![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
38 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
1. What is the sensitivity, specificity and accuracy of FNA diagnosis of malignancies in the liver? (generally percutaneous, CT, US or MRI guided) 2. What 3 liver lesions have been misdiagnosed as malignant? 3. What features of transplant rejection can be seen on FNA? |
1. sensitivity: 71-94% specificity: 87-100% accuracy: 90-94% False positives very uncommon 2. hepatic dysplasia, FNH, Bile duct hamartoma 3. activated lymphocytes (enlargement, "blast" forms), hepatocyte injury (swelling, vacuolization, necrosis) and cholestasis |
|
|
|
1. List 3 risks associated with FNA? 2. List FNA locations where hepatocytes may be inadvertantly sampled. 3. What are the components of a normal liver aspirate? |
1. tumor seeding (0.1-0.6%) recurrent HCC after transplant Death (mortality 0.6%) 2. pancrease, right kidney, right adrenal, right lower lobe lung 3. hepatocytes, bile duct epithelium, kupffer cells and sheets of mesothelial cells |
|
|
|
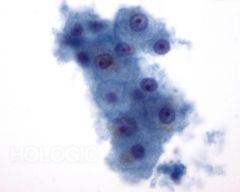
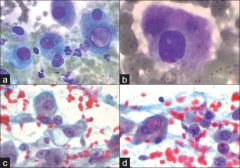
Normal hepatocytes with aging pigment 1. What is the cytomorphology? |
1. large polygonal cells isolated, thin ribbons (trabeculae) OR tissue fragments central, round/oval variably sized nuclei binucleation common prominent nucleolus intranuclear pseudoinclusions abundant granular cytoplasm lipofuscin pigment ( common; golden on pap and green-brown on romanowski) hemosiderin (UNcommon may represent iron metabolism disorder; dark brown on pap and blue on romanowsky) bile (in cholestasis; dark green on pap and romanowsky, maybe black) |
|
|
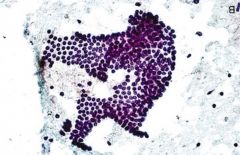
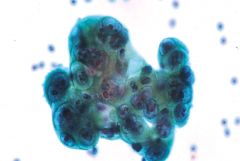
normal bile duct epithelium
1. What is the cytomorphology? 2. What is the cytomorphology of Kupfer cells? 3. What is the DDX of normal hepatocytes? |
1. cohesive flat sheets cuboidal cells smaller than hepatocytes evenly spaced nuclei (honeycomb) 2. resemble macrophages vacuolated cytoplasm +/- pigment (usually hemosiderin) 3. hepatic adenoma Focal nodular hyperplasia (FNH) regenerative nodule in cirrhosis nodular regenerative hyperplasia steatosis |
|
|
1. List causes of steatosis. |
1. alcohol diabetes obesity drugs (e.g. methotrexate) TPN post jejunoileal bypass surgery hepatitis C |
|
|
|
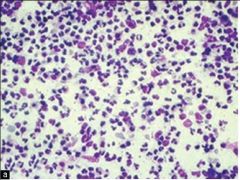
hepatic abscess 1. What are three causes? list common examples. 2. What is the cytomorphology of the first two? |
1. bacterial: Streptococci, staphylococci and enteric bacteria result from ascending cholangitis fungal: Candida in immunocompromised patients amoeba: E. histolytica 2. abundant neutrophils and necrotic debris +/- bacteria/fungi on routine stains (special stains and culture are helpful) |
|
|
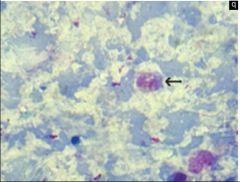
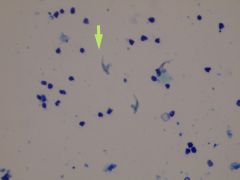
amoeba with necrosis 1. Usually due to what organism? (seen in this photo) 2. Sequela from what ? 3. What is the cytomorphology? |
1. Entomoeba histolytica 2. colon infection 3. macroscopic anchovy paste necrotic debris little if any acute inflammation amebic trophozoites resembling histiocytes (round nucleus, peripheral chromatin marginization, abundant ovoid cytoplasm containing ingested RBCs) |
|
|
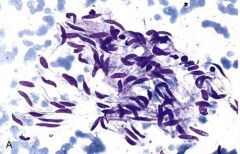
1. What are these? Name the causative organism. 2. How common is the above infection? 3. Where is this endemic? 4. What is the cytomorphology? 5. What is a classic but uncommon complication of FNA of these cysts? 6. List 3 other parasitic diseases manifesting with liver masses. |
