - |
|
What is being shown? What are key characteristics?
|
Carcinoid tumor
- Endobronchial polypoid obstructing mass or mucosal plaque (collar- button lesion) - Well demarcated - May cause atelectasis - Bleeds easily - metastasizes to hilar lymphnodes - nests of uniform cells that have "salt & pepper chromatin" |
|
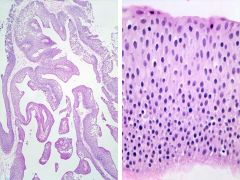
What is being shown? How can you tell?
|
• Normal urothelium.
• Epithelium is less than 7 cell layers thick. Nuclei are uniform with finely granular chromatin, Nucleoli are indistinct. The cells of the topmost layer (umbrella cells) have larger nuclei and lie parallel with the basement membrane. Stain: H&E. |
|
What is being shwon?
|
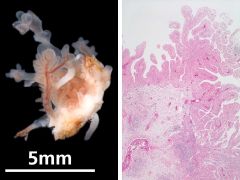
Benign papilloma of the bladder
|
|
What is being shown? How do yo know?
|
Benign papilloma.
• < 7 cells thick, no atypia |
|
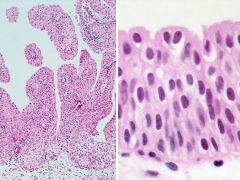
What is being shown? How do you know?
|
• Low-grade urothelial carcinoma
• Epithelium > 7 cells thick Papillary urothelial cell carcinoma. Description: The tumor is composed of papillary fronds of thickened urothelium resting on fibro-vascular cores. There is no invasion through the basement membrane. Clinical findings: **Macrohematuria** Papillary tumor noted on the posterior wall of the bladder on cystoscopy |
|
What is being shown? What is significant?
|
• Moderately differentiated TCC of the urinary bladder with muscle invasion.
Description: Solid tumor masses infiltrate the smooth muscle of the bladder wall. There is a prominent desmoplastic reaction. Clinical findings: Macrohematuria. Exophytic tumor in bladder wall. Recurring papillary urothelial tumors for 18 years. Stain: H&E. |
|
What is shown? What is the circle indicating? What is a common mutation that is associated? What does that mean?
|
High-grade papillary TCC of the urinary bladder w/ stromal invasion and necrosis (circle)
• p53 mutation means high risk of progression. |
|
What is pictured? What is indicated in the box? What mutations are associated?
|
• Clear cell carcinoma
• ***Renal vein invasion*** • Familial type has autosomal dominant von Hippel-Lindau disease with germ-line mutation in VHL gene on chromosome 3p25 ****The VHL protein limits the angiogenic response to hypoxia and acts a tumor suppressor**** |
|
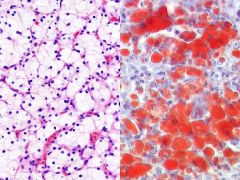
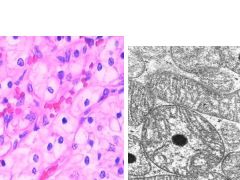
What is being shown? What stain on the right? What does it tend to invade? What mutation is associated?
|
• Clear cell carcinoma
• Oil red O - stains fat • Tends to invade renal vein • Familial type has autosomal dominant von Hippel-Lindau disease with germ-line mutation in VHL gene on chromosome 3p25 ****The VHL protein limits the angiogenic response to hypoxia and acts a tumor suppressor**** |
|

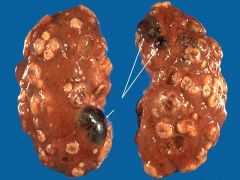
What is being shown? How are these found? What demographic is affected? What is the prognosis?
|
Wilms tumor
• Usually found on palpation • Children • 10% are bilateral or multicentric • Good prognosis: 2-year survival up to 90% even for tumors that have spread outside the kidney |
|
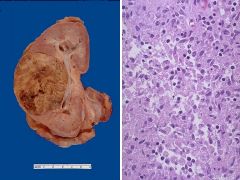
What is pictured? What is significant about the cells on the right vs. the left? What demographic does this affect?
|
Wilms tumor
• Can identify tubules (left) good prognosis, anaplasia (right) poor prognosis • Children • 10% are bilateral or multicentric • Good prognosis: 2-year survival up to 90% even for tumors that have spread outside the kidney |
|

What is shown?? What is typical of the cells?
|
• Renal oncocytoma
• Large cells with abundant eosinophilic granular cytoplasm |
|
What is shown? What is characteristic of the cells? What is significant of the cells on the right?
|
• Renal oncocytoma
• Large cells with abundant eosinophilic granular cytoplasm • Tumor cells are packed w/ mitochondria (right) |
|
What is shown? What do they stain positive for?
|
• Angiomyolipoma.
• The spindle cells show focal positivity for HMB-45 and are strongly positive for SM-Actin. • Up to 50% of angiomyolipomas are seen in association with patients who have tuberous sclerosis. |
|
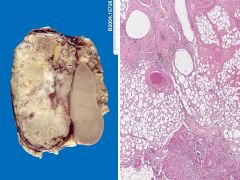
What is shown? What causes it? What is shown on the right?
|
Tumor-like lesion:
Xanthogranulomatous pyelonephritis Sometimes long-standing renal infection may be localized and form a mass-like lesion. This is a disease known as xanthogranulomatous pyelonephritis (**chronic necrotizing inflammation**). It is uncommon, but may mimic a neoplasm. Right: The microscopic appearance of xanthogranulomatous pyelonephritis shows many pale to foamy macrophages from breakdown of renal parenchyma with ongoing inflammation. |
|
What is being shown? What are the arrows pointing to?
|
Metastatic lung cancer to the kidneys
• Benign cysts (arrows) • Metastatic tumors are far more common than 1º tumors in the kidney |
|

If a PE is attached to the vessel wall (as shown), what kind of tissue will be seen in the attachment? What factors will fibroblasts release?
|
• Granulation tissue
• VEG-F |
|

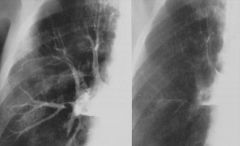
What is the cause of the indicated "Hampton's hump"? Why is it shaped that way?
|
• Hamptons hump is caused by a Pulmonary Embolus.
• Blockage of blood flow causes edema and alveoli get filled with blood (blood vessels there hemmorhage). Why is it a wedge shaped area pointing towards the hylum? • The vessel that is blocked off is in the hyla and the blood is backing up behind it. |
|
What is being shown? What type of image?
|
Angiogram depicting a Pulmonary embolus
|
|
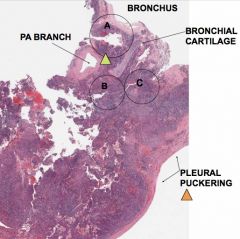
What is shown? What is the orange arrow indicating? Why is this significant/what is it the result of?
|
Bronchogenic carcinoma
• Pleural puckering • Due to the pulling of the tumor on the basement membrane **Desmosome rxn** |
|
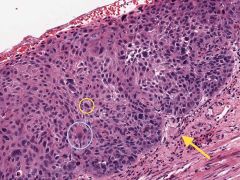
What is shown? How can you tell? What is indicated in the rectangle?
Is it invasive? How can you tell? What cells do you see surrounding? What structure is nearby? |
Carcinoma in situ.
• Cells > 7 layers thick • Rectangle shows: Extensive atypical squamous metaplasia. **Extremely large nuclei** Not invasive • Basement membrane intact Host response: lymphocytes (chronic inflammatory response) |
|
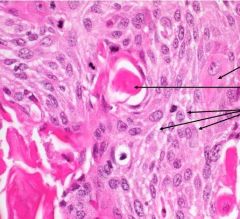
What is the Ddx? What is shown in the circle? What cells are surrounding it (arrow)? Why? What is the prognosis?
|
• Squamous cell carinoma
• Keratin pearls • Necrotic cells because of lack of oxygen • The prognosis is not dire, b/c it is a well differentiated cancer mne: skin is squamous cells --> skin requires a lot of keratin (that is what we slough off) --> squamous cell cancer makes keratin pearls |
|
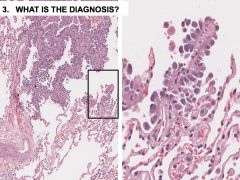
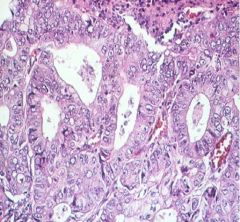
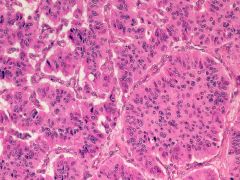
What is the diagnosis? How do you describe the growth pattern?
What type of cancer is this? Where does it tend to occur? What is a key characteristic of it? |
Bronchioalveolar carcinoma
• Lepdic growth pattern (like alighting butterflies) • A subtype of adenocarcinoma • tends to occur in the peripheral parts of the lung (terminal bronchiloles) • ****The key feature of BACs is their growth along preexisting structures and preservation of alveolar architecture**** |
|
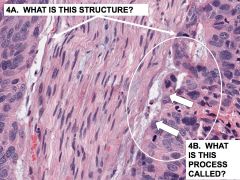
What structure is shown? What is the process called? What symptoms would this likely cause?
|
• Nerve
• Perineural invasion by bronchogenic carcinoma • This is the cause of the patient's pain! The nerve is being invaded and that's why there radiating pain. |
|
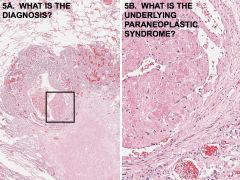
What is the diagnosis? What is the underlying paraneoplastic syndrome? What type of cancer is most like to cause this? What other syndromes could occur?
|
• Pulmonary thromboembolism
• Hypercoagability • Adenocarcinoma • also associated with hematologic manifestations, including migratory thrombophlebitis, nonbacterial endocarditis, and disseminated intravascular coagulation |
|