1. hooklets! from Echinococcus granulosus 2. accounts for 10% of of hepatic cysts >4cm in diameter 3. countries bordering the mediterranean and baltic seas, south america, australia and new zealand 4. fragments of laminated membrane (that lines cyst) scolices hooklets 5. anaphylactic shock 6. schistosomiasis chlonorchiasis visceral larva migrans |
|
|
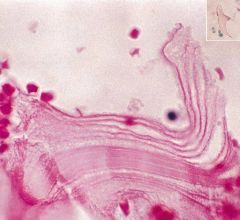
Laminated membranes 1. Describe these? 2. Describe hooklets and how they stain on pap. 3. What conditions cause granulomas in the liver? 4. What tumor mimics granulomas? Describe. |
1. parallel acellular striations which are dianostic! 2. pale daggerlike do NOT stain on pap! 3. miliary TB sarcoidosis PBC Hodgkin drug reactions 4. Angiomyolipoma; the myoid cells have a syncytium like appearance like epithelioid histocytes but also adipocytes and extramedullary hematopoesis |
|
|
1. What cyst is lined by cells resembling respiratory epithelium? Describe cytomorphology. 2. What is in the DDX? |
1. ciliated foregut cyst: ciliated columnar cells and mucus cells 2. bile duct cystadenoma bile duct cystadenocarcinoma |
|
|
|
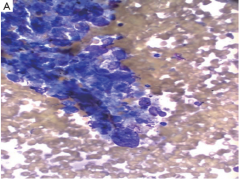
cirrhosis 1. What is the cytomorphology? 2. What is the DDX? |
1. normal hepatocytes +/- steatosis focal atypia (marked nuclear size variation, prominent nucleolus, binucleation; and other sites said fragments of fibrotic tissue as seen in photo) 2. HCC hepatic adenoma FNH normal liver nodular regenerative hyperplasia |
|
|
1. What is the cause of FNH? 2. What is the patient population and prognosis? 3. What is the cytomorphology? 4. What is the DDX? 5. What is the characteristic radiologic and histologic appearance? |
1. unknown but possibly vascuolpathy 2. it's benign! occurring as a solitary mass in women in 3-4th decades 3. hepatocytes without atypia normal trabeculae (2 cells thick) +/- steatosis bile ductular cells 4. hepatic adenoma regenerating nodule in cirrhosis normal liver 5. central scar, with nodules of hepatocytes separated by radiating fibrous septae containing bile ductules |
|
|
|
1. How are hepatic adenoma, FNH and cirrhosis differentiated on cytology? 2. What are the usual hepatocyte markers (positive in FNH)? 3. In the context of suspected FNH on radiology what finding can "exclude" an adenoma? 4. Why is it important to differentiate the above? |
1. They aren't! Cytologically indistinguishable requiring radiologic and clinical correlation 2. HepPar1, TTF-1 cytoplasmic, arginase1 and cam5.2, canalicular pCEA 3. bile ducts (absent in adenoma) 4. hepatic adenomas carry a risk of life threatening hemorrhage and ar linked to HCC |
|
|
|
1. What stains can be used to differentiate FNH from adenoma? 2. What is the patient population for hepatic adenoma? 3. What is the characteristic histology? |
1. glutamine synthetase (map like staining in FNH), liver fatty acid-binding protein, serum amyloid A OR C-reactive protein, and beta-catenin 2. women <30 with history of long term oral contraceptives 3. composed entirely of hepatocytes lacking portal triads with scattered "naked" arterioles (characteristic) |
|
|
|
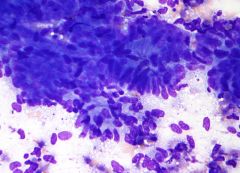
hepatic adenoma 1. What is the cytomorphology? 2. What is the DDX? 3. What markers does this share with FNH? 4. How is HCC distinguished from adenoma? |
1. normal hepatocytes +\- steatosis normal trabeculae (2 cells thick) naked arterioles (cell block and biopsy) 2. normal liver FNH regenerating nodule in cirrhosis HCC 3. all markers of hepatocellular differentiation 4. HCC cells have higher N:C ratios and more architectural derangment |
|
|
1.Bile duct hamartomas AKA? 2. What is the gross/histologic appearance? 3. What is the gross appearance of the related lesion bile duct adenoma? 4. What is the cytomorphology that these two lesions share? |
1. von Myenberg complex 2. multiple small nodules dispersed throughout liver composed of haphazardly arranged bile ductules and fibrous stroma 3. <1cm solitary subcapsular 4. hypocellular benign ductal cells in tubules and cohesive sheets benign hepatocytes |
|
|
|
Hemangioma 1. How common is this? 2. What are the most commonly encountered spindled lesions in the liver? 3. What is the cytomorphology? |
1. THE most common benign liver tumor 2. hemangioma > metastatic GIST > metastatic leiomyosarcoma > granulomatous hepatitis 3. blood only (sometimes) heaptocytes only (sometimes) 3D arcades and compact, dense coils of bland elongated spindle cells rare isolated spindle-shaped cells vascular channels lined by endothelial cells (cell block) |
|
|
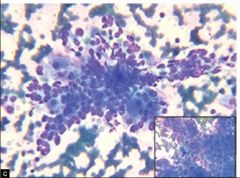
Angiomyolipoma 1. Where does this tumor most commonly occur? 2. What is the average age of diagnosis? associated syndrome? 3. What feature is readily recognized on CT/MRI that precludes FNA diagnosis? 4. What is the stain in the photo? why is this relevant? 5. How common is EMH in these? |
1. kidney>>> liver (100 reported worldwide) 2. 50 years (60% symptomatic the rest found incidentally) tuberous sclerosis 3. FAT 4. smooth muscle actin (staining myoid component); this component is the only specific diagnostic component (unlike fat and vessels that complete the triad) 5. 40% which is much more than the renal version |
|
|
1. What stain is a helpful diagnostic feature of AML? 2. What is the DDX of hepatic AML? 3. Why are is the DDX broad? |
1. HMB45 and melan-A (MART1) which is positive in the myoid cells 2. HCC carcinomas granulomatous inflammation myelolipoma nodular hematopoesis sarcoma 3. because the myoid cells vary in in appearance from epithelioid to spindled with indistinct cell membranes (syncitium) and be markedly pleomorphic with bizarre giant cells! |
|
|
|
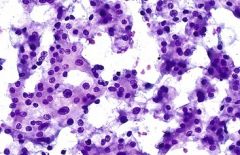
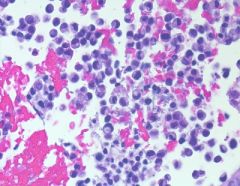
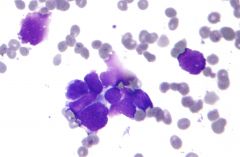
HCC 1. How common is this? 2. AFP>? is highly suggestive? 3. What are the 3 architectural patterns seen in classical HCC? 4. List 4 cytoplasmic inclusions seen in this tumor? 5. List 5 special (non-classical) types of HCC. |
1. 90% of all primary cancers of the liver!!!! (Africa & Asia > USA and Europe) 2. >4000 3. trabecular, pseudoglandular (acinar) and compact 4. mallory hyaline bodies, globular hyaline bodies, pale bodies and ground glass 5. fibrolamellar, scirrhous, undifferentiated, lymphoepithelioma-like and sarcomatoid |
|
|
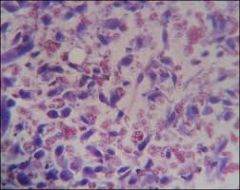
1. What is the cytomorphology of well-moderately differentiated HCC? 2. What is the DDX of the above? 3. What stain is positive in HCC and negative in benign hepatocytes? |
1. highly cellular polygonal isolated cells with moderate to abundant cytoplasm many large naked nuclei thickened cell cords (trabeculae) wrapped in endothelial cells pseudoglandular/acinar structures transgressing vessels increased N:C ratio large, central round nucleus with prominent nucleolus +/- pseudoinclusions intracellular bile 2. Regenerating nodule in cirrhosis hepatic adenoma FNH 3. Glypican-3 |
|
|
|
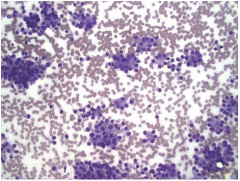