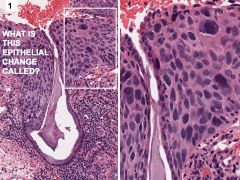
What is this epithelial change called?
• What is the arrow indicating? • What is the purple circle indicating? • What is the green circle indicating? |
Carcinoma in-situ
• Basement membrane is intact (carcinoma in-situ), and the entire epithelium of the bronchos is cancerous. Underlying stroma is fibrotic and has ***chronic inflammatory cells*** (arrow) • Nuclei are abnormally enlarged, they are hyperchormatic, there is loss of polarity. They vary in size and shape (anisonucleosis) (purple) • Intracellular keratin production (pink inside the cell) (green) |
|
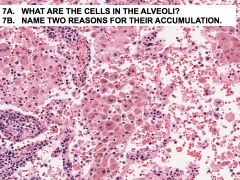
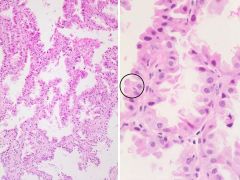
What are the cells in the alveoli? Why are they accumulating there? What do the cells contain? What is a sequelae of there presence?
|
• Macrophages
• Obstruction, healing pneumonia. [Other reasons: hemorrhage, inhalation of foreign material. In desquamative interstitial pneumonia (DIP) tobacco smoke appears to be the precipitating factor.] • Macrophages some of which that contain hemosiderin. • Also have a foamy appearance because they have phagocytosed fat --> Lipopneumonia ****Golden pneumonia*** |
|
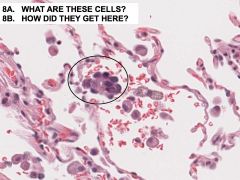
What are these cells? What type of cancer is this? How did they get there?
Normally, where would these cancer cells be found? What is a key characteristic of this cancer? |
• Bronchioaveolar cancer cells (Adenocarcinoma)
• Aerogenic spread • Normally found in the periphery (in lepidic grown patterns) *****The key feature of BACs is their growth along preexisting structures and preservation of alveolar architecture***** |
|
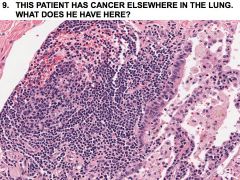
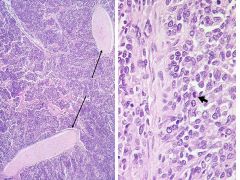
The patient was a 63-year-old man, who smoked 1-2 packs of cigarettes a day since he was 14 years old. He came to see his primary care physician because he was coughing more than usually and lately the sputum has been blood-streaked. He denied weight loss and any symptoms other than the cough. A chest film revealed a 3.5 cm poorly demarcated mass in the right lower lobe adjacent, but not continuous with the hilus. Lymph node biopsy obtained at mediastinoscopy was negative for tumor. The specimen is from the right lower lobe lobectomy specimen.
What type of cancer may this be according to the case? What other infection does he have? How do you know? |
• Squamous cell carcinoma
• Chronic bronchitis • Inflammatory cells |
|
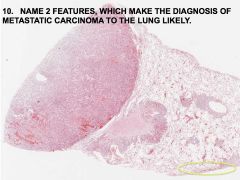
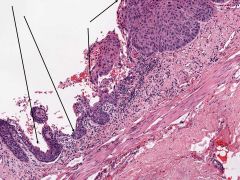
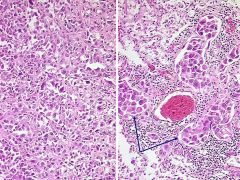
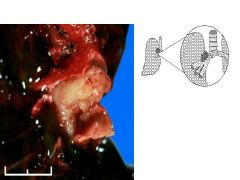
What are two features that make diagnosis of metastatic carcinoma likely?
What is the green circle showing? How did the tumor start to invade the lung? What kind of tumor might this have been? What complication is also seen? |
• 1. Multifocal tumor 2. Distribution in the subplerual & peribronchovascular lymphatics
• Showing metastases to lymphatics, growth outside of lymphatics and desmoplastic rxn (Tumor requires a fibrous foundation - stimulates the fibroblasts. Analogous to angiogenesis) [green circle] • Lymphatic & Hemotogenous spread • Pheochromocytoma • Paraneoplastic syndrome: Hypercoagulability (shown by platelets, fibrin and PE accumulating) |