1. What is the cytomorphology of poorly differentiated HCC? 2. What is the DDX? 3. Which tumors do the clear cell and fatty change variants of HCC mimic? 4. What is the difference in staining pattern of pCEA in HCC versus ACA? 5. What stains kupfer cells and what is their appearance? |
1. highly cellullar isolated cells or clusters moderate to marked pleomorphism atypical mitoses spindle shaped cells tumor giant cells bile 2. cholangiocarcinoma metastatic carcinoma 3. renal, adrenal and germ cell 4. HCC: linear pattern outlining bile canaliculi ACA: diffuse cytoplasmic 5. vimentin, spider-shaped, not seen in ACA |
|
|
Fibrolamellar HCC 1. What is the unusual clinical presentation? 2. What is the cytomorphology? 3. How do this and pediatric HCC stain differently than adult HCC? |
1. young patients mid20s NOT cirrhotic, favorable prognosis 2. large cells (bigger than HCC and normal hepatocytes) abundant granular cytoplasm large nucleus prominent nucleolus isolated or loose clusters intracytoplasmic hyaline globules bands of fibrosis separating neoplastic cells (histology) 3. more likely to be CK7+ than adult HCC |
|
|
1. What is the staining pattern of TTF-1, pCEA, HepPar1 and arginase in HCC? 2. What is the second most common primary hepatic malignancy? 3. What are risk factor for the above? |
1. TTF1: cytoplasmic pCEA: canalicular HepPar1: cytoplasmic arginase: cytoplasmic +/- nuclear 2. cholangiocarcinoma 5-15% of primary liver cancers 3. primary sclerosing cholangitis, hepatolithiasis (Far East), parasite of liver Chlonorchis sinesis, nonbiliary cirrhosis, deposition of thorotrast |
|
|
|
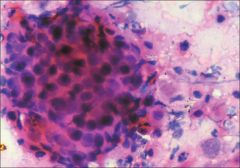
Cholangiocarcinoma 1. What is a Klatskin tumor? 2. What is the clinical presentation? 3. How is it usually diagnosed? 4. With what is peritoneal biopsy associated? 5. What is the cytomorphology? 6. What is the DDX? |
1. a cholangio arising from right or left hepatic ducts near the junction/hilum 2. extra hepatic present with obstructive jaundice, often elevated CA19.9 and CEA 3. 60-70% w/ bile cytology, biliary bush or FNA (EUS more popular) 4. incrased peritoneal metastasis 5. isolated cells, crowded sheets or clusters glandular differentiation (mucin vacuoles or acini) nuclear enlargement with variation in size and shape 6. HCC and metastatic ACA |
|
|
1. What stains are characteristic of cholangiocarcioma? 2. What is the distinction between pancreatic and cholangiocarcioma? 3. What stain pattern do the above exhibit? 4. What is hepatoblastoma and the cytologic appearance? |
1. + mucicarmine, AE1/3 CK, and diffuse cytoplasmic pCEA; also + for CK7/17/19 whereas HCC is not and is usually CK8/18+ 2. location! 3. overexpression of p53 and loss of SMAD4 4. rare tumor of infancy and childhood mimics HCC with lrager more anaplastic cells or a small round blue cell tumor of childhood |
|
|
|
Angiosarcoma 1. How common in the liver? 2. What association does it have in common with HCC? 3. With what environmental factors is it associated? 4. What is a potential complication of FNA? 5. What is the cytomorphology? 6. What is the DDX? |
1. <1% of primary hepatic malignancies 2. cirrhosis (1/3 of cases) 3. polyvinyl chloride and Thorotrasat radiographic contrast agent 4. Massive bleeding 5. well diff: elongated cells, isolated or tightly cohesive w/ syncitia poorly diff: large spindle shaped or epithelioid (very difficult to ID on FNA) pleomorphic nuclei multinucleated giant cells with rhapdoid forms in some epithelioid angiosarcomas abundant fine or coarsely vacuolated cytoplasm often with intracytoplasmic lumina cell blocs show anastomosing vascular pattern 6. epithelioid hemangioendothelioma other malignant neoplasms |
|
|
1. What is epithelioid hemangioendothelioma? 2. What is the cytomorphology? 3. What does this mimic in the lung/pleural fluid? 4. How common are metastases to the liver? 5. What are common mets? |
1. another endothelial tumor less aggressive and more rare than angiosarcoma 2. hypocellular (sometimes) with clean background isolated large polymorphous cells with folded nuclear outline fragments of metachromatic stroma frequent binucleated or multlnucleated giant cells round or irregular prominent nucleoli abundant lacy or dense cytoplasm +/- intracytoplasmic lumina 3. mesothelioma! 4. account for the majority of liver masses (usually carcinomas) 5. colorectal, lung, pancreas, stomach, and breast |
|
|
|
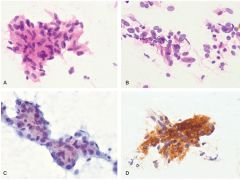
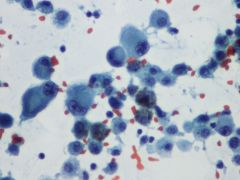
colorectal adenocarcinoma 1. What is the cytomorphology and IHC? |
1. tall columnar (picket fence) dark and "dirty" necrotic
+ CK20, CDX2 and SATB2 - CK7 |
|
|
gastric ACA 1. What is the cytomorphology? |
1. signet ring cell OR intestinal type (arises from intestinal metaplasia)
|
|
|
Breast (ductal actually) ACA 1. What is the variable cytology? 2 What is the IHC? |
1. ductal or lobular with variable differentiation, look for signet ring cells 2. + mammaglobin, GCDFP-15, estrogen an progesterone and HER2 |
|
|
Prostatic ACA 1. What is the cytomorphology and IHC? |
1. microacini with prominent nucleoli; + Prostatic acid phosphatase and PSA |
|
|
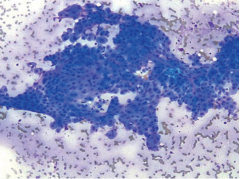
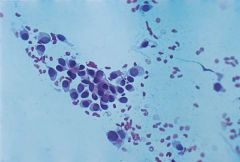
well diff. neuroendocrine tumor 1. What is the cytomorphology? 2. What is the general IHC pattern? 3. What is IHC for pancreatic origin? 4. How are neuroendocrine tumors of the GI tract and pancreas graded? |
1. eccentric nuclei, salt and pepper chromatin, abundant granular cytoplasm, isolated, loosely cohesive and rosettes 2. + synapto, chromo, CD56 3. + islet-1 and PAX8 4. by proliferative rate Low: <2mits/10HPF with Ki67<4% Intermediate :2-20 mits/10HPF with Ki673-20% High: >20mits/10HPF Ki67>20% |
|
|
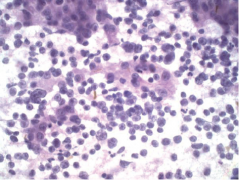
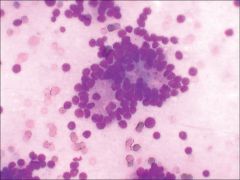
Small cell carcinoma 1. What is the cytomorphology? |
1. isolated and loosely cohesive cells nuclear molding hyperchromatic nucleus fine granular chromatin with small nucleoli round/polygonal or spindle cells?? paranuclear blue bodies |
|
|
poorly diff. SQC 1. What is the cytomorphology? 2. IHC? |
1. small dark nuclei without texture abundnat cytoplasm with hard, glassy appearance (orange on pap and gray on romanowsky) poorly diff. nonkeratinized hard to distinguish from other poorly diff malignancies 2. keratins and p63 |
|
|
melanoma 1. What is the cytomorphology?2. IHC? |
1. prominent isolated cell partter, intranuclear pseudoinclusions macronucleolus, abundant cytoplasm +/- pigment which is finely granular (bile is more variable) 2. S100 HMB45 MART1 |
|
|
sarcoma 1. What is the cytomorphology? 2. Which GI spindled tumors have a propensity to metastasize to the liver? |
1. spindle shaped round or pleomorphic 2. GIST (+ CKIT/CD117 and DOG1) |
|
|
1. What is the immunoprofile of seminomas/dysgerminomas? 2. Which are nuclear stains? |
1. + PLAP and SALL4(seen in most GCTs) OCT3/4 and NANOG (seen in these and embryonals) CD117 (cytoplasmic and membranous, not seen in any other GCTs) NEGATIVE for keratin, EMA, AFP and CEA 2. OCT3/4, NANOG and SALL4 |
|